
Abstract
In recent years, it has become increasingly apparent that the laryngotracheal stenosis (LTS) cohort comprises distinct etiological subgroups; however, treatment of the disease remains heterogeneous with limited research to date assessing predictors of treatment outcome. We aim to assess clinical and surgical predictors of endoscopic treatment outcome for LTS, as well as to further characterize the disease population. A retrospective chart review of adult patients with LTS presenting over a 16-year period was conducted. Seventy-five patients were identified and subdivided into 4 etiologic subgroups: iatrogenic, idiopathic, autoimmune, and “other” groups. Statistical comparison of iatrogenic and idiopathic groups was performed. Subsequently, stepwise logistic regression was employed to examine the association between clinical/surgical factors and treatment outcome, as measured by tracheostomy incidence and dependence. We demonstrate that patients with iatrogenic LTS were significantly more morbid (P < .001) and had worse disease, with significantly greater percentage stenosis (P = .015) and increased incidence of tracheostomy (P < .001). Analyzing the predictive effect of clinical and surgical variables on endoscopic treatment outcome, we have shown that when adjusted for age, sex, and iatrogenic etiology, patients with an American Society of Anesthesiologist score >2 were significantly more likely to undergo tracheostomy (adjusted odds ratio = 11.23, 95% confidence interval [CI] = 1.47-86.17). Similarly, when compared with their idiopathic counterparts, patients with iatrogenic LTS had higher odds of undergoing tracheostomy (17.33, 95% CI = 1.93-155.66) as were patients with Cotton-Myer grade 3-4 stenosis (9.84, 95% CI = 1.36-71.32). The odds of tracheostomy dependence at time of last follow-up were significantly higher in patients with gastroesophageal reflux disease (15.38, 95% CI = 1.36-174.43) and cerebrovascular accident (9.03, 95% CI = 1.01-81.08), even after adjustment. No surgical techniques were significantly associated with either outcome when adjusted. We present a heterogeneous LTS cohort comprised of homogeneous subgroups with distinct levels of morbidity, disease morphology, and treatment burden. Further our data suggest that the treatment outcome is more dependent on patient factors, rather than surgical technique used.
Introduction
Laryngotracheal stenosis (LTS) occurs as a result of a pathological fibroinflammatory repair process producing recurrent and excessive scarring in the larynx and trachea. Progressive luminal narrowing subsequently can lead to life-threatening airway obstruction. 1,2
Etiology
The literature describes various causes of LTS, with the most common being idiopathic, autoimmune, and iatrogenic (postintubation) etiologies. 3 Making an etiological distinction is of vital importance; while somewhat homogeneous in presentation, large retrospective chart reviews have revealed that etiology significantly alters the morphology, disease course, pathophysiology, treatment response, and outcomes. 2
The literature shows that the most common cause of LTS is iatrogenic, occurring postintubation, in particular following the use of large endotracheal tubes (ETTs) and prolonged ETT placement. 4,5 Large case series have shown that this cohort have higher rates of tobacco use, cardiovascular disease, obesity, and diabetes, which are thought to result in vulnerability to ischemic damage and states of dysregulated wound healing. 3,4,6,7 Patients have stenotic segments that are longer and further from the glottis than other etiologies and tend to have worse outcomes, with increased tracheotomy dependence and higher rates of intervention. 4,8
Laryngotracheal stenosis may also develop in many autoimmune and rheumatological diseases. Most established is its association with granulomatosis with polyangiitis (GPA). Laryngotracheal stenosis has been noted to develop in 12% to 23% of patients with GPA. 9,10 Patients with GPA LTS are more likely to undergo tracheotomy and are also more likely to require additional treatment following open surgery than their idiopathic counterparts, due to the ongoing disease process. 4,11
Idiopathic subglottic stenosis (iSGS) is a rare disease with an incidence of roughly 2.5 per million person-years. 2,12 It is a diagnosis of exclusion and is yet to be defined. 2,13 Multiple series have shown that the disease affects primarily otherwise well Caucasian (95%), perimenopausal (average age: 47-50.4) females (98%-99.2%). 2,4,12 Idiopathic subglottic stenosis is classically localized to the subglottis and as such has been labeled subglottic stenosis rather than LTS in this article. However, it may, less commonly, occur in other laryngeal and tracheal subsites. Idiopathic subglottic stenosis has the lowest rates of tracheotomy dependence and requires less frequent treatment. 2,4,8
Management
The primary aim of subglottic stenosis management is to maintain airway patency and reduce dyspnea. Additional goals include preservation of voice and swallow. However, the avoidance of a tracheotomy and decannulation of tracheotomy are more objective end points and are therefore used in the literature to evaluate treatment success. Time to second procedure is often a secondary measure of treatment success, because of the chronic nature of the disease and rates of recidivism. 4,7,8 Nonetheless, the comparison of surgical outcomes can be difficult, due to inconsistent outcome measures across studies, as well as the waxing and waning nature of the disease.
