
Abstract
Purulent chondritis of the thyroid cartilage is a rare affliction that is not frequently observed in patients undergoing laryngeal surgery. The formation of abscesses between the inner and outer perichondria can cause constriction of the laryngeal lumen, leading to hoarseness and difficulty breathing. This report details the case of a middle-aged diabetic woman who experienced swelling in the tissue of her laryngeal cavity and destruction of her thyroid cartilage plate after undergoing laryngectomy. The pathological examination revealed evidence of inflammation, and the patient was ultimately diagnosed with purulent chondritis of the thyroid cartilage.
Introduction
Purulent chondritis of the thyroid cartilage is a condition characterized by inflammation of the laryngeal framework cartilage and the formation of abscesses between the inner and outer perichondria. Patients typically present with hoarseness and dyspnea due to narrowing of the laryngeal lumen. Most cases resolve with symptom management. 1 Causes of the condition include prolonged intubation, autoimmune diseases like relapsing polychondritis, previous radiotherapy, allergies, and trauma. 2 Although rare, the condition can be life-threatening if it causes difficulty breathing.
Although not officially linked, uncontrolled blood glucose levels associated with diabetes mellitus may play a role in the development of purulent chondritis after surgical removal of a laryngeal tumor. This is because uncontrolled blood glucose can lead to postoperative complications such as infection and focal ischemia. 3 This report describes a case of purulent chondritis of the thyroid cartilage after tumor removal, where uncontrolled blood glucose may have contributed to the development of the condition.
Case Presentation
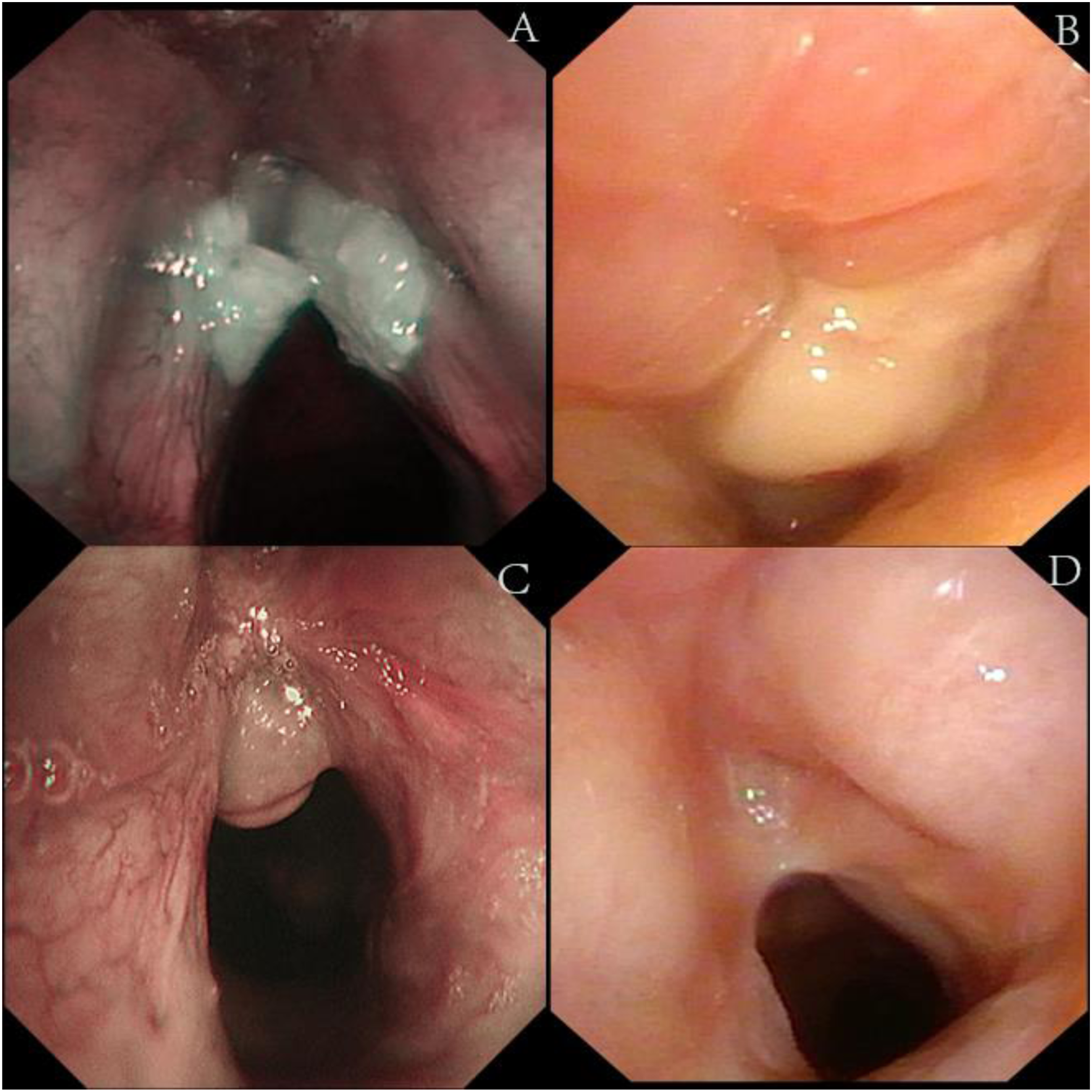
