
Abstract
Objective
Children with a history of recurrent croup alert the ENT clinician to the potential for underlying laryngotracheal pathology. There is equipoise about the likelihood of identifying any underlying structural issues or subglottic stenosis in those children who undergo airway assessment.
Methods
A retrospective cohort study in a tertiary UK paediatric hospital of a decade of children with recurrent croup who underwent a rigid laryngo-tracheo-bronchoscopy (airway endoscopy).
Main Outcome(s)
airway pathology seen on endoscopy and need for further airway surgery.
Results
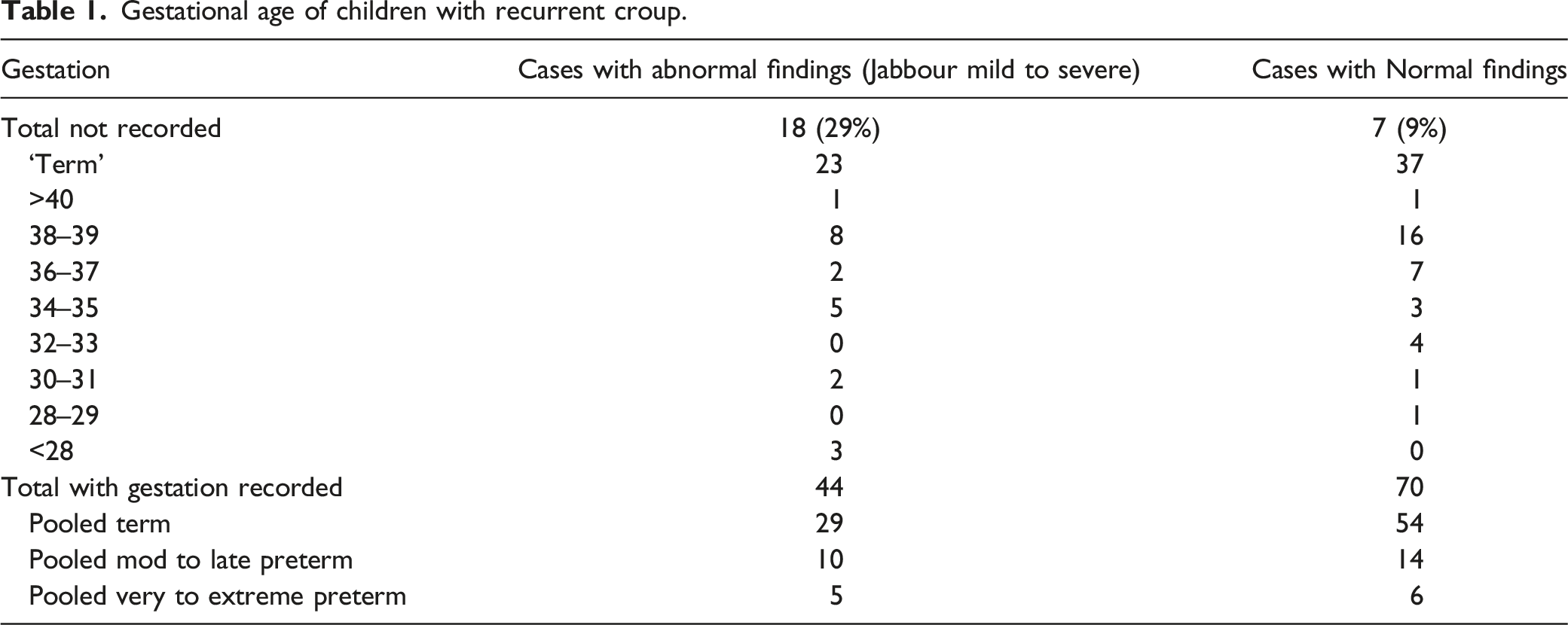
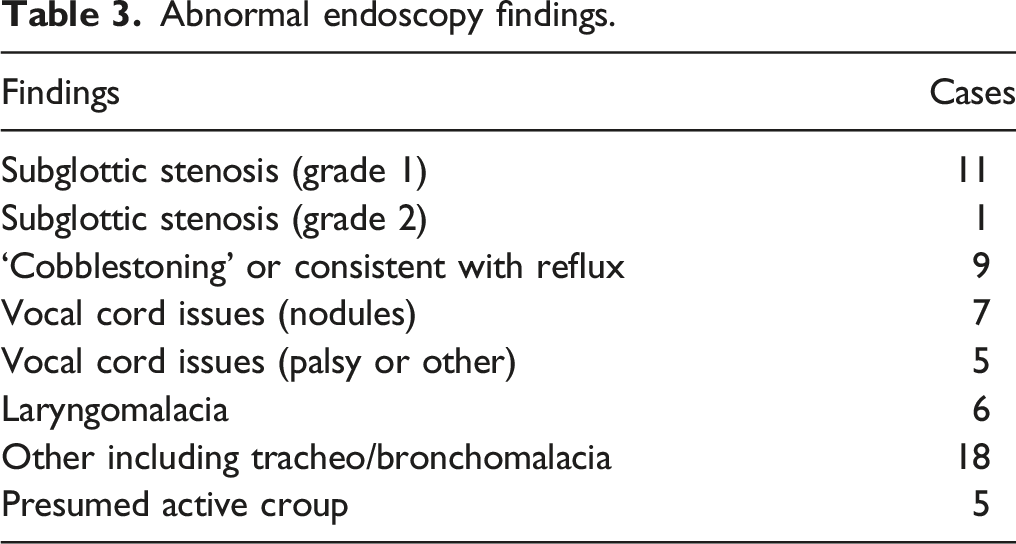
In ten years, 139 children underwent airway endoscopy for recurrent croup. Operative findings were abnormal in 62 (45 %) cases. Twelve cases (9%) had subglottic stenosis. Although recurrent croup was more common in males (78% of cases), this was not found to predispose them to operative findings. Children with previous intubations had >2 times the risk of abnormal findings and children born prematurely (<37 wks) had a trend towards abnormal operative findings versus children with no airway findings in our cohort. Even in those patients with abnormal findings, none necessitated further airway surgery.
Conclusions
Surgeons and parents can be reassured that rigid airway endoscopy for children with recurrent croup demonstrated high diagnostic utility but will rarely lead to further surgical intervention. Greater understanding about recurrent croup may require consensus clarification about definitions of recurrent croup and/or a universal adoption of a minimum standard operative record or grading system after rigid endoscopy for recurrent croup.
Key Points
Introduction
Croup is a clinical condition of characteristic barking cough and stridor found in patients with laryngotracheobronchitis. The barking cough usually develops on day 2 or 3 of acute viral infection of the larynx, trachea and bronchi. 1 Croup is one of the commonest presentations to paediatric emergency departments(ED) with reports of croup symptoms in up to 65% of all ED attendees. 2 Cross sectional studies suggest that croup may affect 15% children at least once in their lifetime, with a 5% population incidence. 3
