
Abstract
Basal cell adenoma (BCA) is a rare benign salivary gland tumor accounting for only 1–2% of all salivary gland tumors. We report a case of a 50-year-old man presenting a BCA of the parotid gland. A pleomorphic adenoma was initially suspected based on radiological features and fine needle aspiration cytology findings (FNAC).
Introduction
Basal cell adenoma (BCA) is a rare benign epithelial salivary gland tumor that appears to have unique histologic features. It accounts for only 1-2 % of all salivary gland tumors. 1 We report a case of BCA of the parotid gland with review of literature.
Case report
A 50-year-old man presented to our outpatient clinic with a 9-month history of a swelling in the left parotid region. Physical examination showed a firm, non-tender and mobile mass in the left parotid region. The mass measured 5 cm × 4 cm. There were no signs of facial nerve involvement and no palpable cervical lymph nodes.
Pre-operative magnetic resonance imaging (MRI) showed a lesion located in the superficial and the deep lobes of the left parotid gland, with peripheral calcifications. The lesion was isointense on T1-weighted sequence and hyperintense on T2-weighted sequence (Figure 1). Fine needle aspiration cytology (FNAC) was performed and suggested the diagnosis of a pleomorphic adenoma. Pre-operative MRI: (a) axial T1-weighted image, (b) axial T1-weighted image with gadolinium injection, (c) axial T2-weighted image, and (d) coronal T2-weighted image.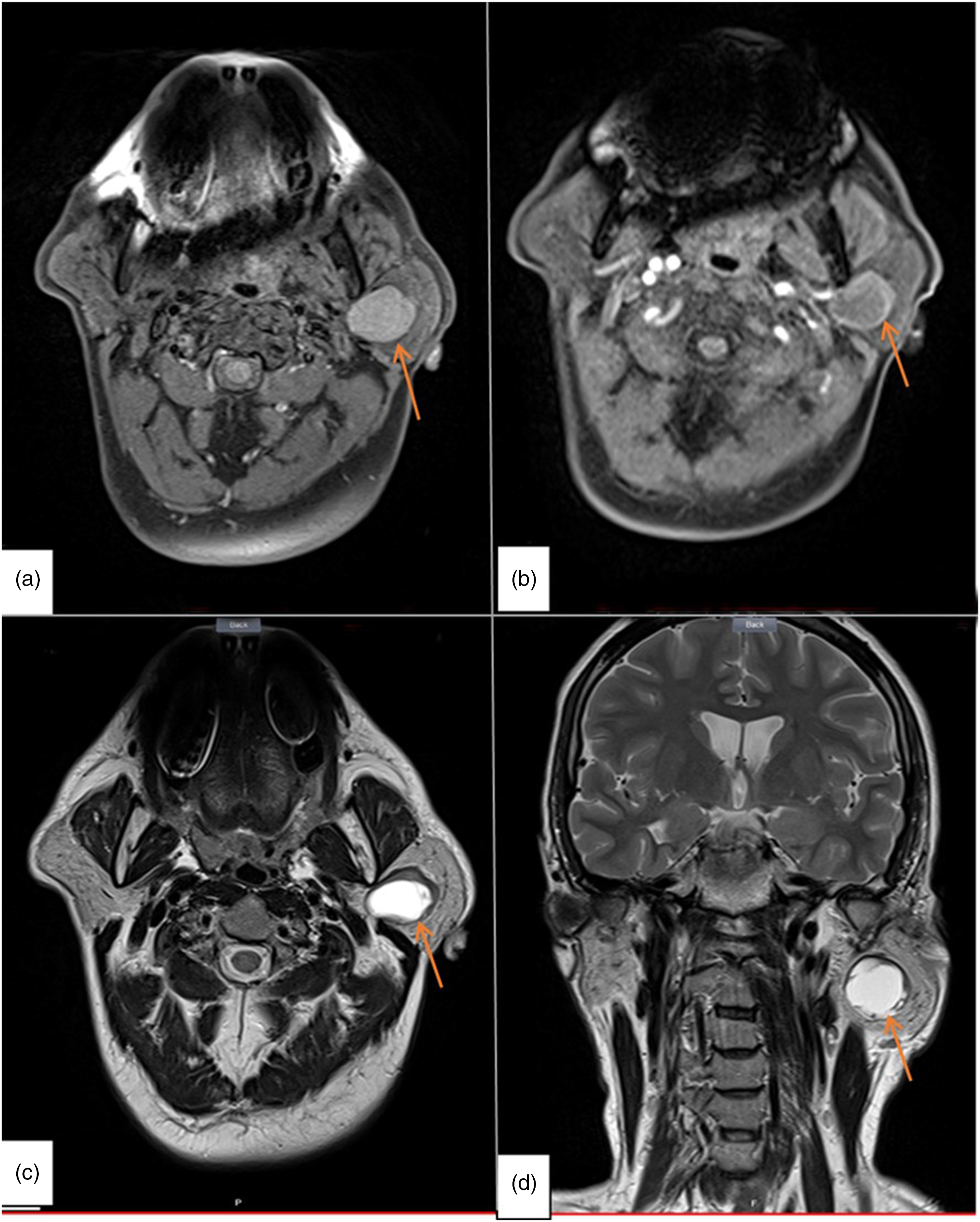
The patient underwent left superficial parotidectomy. The post-operative course was uneventful.