Endoscopic management typically consists of incision or excision of scar tissue with carbon dioxide laser or cold steel, dilatation of stenosis with bougie or balloon, plus or minus intralesional or topical adjuvant therapy at the time of dilatation such as steroid injection or mitomycin C application. 4,14 Serial dilatations have been shown to achieve improved airway diameter and successful decannulation in patients previously requiring tracheotomy. Generally, patients require 1 to 2 procedures per year to retain airway patency, but at times this can even achieve cure. 1,9,15,16
Open surgery, on the other hand, consists of either resection and anastomosis or reconstruction with or without grafting, depending on the extent and level of stenosis. Open procedures have achieved high rates of decannulation in select groups. Although potentially more successful, patients may experience restenosis following major surgery, requiring further treatment, and are subject to a high degree of morbidity from potential complications and long-term alterations in voice 17 -19 and swallow. 20
Although tracheotomy is a lifesaving procedure that maintains airway patency, it affects voice, swallowing, breathing, and quality of life. Additionally, instrumentation of an airway predisposed to scar formation can worsen the overall disease state by extending the degree of stenosis, dynamic collapse, and increasing risk of bacterial colonization. 3,21,22
The rarity of LTS, combined with the heterogeneous cohort, geographic separation, and inconsistencies in treatment, makes comparative effectiveness research difficult. In the absence of prospective observational studies, retrospective reviews form an important tool in understanding etiological subgroups and varying response to treatment.
We have, for the first time, described an Australian cohort of LTS patients receiving care at a single, tertiary-referral center over a 16-year period, and have investigated patient and treatment factors as predictors of treatment outcome.
Materials and Methods
A retrospective chart review was performed to analyze the LTS cohort at our center over a 16-year period from January 1, 2001, to January 1, 2017, to identify LTS patients who had undergone endoscopic management. Laryngotracheal stenosis patients were identified via Health Information Services using the 10th version of the “International Statistical Classification of Diseases and Related Health Problems” diagnostic codes relating to LTS.
The following criteria were used to determine the stenosis etiology at our institution. Disease was coded as iatrogenic if the patient had undergone a major surgery in the 2 years leading up to presentation, 3 and as autoimmune LTS if they had a coexisting diagnosis of connective tissue disease. If neither of these diagnoses were applicable, patients were labeled with iSGS. Patients with other given diagnoses, that is, postinfective and polytraumatic were included in the “other” category.
When surgical details were unavailable, data were recorded as missing. Although many patients underwent multiple procedures, only treatment information from their first procedure was used. All patients underwent endoscopic treatment.
Two treatment outcomes were identified, tracheotomy dependence (tracheotomy at time of last follow-up) and tracheotomy incidence (undergoing tracheotomy at any time during treatment). Mean procedure interval was also identified as a possibly secondary outcome but was not analyzed due to numerous covariables and missing data.
All data were processed using Statistical Package for the Social Sciences (SPSS), version 24.0 (IBM, New York, New York). Missing data were left blank and no substitution via imputation or any other means was performed. Variables with greater than 10% randomly missing data were not included in statistical analysis. An α of .05 was considered to be statistically significant.
Descriptive analysis was performed on the total population and on etiological subgroups. Categorical variables were reported using relative frequencies. As the data were not normally distributed, nonparametric statistics were used, and continuous numerical variables were reported as medians with interquartile ranges (IQRs) to account for outliers. Iatrogenic and idiopathic subgroups were compared in isolation, as autoimmune and “other” groups lacked sufficient sample size. Chi-squares were used for categorical variables, with additional continuity correction for 2-by-2 comparisons. Fisher exact tests were used when expected counts below 5 exceeded 20% of all expected counts.
Surgical and clinical predictors of outcome were analyzed using stepwise logistic regression analysis. Predictor variables were carefully selected in advance by clinical significance so as to avoid “data dredging.” Predictor variables were initially tested with bivariate analysis as above, and an unadjusted odds ratio (OR) was found. Variables were then adjusted for age, sex, and iatrogenic etiology to yield an adjusted OR (AOR). This project has been carried out in accordance with the Declaration of Helsinki and was approved by the Monash Health and Monash University Human Research Ethics Committees (LNR/17/MonH102).
Results
Etiological Differences
We identified 75 patients with LTS, treated at our center over the 16-year period. The most common etiology was idiopathic (49.3%) followed by iatrogenic (35.7%), autoimmune (9.3%), and other (6.7%).
Demographics and comorbidities
Demographic characteristics and comorbidities have been described in Table 1. Iatrogenic patients tended to be older than their counterparts, with a median age of 62.5 (IQR: 48.8-72.3). Unlike other etiological groups, idiopathic patients were almost entirely female (97.3%). The cohort had a median body mass index of 28 (IQR: 24.6-33.1) indicating that patients tended to be overweight. The American Society of Anesthesiologists (ASA) score given to each patient perioperatively was recorded and assessed. There were greater proportions of ASA scores above 2 in iatrogenic (53.8%) and autoimmune (42.9%) groups, when compared with the idiopathic group (5.6%). This was consistent with higher rates of diabetes (30.8%), hypertension (46.2%), stroke (19.2%), and acute myocardial infarction (15.4%) in the iatrogenic group than in other subgroups. Conversely, idiopathic patients had higher rates of clinically reported gastroesophageal reflux disease (GERD; 73%).
