
Abstract
Keywords
Introduction
Laryngeal squamous cell carcinoma (LSCC) is one of the most common tumors of the head and neck. Approximately 60% of patients present with advanced (stage III or IV) disease at diagnosis. Although concurrent systemic therapy, radiation therapy, and induction chemotherapy have been accepted standards of care, surgery remains the mainstay for patients with advanced LSCC, especially those with stage T4 cancers. 1 A study using the National Cancer Database found that there was a statistically significant survival benefit for patients with T4a laryngeal cancer who underwent total laryngectomy versus larynx preservation chemoradiation. 2
According to the NCCN Guidelines for Head and Neck Cancers (Version 1.2021), a thyroidectomy is suggested as a routine measure during total laryngectomy in patients with advanced LSCC. LSCC can invade the thyroid gland by direct extension or, less frequently, spread indirectly by lymphatic or vascular channels. 3 Hilly et al. reported that thyroid gland invasion was associated with poor overall survival. 4
In contrast, some investigators examining postoperative complications of hypothyroidism have not supported thyroidectomy during total laryngectomy. The incidence of hypothyroidism after total laryngectomy with hemithyroidectomy can be as high as > 50%.5,6 And the addition of postoperative radiotherapy which is mostly applied in advanced laryngeal cancers may increase this morbidity of hypothyroidism. Although simple to treat in some, postoperative hypothyroidism can be difficult to treat in others, and postoperative thyroid function needs to be followed up for > 2 years. 7 It is associated with various morbidities including delayed wound healing, pharyngeal fistula, mood depression, hypercholesterolemia with irreversible damage to the vascular system, and cardiac morbidity. 8 Hypoparathyroidism is a most common complication of total thyroidectomy and it is a much serious complication than hypothyroidism, which can cause hypocalcemia and lead to tetany, ventricular tachycardia, ventricular fibrillation, and mental symptoms. 9 A 12-year retrospective study reported that thyroid-preserving laryngectomy did not increase the local recurrence rate and did not have a negative effect on disease-free survival. 10
Many predictors for thyroidectomy during laryngectomy have been reported in the literature. Some authors have recommended that thyroidectomy may be required only for patients considered to be at risk, such as those with thyroid cartilage invasion and tumors with subglottic extension > 10 mm. Mendelson et al. indicated that thyroidectomy may only be required during total laryngectomy for transglottic and subglottic tumors and tumors with subglottic extension >10 mm. 11 Gorphe et al. reported that thyroid cartilage invasion was a significant factor associated with thyroid gland invasion. 12
To achieve local tumor control and improve patient prognosis, while reducing postoperative complications and improving quality of life, it is necessary to explore positive predictors of thyroid gland invasion in LSCC. In this study, we collected clinical and pathological data from patients with advanced LSCC undergoing total laryngectomy with thyroidectomy to identify predictors of thyroid gland invasion. We aimed to investigate the incidence of thyroid gland invasion to facilitate decision-making regarding whether to perform thyroidectomy during total laryngectomy.
Patients and Methods
In our study, data from 113 patients, who underwent total laryngectomy with thyroidectomy for advanced LSCC at Guangdong Provincial People’s Hospital (Guangzhou, China) between 2009 and 2019, were retrospectively analyzed. Inclusion criteria were as follows: patients with pathologically confirmed LSCC, staged as III or IV according to American Joint Committee on Cancer (AJCC) criteria, 8th Edition; surgery performed at Guangdong Provincial People’s Hospital as primary or salvage treatment; and total laryngectomy with partial or total thyroidectomy. Individuals with laryngeal carcinoma of other pathological types and those with LSCC who did not undergo preoperative examination or surgery at Guangdong Provincial People’s Hospital were excluded from the study.