Macroscopically, the tumor measured 2.5 cm × 2 cm. The cut surface revealed an encapsulated whitish microcystic mass. On microscopic examination, sections showed proliferation of basaloid cells arranged in solid masses and numerous tubules. These tubules were lined with one or two layers of cuboidal and basaloid cells; the lumen often contained an eosinophilic secretion. On immunohistochemistry, tumor cells were positive for CK7 and smooth muscle actin. There was no vascular invasion, no perineural invasion, and no chondromyxoid matrix (figure2). Tubules lined with one or two layers of cuboidal and basaloid cells with no mitosis and no atypia. (a): H&E x100; (b):H&Ex 400; (c) tumor cells are positive for CK7 and smooth muscle actin (d).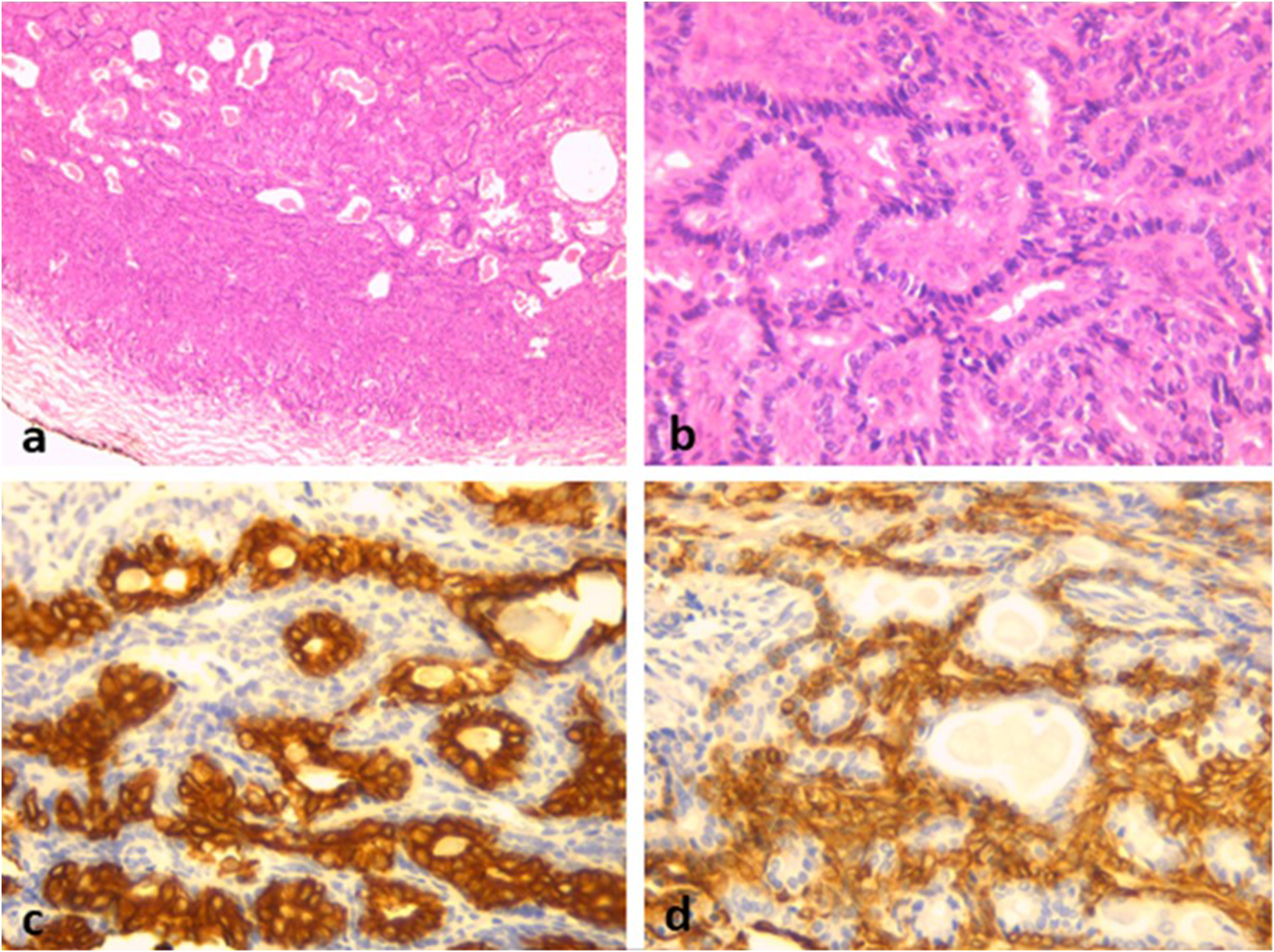
Discussion
Basal cell adenoma is a benign neoplasm developed from basaloid cells and classified as monomorphic adenoma. 2 Bernacki and al suggested that the origin of this adenoma is the intercalated duct and found that this tumor occurs mainly in the major salivary glands. 3
BCA accounts for only 1–2% of all salivary gland tumors. It mostly affects women in the fifth decade. 1,4
This tumor predominantly affects the parotid gland with an incidence approximately of 75%. 2 It can be seen, but rarely, in the accessory salivary glands and the submandibular gland. 2,5
Clinically, BCA presents as a movable firm or elastic mass that may be cystic making it indistinguishable from pleomorphic adenoma. 2,6
This tumor is encapsulated and usually measuring less than 3 cm in diameter.
It is superficially located in the parotid gland with a brownish–whitish appearance. In our case, the tumor was developed in the superficial and deep lobes of the parotid gland. 6