Demographics, Comorbidities, Disease Morphology, and Treatment Grouped by Etiology.a
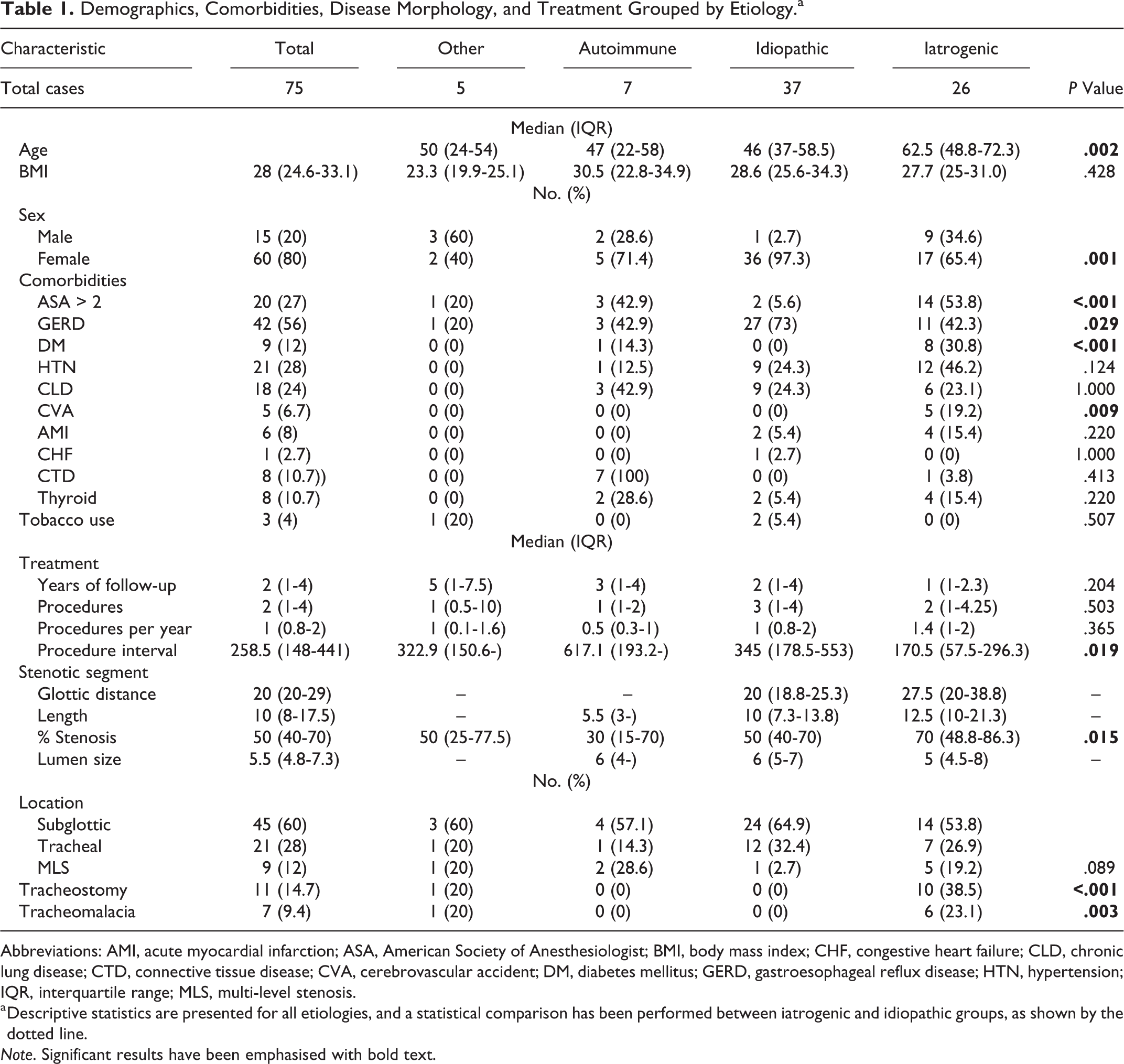
Abbreviations: AMI, acute myocardial infarction; ASA, American Society of Anesthesiologist; BMI, body mass index; CHF, congestive heart failure; CLD, chronic lung disease; CTD, connective tissue disease; CVA, cerebrovascular accident; DM, diabetes mellitus; GERD, gastroesophageal reflux disease; HTN, hypertension; IQR, interquartile range; MLS, multi-level stenosis.
a Descriptive statistics are presented for all etiologies, and a statistical comparison has been performed between iatrogenic and idiopathic groups, as shown by the dotted line.
Note. Significant results have been emphasised with bold text.