Croup is the most common cause of upper airway obstruction in children aged 6 months to 6 years, but fortunately, most children can be successfully treated in the ED with steroid and adrenaline(nebulized racemic epinephrine), 4 leaving only between 1 and 6% requiring hospitalisation. 5
Croup can come to the attention of Ear, Nose and Throat (ENT) surgeons when it is recurrent or recalcitrant. Recurrent Croup is usually defined as ≥ two episodes per year of croup (either confirmed medically or reported by the parent).6,7 Recurrent croup should not be considered a diagnosis, but instead an indication to assess for non-viral pathology. 8
Thresholds in the literature for performing airway endoscopy in recurrent croup vary as do the reported findings. Operative findings vary from only 8.7% 9 to 60%, 10 73% 11 or as high as 100%, 12 which implies that either patient cohorts or indications for surgery are heterogenous, or that classification of findings may not be uniform. If surgeons use the Jabbour croup classification scheme 13 this can group normal and mildly abnormal findings together for analysis because they do not require further surgical management. 9
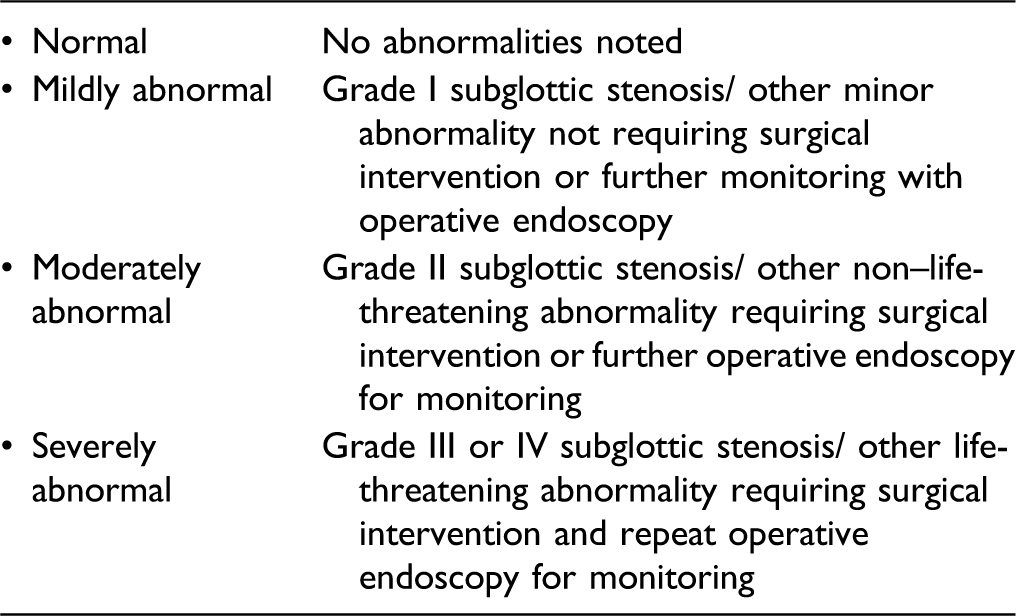
A 2016 systematic review suggested <9% pooled prevalence of ‘significant’ operative findings across 11 studies, using a variation on the Jabbour ‘moderately abnormal’ definitions. 14
At our centre, we anecdotally felt there were increasing numbers of negative findings on endoscopy so we sought to quantify our findings and look for correlations against pre-determined patient variables.
Materials and methods
This study and manuscript follow the STROBE reporting guidelines for observational cohort studies. 15
Ethical considerations and institutional review