Preoperative clinical data, pathological characteristics, and demographic information were collected, including previous treatment(s), laryngoscopy findings, computed tomography (CT), or/and magnetic resonance imaging (MRI) reviews, as well as the type of surgery and intraoperative evaluation. Radiological assessment was evaluated by two experienced radiologists who were blinded to patient information. If the assessments of the 2 radiologists were not identical, a third radiologist evaluated the films, and his assessment was used as the final result.
Eighty-four cases with complete data and 19 factors were statistically analyzed using SPSS version 25.0 (IBM Corporation, Armonk, NY, USA) for Windows (Microsoft Corporation, Redmond, WA, USA). Univariate analysis was performed using t-test/Fisher’s exact test, and multivariate analysis was performed using binary logistic regression analysis. A new predictor was proposed using a parallel test, which means if either or both of two predictors are positive, the joint predictor was judged to be positive. Moreover, the sensitivity and specificity of the positive predictors were calculated to construct a receiver operating characteristic (ROC) curve. Differences with P < 0.05 were considered to be statistically significant.
All procedures performed in this study were in accordance with the ethical standards of Research Ethics Committee Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Science (No.GDREC2019755H).
Results
Characteristics of Patients With Laryngeal Squamous Cell Carcinoma Who Underwent Laryngectomy and Thyroidectomy.
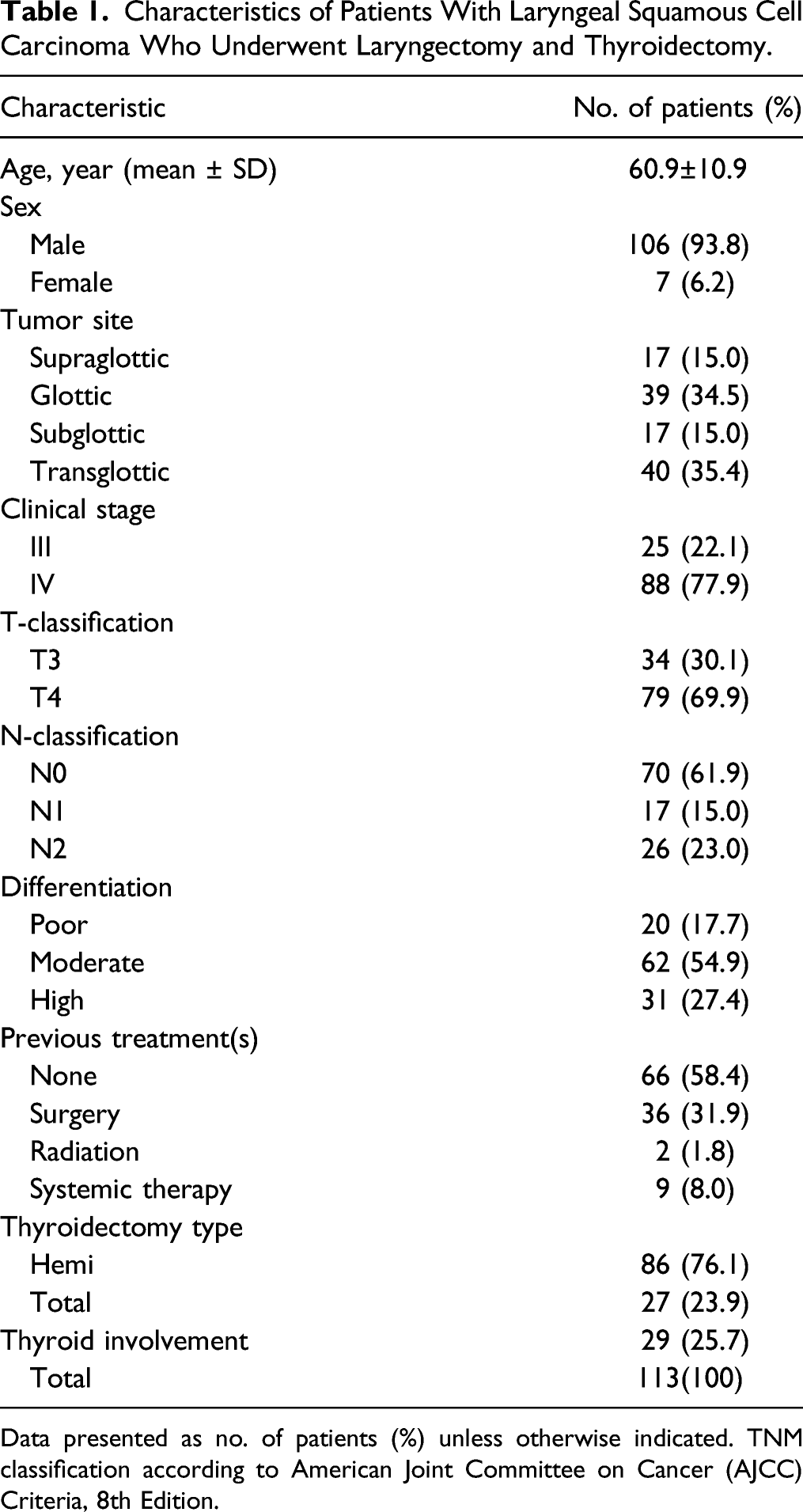
Data presented as no. of patients (%) unless otherwise indicated. TNM classification according to American Joint Committee on Cancer (AJCC) Criteria, 8th Edition.
Characteristics of 84 Patients and Their Association With Thyroid Invasion.
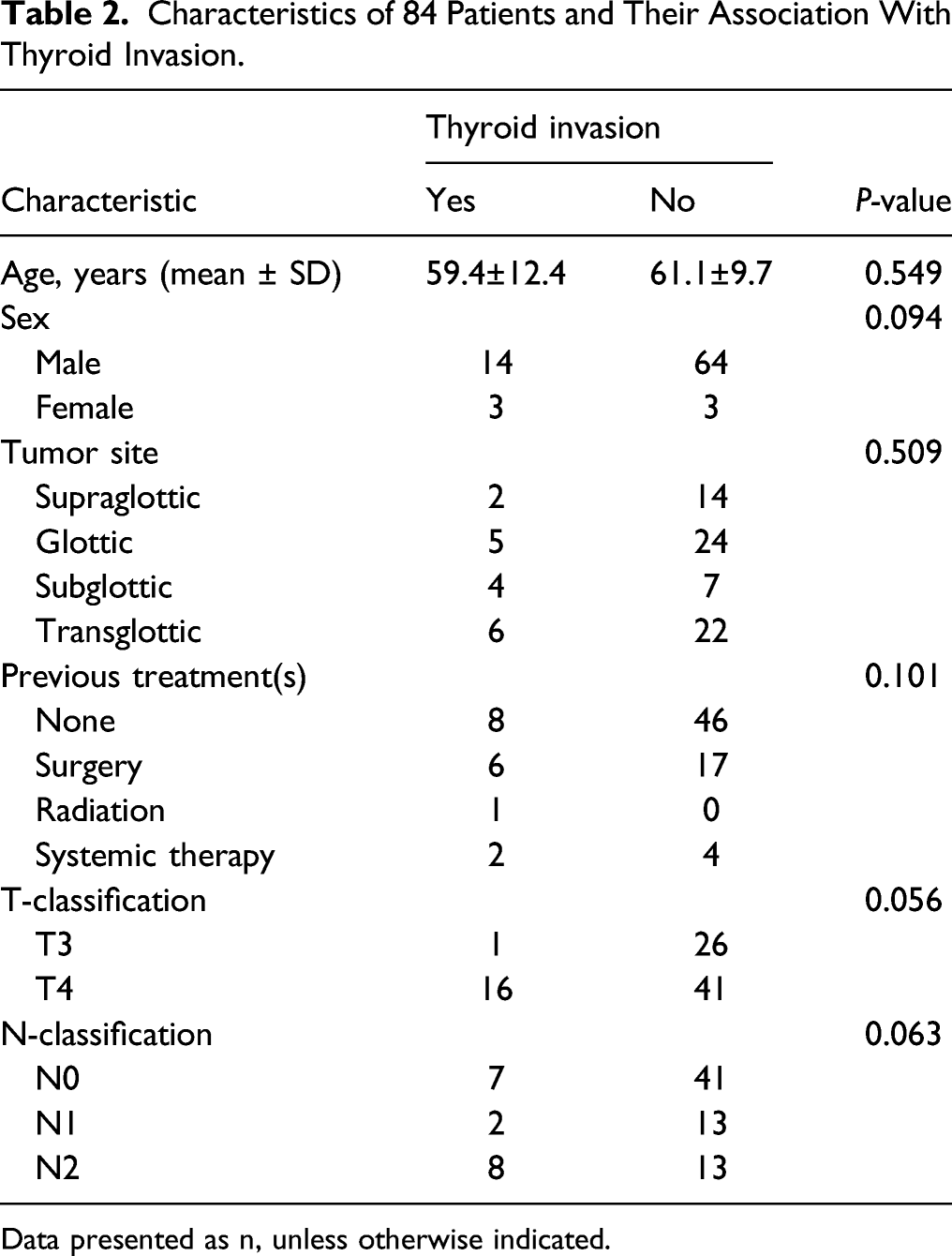