Disease morphology
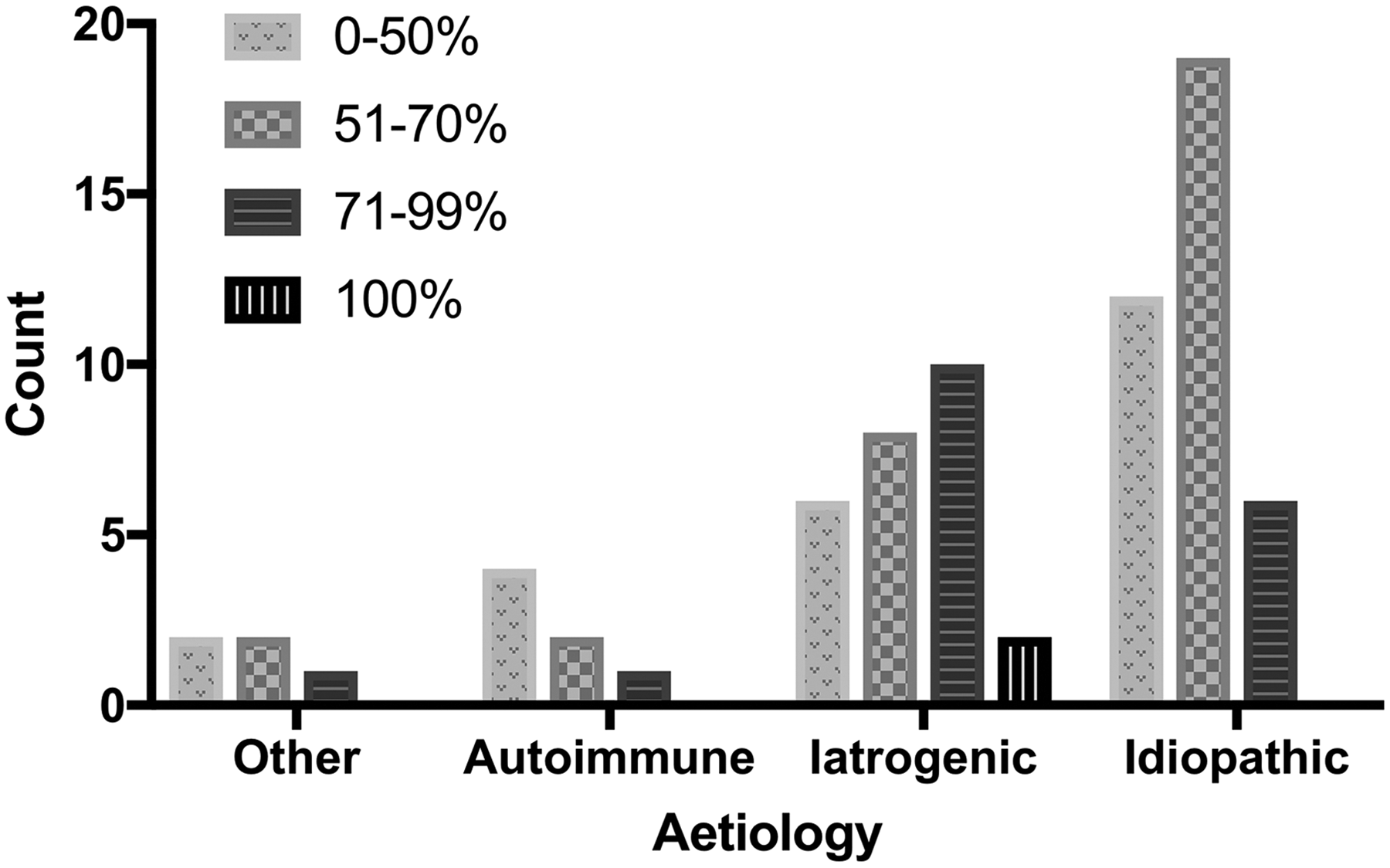
Overall, patients presented with a median of 50% stenosis (IQR: 40-70), but iatrogenic patients presented with a greater degree of stenosis than other subgroups, median 70% (IQR: 48.8-86.3). Figure 1 illustrates proportions of Cotton-Myer (CM) score across etiological groups. In comparison to the total cohort, iatrogenic LTS segments were longer (median: 12.5, IQR: 10-21.3) and further from the glottis (median: 27.5, IQR: 20-38.8). Meanwhile, patients with iSGS had shorter (median: 10, IQR: 7.3-13.8) stenotic segments that were closer to the glottis (median: 20, IQR: 18.8-25.3).
Stenosis location stratified by Cotton-Myer score.
Of all stenoses, 60% of segments were confined to the subglottis, 28% to the trachea and 12% spanned multiple subsites. In comparison, iatrogenic patients were more likely to have multilevel stenosis (19.2%), both with and without glottic involvement (Table 1; Figure 2), whereas only 1 (2.7%) patient with iSGS had multilevel stenosis.
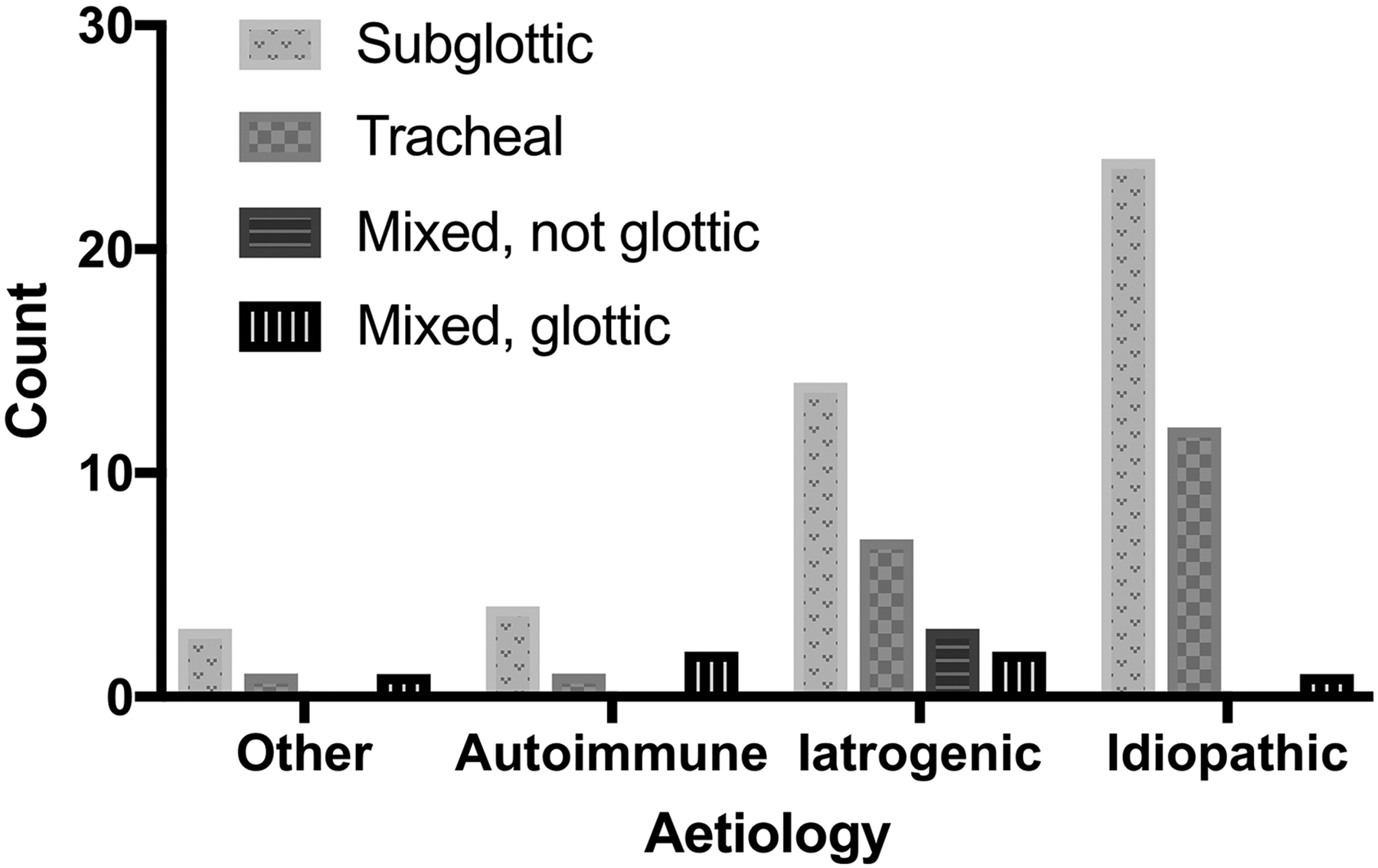
Stenosis location stratified by etiology.
Treatment
Patients experienced similar length and frequency of treatment across subgroups. Patients with LTS classified as “other” seemingly were followed up for longer periods of time (median: 5, IQR: 1.75). Meanwhile, iatrogenic patients underwent procedures most frequently, with the highest number of procedures per year (median: 1.4, IQR: 1-2) and the shortest number of days between procedures (median: 170.5, IQR: 57.5-296.3). Conversely, individuals with autoimmune LTS had the longest interval between procedures, with a median of 617.1 days (IQR: 193.2-undefined).
Comparison of iatrogenic and idiopathic groups
Comparison between all etiological subgroups was not possible due to limited sample sizes. However, the data set was analyzed for differences between idiopathic and iatrogenic groups.