This project was registered with the clinical audit and governance department at the Alder Hey Children’s NHS Foundation Trust. Retrospective data collection occurred for a 10 year period for all rigid endoscopies in which recurrent croup was coded.
Definitions
For the purposes of the initial analysis we defined recurrent croup as any written instance of ‘recurrent croup’, that is, surgeon reported recurrent croup, or documentation of 2 episodes or more.
We followed the WHO classification for prematurity based on gestational age: extremely preterm (<28 weeks), very preterm (28–32 weeks) and moderate to late preterm (32–37 weeks). 16
Search inclusion and exclusion criteria
We performed a retrospective review of the hospital electronic record system, using clinical coding to identify all children who had ever undergone rigid airway endoscopy who had received a diagnosis at some stage of recurrent croup. All ‘Microlaryngotracheobronchoscopy’ (airway endoscopy) performed at Alder Hey Children’s NHS Foundation trust with an indication of recurrent croup were included in further analysis.
Data were collected retrospectively for a decade spanning 1/1/10 until 31/12/19. We excluded any patients over 16 years old. We also excluded any patients who underwent airway endoscopy for a single episode of croup, even if it was severe. There is no management algorithm at our centre for this presentation and patients are taken to theatre based on multiple episodes of croup and ENT consultant decision regarding history and symptoms.
Statistical methods
Data were collated into Excel workbooks (Microsoft Office 365, Microsoft, USA). Statistical exploratory analysis was performed in SPSS (IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp). We analysed sample demographics and reported summary measures.
Variables of interest
Age at procedure, sex, referral source, gestational age at birth, number of previous intubations, documented comorbidities, number of croup episodes and anti-reflux treatment were all pre-determined variables that were analysed.