A 69-year-old female with a history of type II diabetes mellitus and hypertension presented with worsening hoarseness that had started 2 months prior. A CT scan and laryngoscopy showed an irregular mass located on the anterior commissure affecting both vocal cords and covered by a white pseudomembrane (Figures1A and 2A). The patient's diabetes was poorly controlled, indicated by an HbA1c of 8.9%. (A) The CT scan upon admission revealed that the left aryepiglottic fold and the posterior wall of the laryngopharynx were thickened and intensified irregularly. Additionally, the left pyriform fossa appeared slightly shallower; (B) the CT scan performed before second surgery revealed that the wall of the laryngopharynx was significantly thickened and displayed heterogeneous enhancement. There was also evidence of laryngeal stenosis. (A) The laryngoscopy upon admission revealed that a mass was present in the anterior portions of both vocal cords and involved the anterior commissure. The surface of the mass was rough, white pseudomembranes were attached, and the glottis was not closing properly. (B) The laryngoscopy revealed laryngeal stenosis, swelling of the laryngeal mucosa, and purulent secretions on the surface. (C) The laryngoscopy revealed the presence of granulation tissue at the anterior vocal cord junction. (D) The laryngoscopy revealed that the laryngeal mucosa was smooth.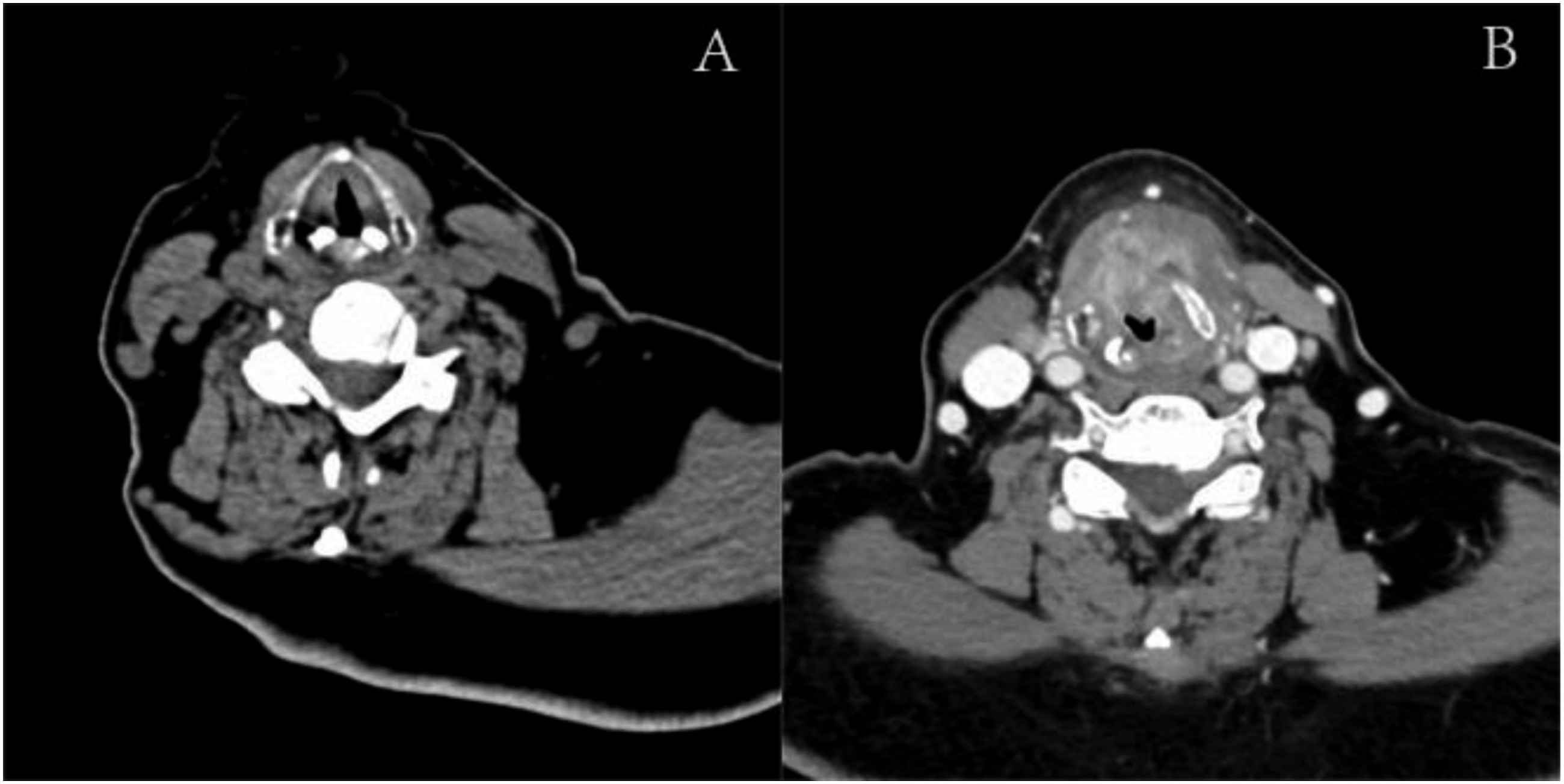
The patient underwent transoral CO2-laser surgery to remove the mass, which was found to be high-grade intraepithelial neoplasia after the pathological exam. Despite being on medication, the patient's blood sugar remained poorly controlled during the hospital stay (morning fast blood glucose (FBG) ranged from 9.7 to 11.4 mmol/L, postprandial blood sugar ranged from 8.4 to 15.3 mmol/L).