Iatrogenic patients (median: 62.5, IQR: 48.8-72.3) were significantly older than their idiopathic (median: 46, IQR: 37-58.5) counterparts (P = .002). They also had significantly higher rates of diabetes (30.8% vs 0%, P < .001) and stroke (19.2% vs 0%, P = .009). This is in keeping with a significantly higher number of iatrogenic patients with an ASA score above 2 (53.8% vs 5.6%, P < .001). Conversely, while the majority of idiopathic patients (73%) had GERD, a significantly smaller number of iatrogenic patients (42.3%) were diagnosed with the disease (P = .029). Comparison of percentage stenosis indicated that iatrogenic patients presented with significantly more severe stenosis of 70% (IQR: 48.8-86.3) compared with 50% (IQR: 40-70) in idiopathic patients (P = .015; Figure 1).
Iatrogenic patients experienced higher rates of tracheotomy (38.5%) and tracheomalacia (23.1%), when compared with the idiopathic group (0%, P < .001 and P = .003). There was no statistically significant difference in years of follow-up or number of procedures among iatrogenic and idiopathic patients. The same was true for procedures per year. Iatrogenic patients experience a significantly shorter interval between procedures, with a median of 170.5 days (IQR: 57.5-296.3), compared with 345 days (IQR: 178.5-553, P = .019).
Treatment Outcomes
Stepwise multivariate logistic regression was performed on patient and endoscopic surgical factors to evaluate whether they were predictive of tracheotomy incidence as well as tracheotomy dependence at time of last follow-up. “Age” was converted into a categorical variable, splitting the cohort at the 50th centile. Similarly, “procedures per year” was split into the third of patients receiving the most treatments per year and the two-thirds of patients receiving the least.
Clinical factors
Table 2 summarizes the association between clinical variables and tracheotomy incidence/dependence. The adjusted odds of undergoing tracheotomy in patients with ASA scores above 2 were 11.23 (AOR = 11.23, 95% confidence interval [CI] = 1.47-86.17) times those of a patient with an ASA below 2. Patients with stroke were more likely to be tracheotomy-dependent at time of last follow-up when adjusted for sex and etiology (AOR = 9.03, 95% CI = 1.01-81.08), though this was on the cusp of insignificance. With adjustment, patients diagnosed with reflux had 15.39 (95% CI = 1.36-174.43) times higher odds of requiring tracheotomy at last follow-up than those without.