Results
There were 138 cases in our final ten-year cohort (see Figure 1). There were abnormal operative findings in 62 patients (45%). (Age and sex distribution of final cohort in Supplemental tables 1 and 2). Flow diagram for inclusion and exclusion of participants in final cohort.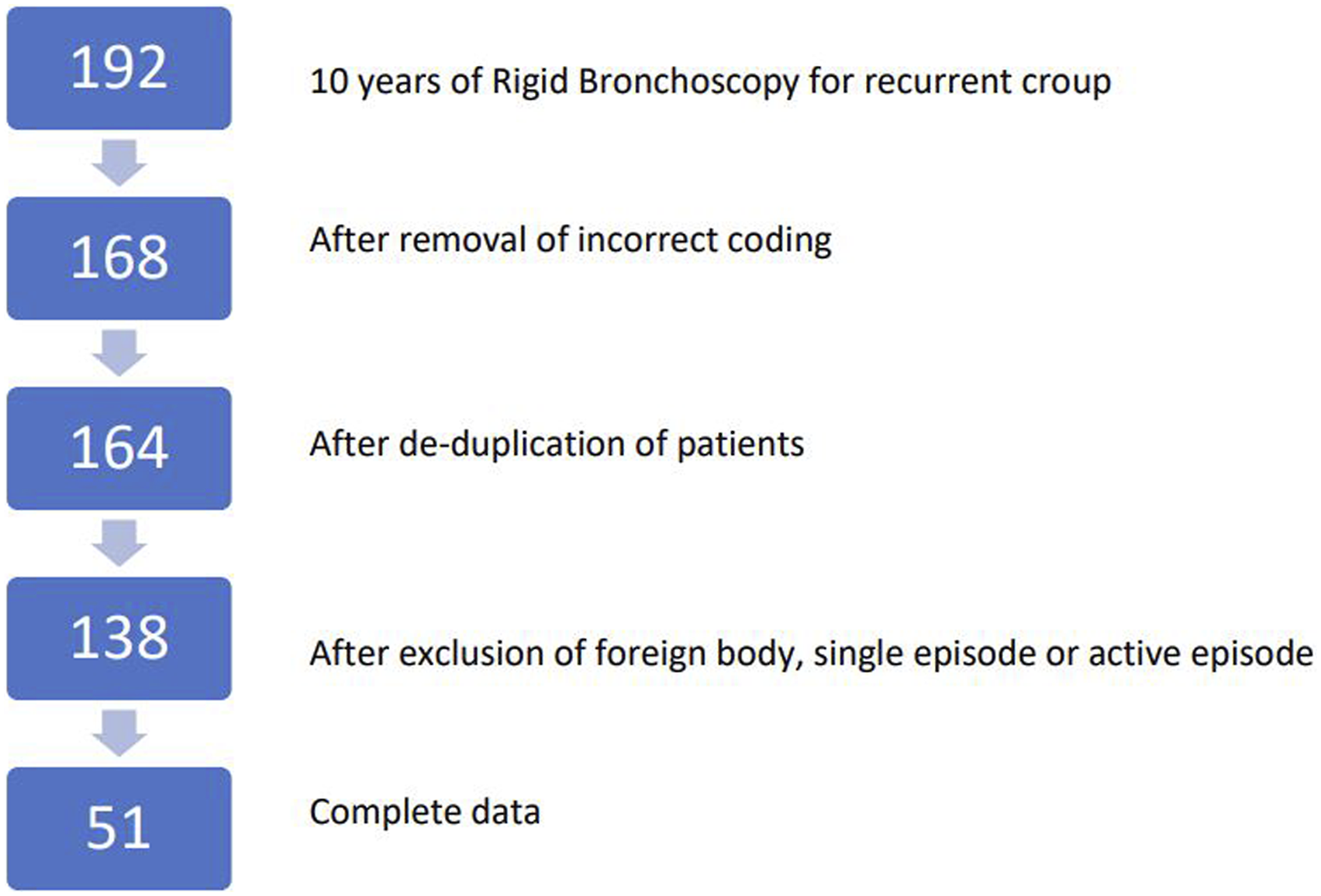
Referrals were received from Emergency, Paediatric, Respiratory, ENT and Intensive Care specialities as an inpatient and also from GP, Paediatric, Respiratory, Allergy and ENT as an outpatient.
The age distribution of cases is shown in Figure 2. Boys represented 78% of cases with recurrent croup (further details in supplement). There was no relation between sex and operative findings. (X2 = 1.9669, P = .160). Demographic breakdown.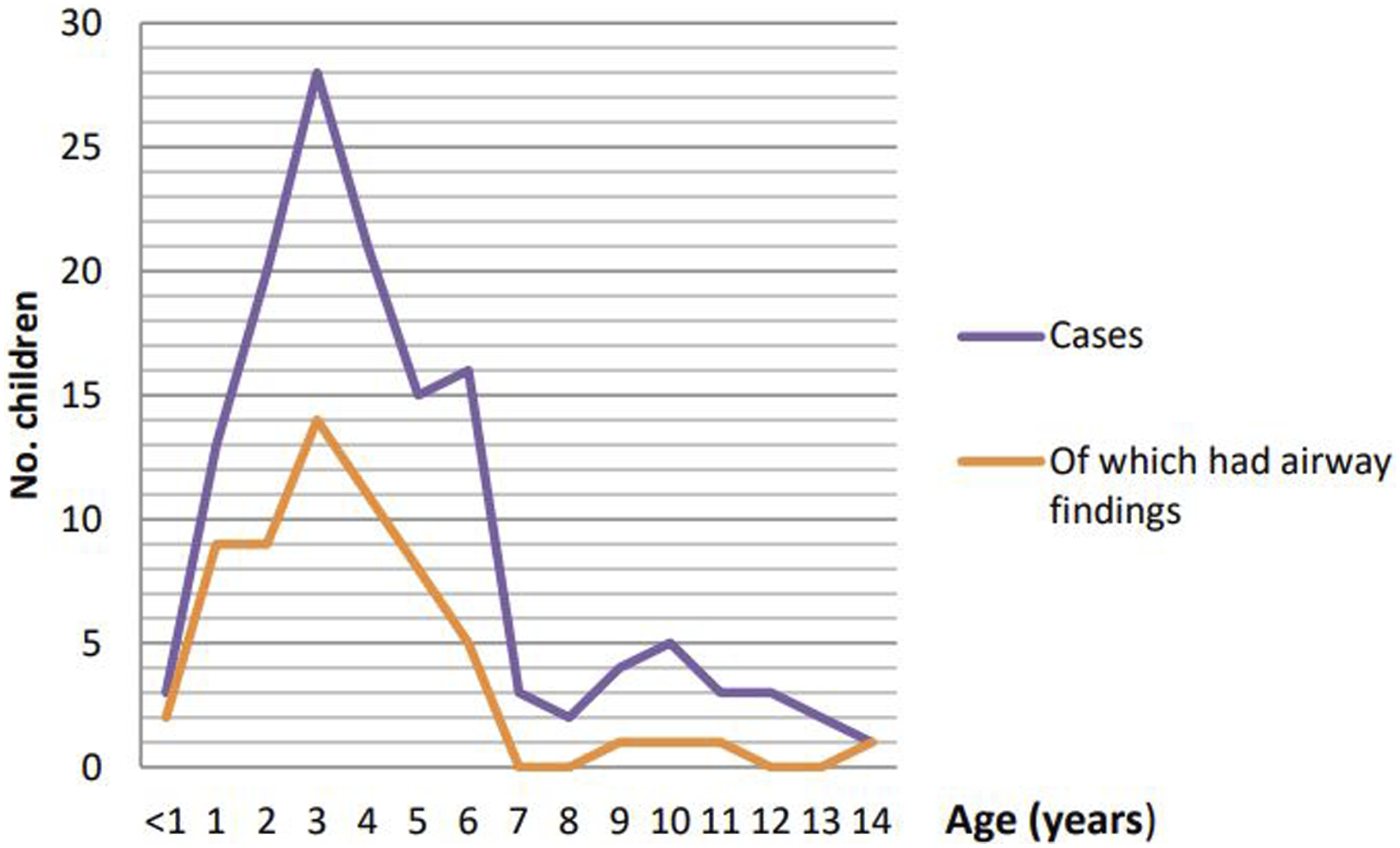
Gestational age of children with recurrent croup.
Previous intubations of children with recurrent croup (abnormal findings are available in Table 3).

Comorbidities
No comorbidities had a significant correlation with operative findings. Thirty-one patients had a physician diagnosis of ‘asthma’ of which 10 patients had operative findings. Sixteen patients had pre-operative treatment with anti-reflux medication and six of these had operative findings.
Endoscopy findings
Abnormal endoscopy findings.
Discussion
In our cohort the incidence of rigid endoscopy for recurrent croup was 138 patients over 10 years (just over one case per month). There were no significant findings needing further surgery due to airway pathology. More cases were seen in boys, but there was no significant increase in airway findings for these patients. The comorbidities, number of episodes of croup and pre-operative treatment did not appear to correlate with findings.
There was no study-size calculation performed and our study still looked at a relatively small number of patients (largest series in literature is 235). 10 We did not assess any other characteristics of the croup episodes, and these factors could be assessed in future studies, for example, time duration between episodes, increasing severity over time, persistent symptoms at rest (‘interval symptoms’), preceding viral illness, presence of tracheal tug or subcostal recession. We also choose not to examine data on parental-reported ethnicity or socioeconomic factors such as poverty, smoking exposure, number of siblings or environmental and indoor air pollution which all may be of relevance.
IgE RAST testing or other allergy testing was not performed as part of our centre’s primary work up, although this has occurred in previous studies assessing recurrent croup. 9 It has been reported that the value of non-specific paediatric IgE testing needs to be carefully interpreted and may not always yield helpful insights about aetiology. 17 We also did not assess vaccination status. Clarity about both of these measures will likely form part of any future protocol and study. Although our data did not allow correlations between patients with asthma, reflux and croup, in the future it may prove useful to consider these patients as a discrete cohort.