Data presented as n, unless otherwise indicated.
Predictors Associated With Thyroid Invasion.
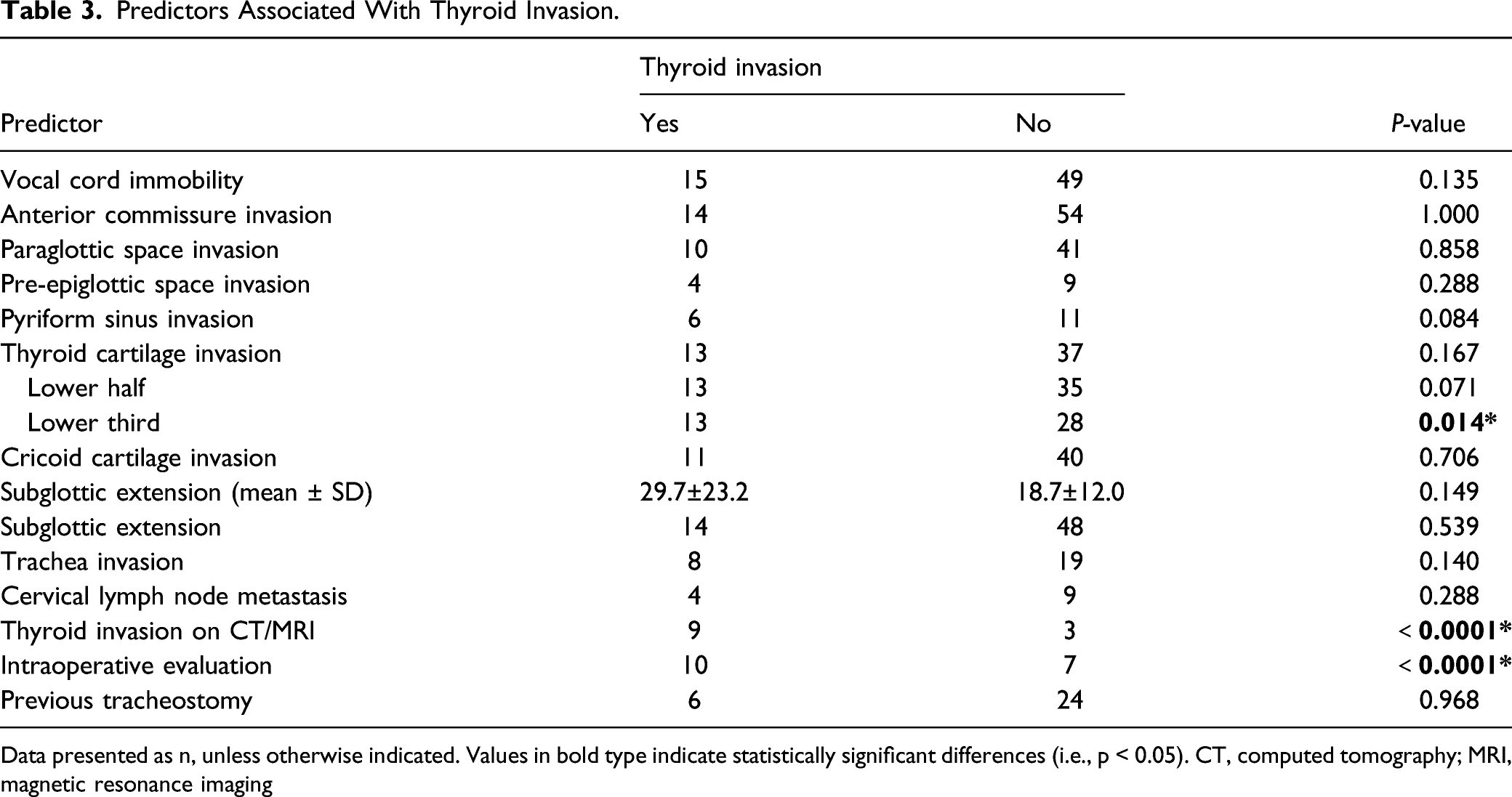
Data presented as n, unless otherwise indicated. Values in bold type indicate statistically significant differences (i.e., p < 0.05). CT, computed tomography; MRI, magnetic resonance imaging
Multivariate Analysis Using the Binary Logistic Regression Test.

Value in bold type indicates a statistically significant difference (i.e., p < 0.05). CI, confidence interval; CT, computed tomography; MRI, magnetic resonance imaging; OR, odds ratio
Sensitivity (Se), Specificity (Sp), and Positive and Negative Predictive Values (PPV and NPV) of Positive Predictors.

A//C: If either A or C is positive, it is denoted as positive. CT, computed tomography; MRI, magnetic resonance imaging
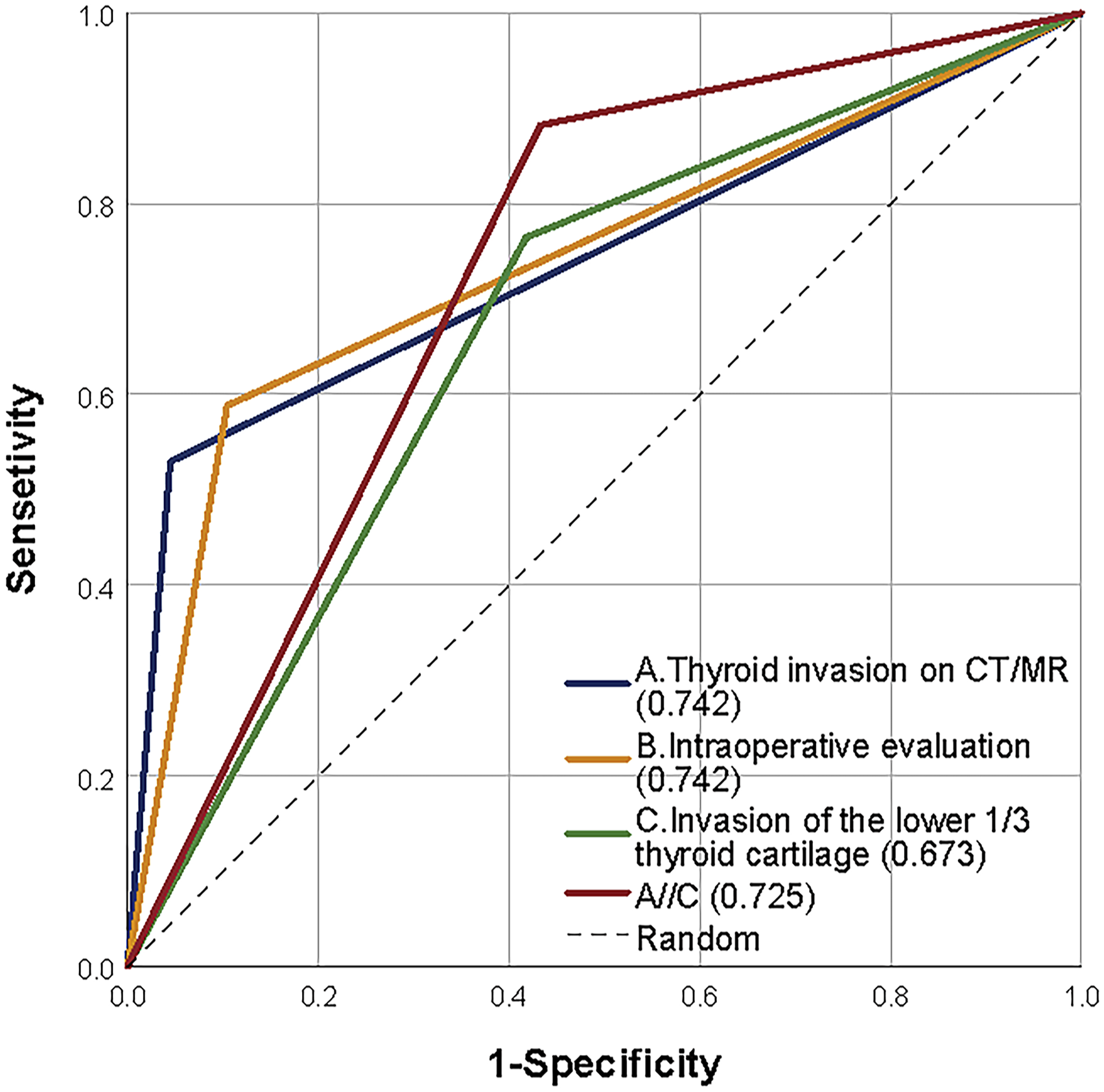
Receiver operating characteristic (ROC) curve of positive predictors. Area under the ROC curve (AUC) is presented in parentheses.