The World Health Organization (WHO) gives a precise definition for basal cell adenomas such as a benign neoplasm composed chiefly of basaloid cells with a prominent basal cell layer and distinct basement membrane-like structure with no myxochondroid matrix. 7
BCA has been histopathologically classified into solid, trabecular, tubular, and membranous variants. The membranous type often shows multinodular growth pattern, and recurrences are seen in nearly 25%. 8 The other types of BCAs have no recurrences. Malignant transformation is rare, more common in the membranous variant and it is about 5%. 9
The main differential diagnosis is pleomorphic adenoma because BCA may have a myxoid or hyaline stroma. 10 In addition, there are other differential diagnoses such as basal cell adenocarcinoma and adenoid cystic carcinoma. However, in BCA, mitoses are rare or absent, and there is no perineural invasion or necrosis. 10
Conventional treatment of BCA is a surgical excision: superficial or total parotidectomy. Likewise for the other locations, the treatment is the same. 11
Conclusion
BCA is an uncommon benign tumor. As BCA is a tumor that affects people over the age of 50, this leads us to think mainly of a malignant tumor arising from same location.
A well-limited lesion located in the superficial and the deep lobes of the left parotid gland, with peripheral calcifications. The lesion was isointense on T1-weighted sequence, hyperintense on T2-weighted sequence, and was enhanced after gadolinium injection. (arrow)
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.