We found considerable missing data which precluded some statistical analyses. This data was not missing-at-random and we have attributed missing data variously to inconsistency in operative record by surgeons, and heterogeneity in information that was reported in ED clerkings, pre-op assessment, anaesthetic charts and clinic letters. This will introduce bias to conclusions. Our decision to focus on complete case analysis rather than model with maximum likelihood estimation was made because of the heterogenous cohort we were studying with multiple additional changes in perioperative care and medical management which occurred in the study period.
We found similar numbers of operative findings compared with other UK and USA cohorts. Discrepancies may relate to surgeon preference based on the history or alternative use of diagnostic scores. Issues about definitions, particularly of ‘recurrent croup’ itself are often heterogenous. It remains to be seen whether these findings will differ from the experience of colleagues outside Europe and North America.
It is worth noting that of our patients with ‘normal findings’ (n = 77), only one patient who was followed up had further episodes of croup. Of the 46 children who were not followed up (60% of the patients with ‘normal findings’) there were no further reported croup episodes at our centre. A Scottish cohort, found 50% of their ‘normal findings’ group had persistent symptoms at follow up. 10 We are not certain if primary care or other centres started medications or initiated other treatment and this level of follow up information would also be useful in future studies.
The aetiology of the recurrent croup syndrome is likely to be varied and others have investigated numerous non-viral causes including; asthma, allergy, reflux and eosinophilic oesophagitis in addition to intrinsic or extrinsic narrowing of the subglottis and trachea. 13 Hoa et al found reflux–related changes in 87% of their recurrent croup cases and reflux treatment improved symptoms in 87% who were surveyed. 18
The International Pediatric Otolaryngology Group (IPOG) issue consensus management recommendations for numerous conditions with equipoise or uncertainty in their management. 19 Paediatric emergency departments and respiratory physicians also have expertise with recurrent croup patients and multi-disciplinary management may provide benefit for all teams. Initiatives based on these collaborations include multi-centre prospective observational cohort studies like BronchStart. 20 To our knowledge there are no such recommendations or initiatives for recurrent croup and we would welcome the development of expertise-based consensus recommendations regarding risk factor models or the management of recurrent croup, with the goal of improving patient care.
Conclusion
Clinicians and parents can be reassured that rigid airway endoscopy for children with recurrent croup seems to demonstrate high diagnostic utility in this cohort but rarely lead to further surgical intervention. We recommend clarification about definitions of recurrent croup and a universal adoption of a single grading system for operative findings after rigid endoscopy for recurrent croup. Whether that be the Jabbour croup classification or a modification (that pools all outcomes which require no further intervention) should be agreed by paediatric otolaryngologists before adoption. In the mean-time, we recommend the adoption of a minimum standard operative record for all such procedures which documents at least; sex, age at time of procedure, gestational age at birth, number of previous intubations, documented comorbidities, number of previous recurrent croup episodes and whether there were any medication or treatment trials pre-operatively for the same condition (e.g. diet change, anti-reflux treatment or asthma inhaler). We hope that with a shared set of objectives we can pool our insights with other centres and understand more about children with recurrent croup, particularly if this could enable us to safely discern how to reduce the number of children taken to theatre with recurrent croup in the future.
Supplemental Material
Supplemental Material - Recurrent croup is a good indicator of underlying paediatric airway issues: A 10-year retrospective cohort study of airway endoscopy
Supplemental Material for Recurrent croup is a good indicator of underlying paediatric airway issues: A 10-year retrospective cohort study of airway endoscopy by Thomas Hampton, MRes, Randa Ghazal Asswad, MBChB, Jaya Bhat, MBBS, Kate Stevens, MBChB, Emma Whitehall, MBChB, Kristijonas Milinis, MPhil, Su De, FRCS(ORL-HNS), Adam Donne, PhD and Madhan Krishnan, FRCS(ORL-HNS) in Progress in Ear, Nose and Throat Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TH receives grant funding from The Wellcome Trust (203919/Z/16/Z) but none of the authors report any other conflicts of interest financial or otherwise.
Data availability
Fully anonymised data that contributed to this manuscript are available on reasonable request only.
ICJME statement
MK conceived the project; MK, AD, SD and TH designed the work; TH, RGA, JB, KS, EW and KM acquired and analysed data; TH drafted and revised the manuscript; RGA, KM, SD, AD and MK provided further revisions to the manuscript; all authors approved the final manuscript; TH agrees to be accountable for all aspects of the work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.