Clinical Factors as Predictors of Treatment Outcome.a
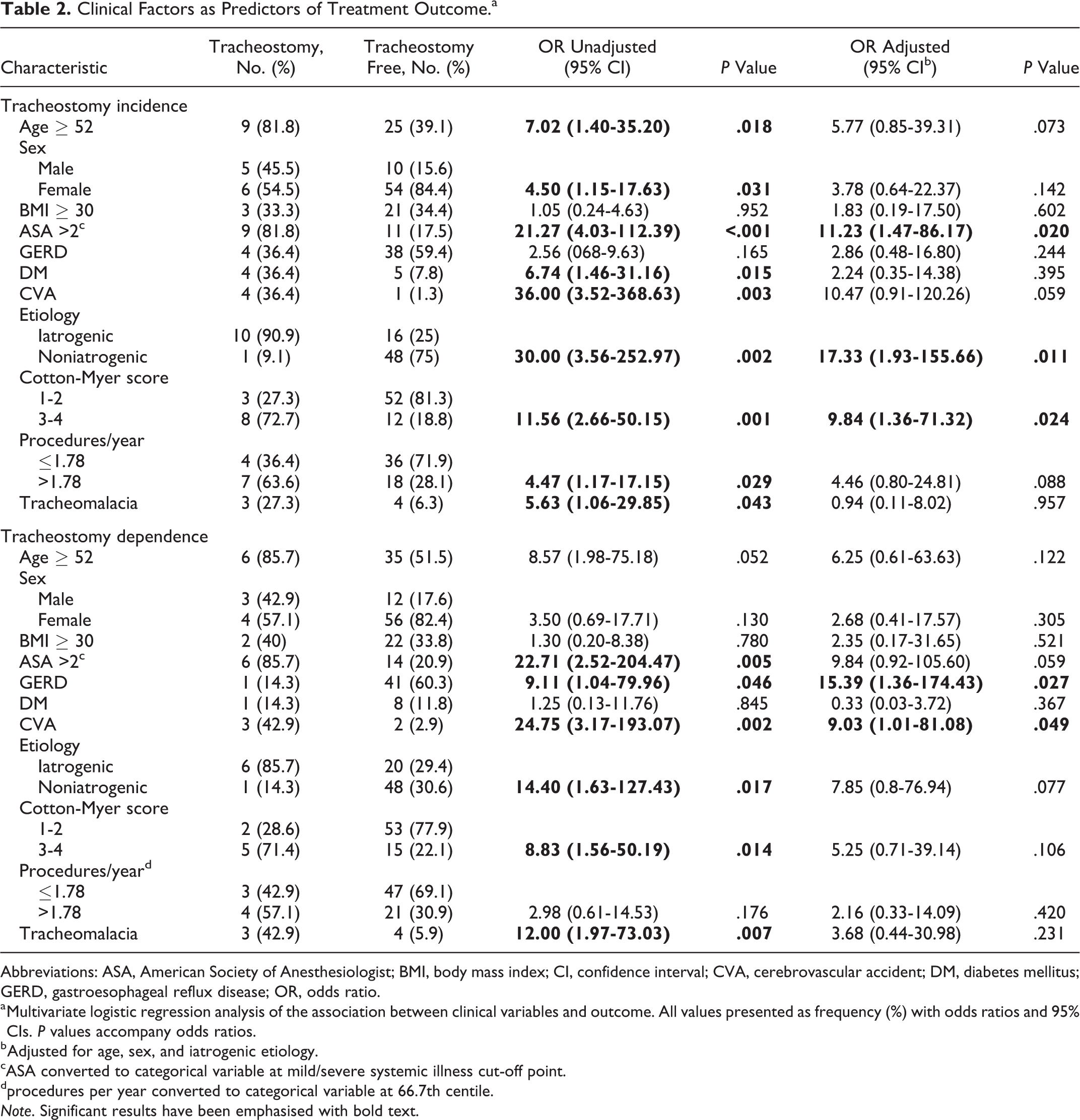
Abbreviations: ASA, American Society of Anesthesiologist; BMI, body mass index; CI, confidence interval; CVA, cerebrovascular accident; DM, diabetes mellitus; GERD, gastroesophageal reflux disease; OR, odds ratio.
a Multivariate logistic regression analysis of the association between clinical variables and outcome. All values presented as frequency (%) with odds ratios and 95% CIs. P values accompany odds ratios.
b Adjusted for age, sex, and iatrogenic etiology.
cASA converted to categorical variable at mild/severe systemic illness cut-off point.
dprocedures per year converted to categorical variable at 66.7th centile.
Note. Significant results have been emphasised with bold text.
Patients with iatrogenic etiology (AOR = 17.33, 95% CI = 1.93-155.66) and those with a CM score of grades 3 and above (AOR = 9.84, 95% CI = 1.36-71.32) were more likely to require tracheotomy during treatment, but this did not hold true for tracheotomy dependence. Tracheomalacia was not associated with a statistically significant increase in the odds of tracheotomy incidence (AOR = 0.94, 95% CI = 0.11-8.02) or dependence (AOR = 3.68, 95% CI = 0.44-30.98), when adjusted for age, sex, and iatrogenic etiology.
Surgical factors
Endoscopic surgical variables were similarly compared with treatment outcome in a stepwise logistic regression model, summarized in Table 3. Before adjustment, patients in whom no cutting modality was used were more likely to be tracheotomy free than those patients in whom cold steel or laser was used (OR = 11.53, 95% CI = 1.30-102.02). Conversely, the odds of undergoing tracheotomy in patients who did not undergo dilatation were 4.44 (1.07-18.39) times higher than those who were dilated. Neither of these results retained significance when adjusted for age, sex, and iatrogenic etiology. Even prior to adjustment, no surgical factors achieved significance when evaluated as predictors for tracheotomy dependence. Neither intralesional nor postoperative steroid was significantly associated with tracheotomy incidence or dependence.