One month later, the patient was admitted for second degree laryngeal obstruction and underwent an emergency tracheotomy. The CT scan showed thickening and enhancement of the laryngopharyngeal wall (Figure 1B). HbA1c was 9.6% (normal range 4.5-6.1%), white blood cell count (WBC) was 9.47 × 10^9/L, neutrophil ratio was 76.7% and the neutrophil count was 7.62 × 10^9/L. At the surgery, the laryngeal cavity was found swollen, and the strap muscles adhered tightly to the thyroid cartilage (Figure 3). The thyroid cartilage was found to be partially necrosed and an abscess had formed, leading to a diagnosis of inflammatory necrosis. Despite being on insulin, the patient's blood glucose remained poorly controlled during this hospital stay. The picture in the second surgery showed a swollen laryngeal cavity and tight adhesion of the strap muscles to the thyroid cartilage, the thyroid cartilage was partially necrotic, and a prelaryngeal tissue abscess had formed.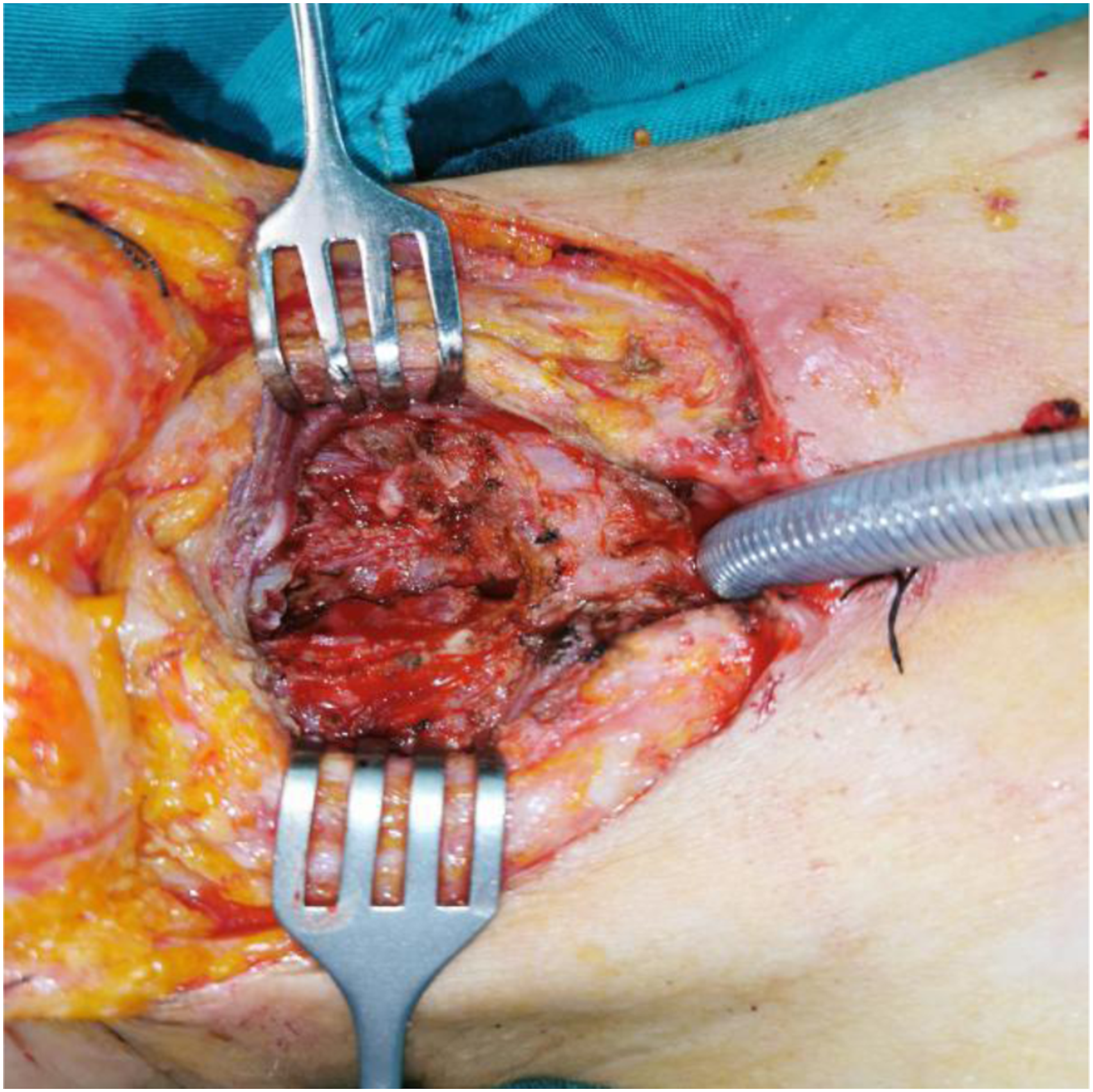
The patient made an uneventful recovery and was discharged with a tracheostomy tube, which was removed 3 months later (Figure 2C). At the next follow-up 3 months later, the patient was in good condition with only mild hoarseness and a laryngoscopy showed no pathological changes (Figure 2D). The tracheocutaneous fistula was closed.
Discussion
Laryngeal purulent chondritis is an inflammation of the cartilages in the larynx, including the thyroid, cricoid, epiglottic, and arytenoid cartilages. The causes of chondritis may include prolonged intubation, autoimmune diseases, previous radiotherapy, allergies or trauma. 1 While literature has reported on idiopathic or post-radiotherapy/chemotherapy laryngeal chondritis,4 -7 purulent chondritis of the thyroid cartilage after laryngeal tumor resection is not well documented.