Surgical Factors as Predictors of Treatment Outcome.a
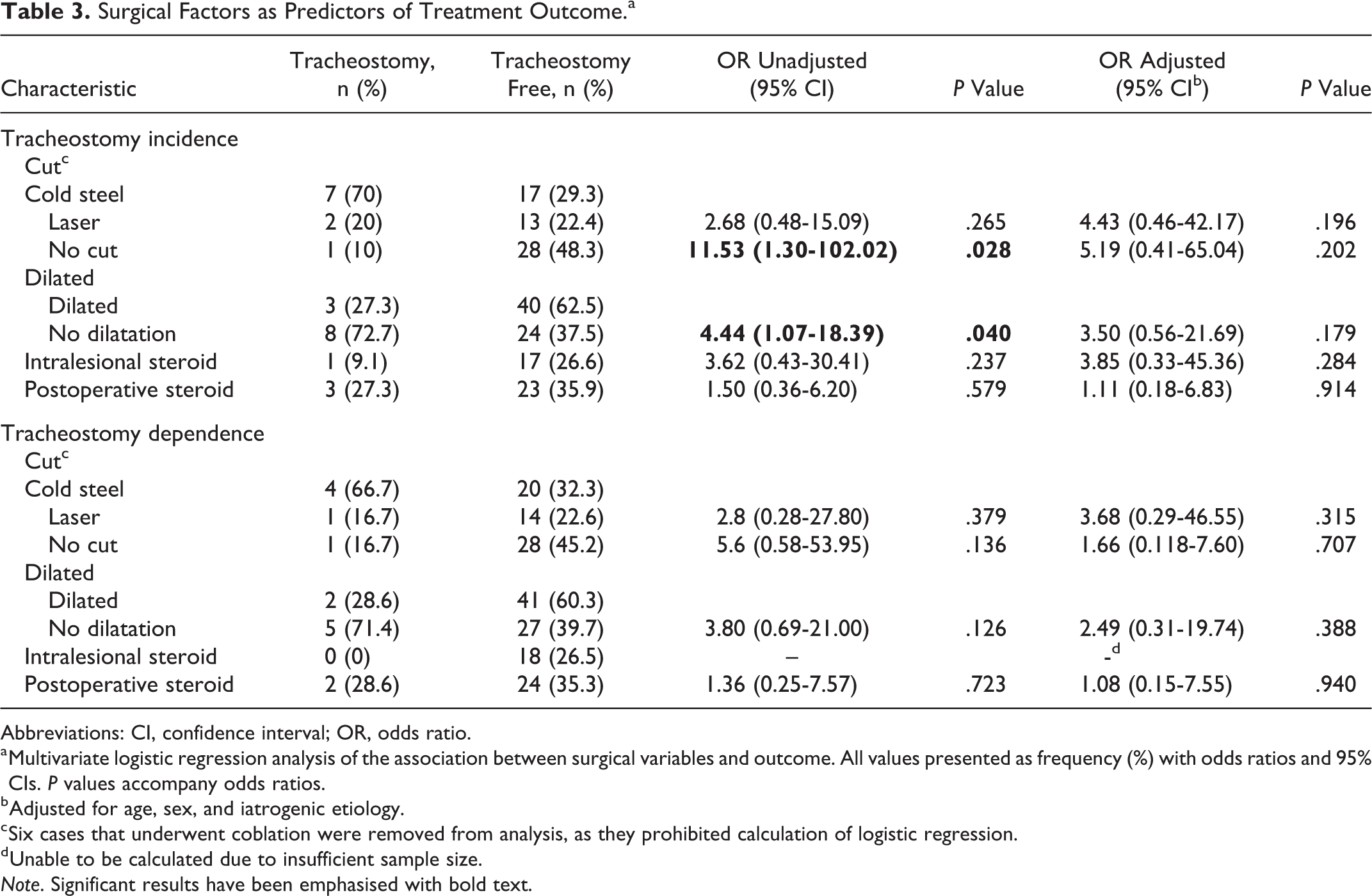
Abbreviations: CI, confidence interval; OR, odds ratio.
a Multivariate logistic regression analysis of the association between surgical variables and outcome. All values presented as frequency (%) with odds ratios and 95% CIs. P values accompany odds ratios.
b Adjusted for age, sex, and iatrogenic etiology.
c Six cases that underwent coblation were removed from analysis, as they prohibited calculation of logistic regression.
d Unable to be calculated due to insufficient sample size.
Note. Significant results have been emphasised with bold text.
Discussion
Group Comparison
Initially, the LTS cohort appeared to be an ill-defined heterogeneous group of patients, but patterns emerged when broken down into their respective etiological subgroups. In our study, of the 75 patients identified with LTS over a 16-year period, almost half had iSGS, and a further 35% had iatrogenic stenosis. The relative proportions differed from other series of LTS populations, which found iatrogenic stenosis to be the most common etiology, comprising approximately 50% of the cohort. 3,4 This difference in representation may be attributed to the protocol used to identify patient etiology when none was explicitly stated. However, a similar protocol was utilized by Gelbard et al who found that 55% of their cohort were iatrogenic cases. It is possible that the lower density of iatrogenic patients may reflect the nature of our patient population or represent the strong emphasis on ward-based and outpatient tracheotomy care at our institution, with early decannulation and extubation protocols instituted to minimize laryngotracheal scarring. Additionally, the iSGS cohort have a strong online presence with multiple peer support groups. Given a strong laryngology focus at our institution, word-of-mouth referrals may have contributed to the higher proportion of idiopathic cases in our cohort. Further, trauma cases requiring prolonged intubation in intensive care are often referred to other trauma-focused hospitals, and as such our department may see fewer iatrogenic and traumatic LTS cases.