CT scans of this condition can resemble tumor recurrence, making it challenging to distinguish between the two without a biopsy. Despite laryngoscopic findings and laboratory results suggesting inflammation, tumor recurrence cannot be excluded without further examination. Misdiagnosing tumor recurrence as inflammation may delay treatment, making reoperation a preferable option.
The patient's laryngeal purulent chondritis may have been partially caused by her uncontrolled diabetes. Despite a lack of direct connection between the two, it has been shown that many diabetic patients experience systemic low-grade chronic inflammation.8,9 The underlying mechanism is complex, involving the release of LPS by gut bacteria or periodontal bacteria, as well as excessive levels of leptin or adiponectin from adipose tissue, which can trigger T-cell response, leading to activation of monocytes and neutrophils and secretion of pro-inflammatory substances.10 -12 Surgery, which can be seen as a stimulus, can worsen the inflammatory response resulting from diabetes. 13
In conclusion, patients with uncontrolled diabetes are more susceptible to infection and regional inflammation. When a laryngeal tumor patient with uncontrolled blood sugar experiences laryngeal obstruction or edema, laryngeal chondritis should be considered as a possible diagnosis. Proper management of the patient's blood sugar levels before and after surgery is important for a better postoperative recovery and to reduce the risk of reoperation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by the Technology Department of Sichuan Province. The project is named the “Key Research and Development Program of Sichuan Province” (2022YFS0065).
Ethics Approval and Consent to Participate
All therapeutic options were approved by the Ethics Committee of West China Hospital, Sichuan University and all medical records were obtained with the consent of the patient.
Consent for Publication
Before obtaining the original data and writing the article, informed consent was obtained from the patient.