As hypothesized, subgroups tended to be quite homogenous, indicating that although they present similarly, they are in fact driven by distinct disease processes.
As reported in other series, 4,12,14 the iSGS group was primarily female, in their fifth and sixth decade and overweight. Additionally, they also had the highest proportion of recorded GERD, supporting the hypothesis that reflux may contribute to the pathogenesis, or at least the potentiation of the disease. 23,24 It is also plausible that a reported diagnosis of GERD in patients with iSGS was overrepresented, as clinicians, knowing the association between iSGS and reflux, 2 may have had a lower threshold for diagnosing the presence of reflux on clinical grounds in these patients, than in patients with other subtypes of LTS.
Meanwhile, iatrogenic patients tended to be sicker than other etiological groups with higher rates of stroke and diabetes suggesting that their susceptibility to scar formation following intubation may be mediated by underlying vascular disease and resultant ischemia. 4,7 Factors predisposing to poor mucosal wound healing may further exacerbate disease, accounting for the significantly longer and narrower stenotic segments. Significantly, higher rates of tracheotomy and tracheomalacia are likely the result of aggressive disease and more morbid patients who are unfit for frequent procedures.
Interestingly, autoimmune patients had the longest mean procedure interval and lowest number of procedures per year. Although one must be cautious in interpreting results from a sample size of 8, these findings are corroborated by larger series and may be the result of good pharmacologic disease control and/or the relapsing-remitting nature of autoimmune disease with periods of active inflammation and relative dormancy. 2,11,25
Predictors of Treatment Outcome
Iatrogenic etiology was strongly predictive of tracheotomy incidence, conferring a 17.33 (95% CI = 1.93-155.66) times increase in adjusted odds compared to other etiologies. This likely accounts for the initial association between older age, male sex, stroke, and diabetes (Table 2), as well as the reduction in significance following adjustment. Patients with an ASA above 2 were more likely (AOR = 11.23, 95% CI = 1.47-86.17) to undergo tracheotomy, which is likely associated with increased LTS severity. Additionally, increased morbidity may have precluded them from undergoing frequent surgery, thus necessitating a surgical airway.
Prior to adjustment, patients who underwent procedures involving endoscopic cold steel resection of their stenosis were significantly more likely to undergo tracheotomy during treatment. Conversely, patients undergoing dilatation were more likely to be tracheotomy free, which is perhaps unsurprising, given the influence of disease severity on choice of treatment. However, these associations were no longer significant when adjusted. As hypothesized, there were no significant associations between surgical technique and tracheotomy dependence at last follow-up. These findings support similar conclusions made by Gadkaree et al and Hseu et al. 4,14 While, Gadkaree et al did find that intraoperative steroid injection was predictive of tracheotomy-free survival, our data did not support this. As such, we have demonstrated that the treatment outcome is more strongly related to patient factors, and in particular etiology and morbidity, than it is to endoscopic technique or surgical factors. Although comparing the outcomes of patients treated with these 2 different treatment modalities was not within the scope of this retrospective review, we plan to collect prospective data to compare these 2 groups in the future.
Evaluation of Methodology
As a result of the retrospective nature of this study, there are certain inherent weaknesses in its methodology. In particular, the assessment of treatment outcome in the LTS cohort is hindered by temporal difficulties inherent in retrospective reviews such as changes across time in data collection methods, which can lead to discrepant or missing data, as well as potential changes in surgeons who may vary in treatment preference and differences in treatment trends over time. Additionally, although we adjusted for some potential confounders, other potential confounding variables remain. Mitigating for the heterogeneity in disease course between individual patients was a particular challenge. Some patients underwent 1 procedure, or in excess of 10 procedures over the course of follow-up. Including all instances of surgery for each patient would result in variable representation, and therefore, weighting of each patient which would not be statistically robust. We therefore sourced data on stenotic segment and surgical approach at time of first presentation. As such, other techniques used during the follow-up period were not assessed. Indeed, analyzing the effect of surgical technique on outcome is difficult without the use of a prospective randomized control trial, which is very difficult to perform on a patient cohort with a rare disease. Inconsistencies are further compounded when considering that LTS patients may move between hospital systems over the course of their treatment. A retrospective design of the study necessitated the end of follow-up to be taken as a surrogate end point so outcomes are not necessarily fully realized.
Further, while tracheotomy is a useful and definitive treatment outcome, more subtle differences in outcome conferred by surgical technique were not measured but might be detected by nondichotomous variables such as time to second procedure, mean procedure interval, or procedures per year—though these variables are often plagued by nonrandom missing data. Peak flow spirometry may also provide a less crude and more objective measure of treatment effect.
Additionally, despite this study including a relatively large cohort of patients for the disease type, sample size issues arose during the statistical analysis of our data. This was particularly evident when calculating 95% CIs for ORs, which yielded large ranges, and in some instances, undefined results. Additionally, the small sample size of autoimmune and “other” subgroups precluded us from performing analysis of variance across all etiological subgroups.
Conclusion
We have, for the first time, described an Australian LTS population. In keeping with similarly large reviews, we have demonstrated that indeed the LTS cohort is comprised of distinct, homogeneous etiological subgroups, each with differing disease morphology and response to treatment. Further, we have demonstrated that patient, rather than surgical factors, affects treatment outcomes of tracheotomy incidence and dependence. This may have future implication for patient monitoring and patient selection for surgery.
Footnotes
Authors’ Note
All work was performed at Monash Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.