Discussion
Our data demonstrated that, among 113 patients with thyroidectomy and total laryngectomy, the probability of thyroid invasion was 25.7%. In univariate analysis, statistically significant predictors included invasion of the lower third of thyroid cartilage, thyroid gland invasion on CT/MRI, and intraoperative evaluation. In multivariate analysis, only thyroid gland invasion on CT/MRI was statistically significant. To our knowledge, this was the first study to use invasion of the lower third of thyroid cartilage as a predictor, which was measured by radiologists on raw imaging data. We found that it had a statistically significant relationship with thyroid gland invasion in univariate analysis, with a sensitivity of 76.5%. Because the sensitivity of thyroid gland invasion on CT/MRI and intraoperative evaluation was not high, we used a parallel test to jointly predict and increased the sensitivity to 88.2%.
Indications for thyroidectomy during total laryngectomy remain controversial. In the present study, we proposed a new predictor that combined invasion of the lower third of thyroid cartilage and thyroid gland invasion on CT/MRI. It improves the sensitivity of thyroid gland invasion on CT/MRI and reduces the missed diagnosis. At the same time, a negative predictive value of 95% means that it can distinguish patients who do not need thyroidectomy commendably. If our results are further validated, improved strategies based on these predictors may be used to identify patients with a higher risk for thyroid gland invasion in total laryngectomy for advanced LSCC.
Several studies have shown that subglottic extension was the only statistically significant factor in thyroid gland invasion. 13 Since the thyroid gland is located in front of the 2/3/4 tracheal rings and below the glottis, laryngeal tumor with subglottic extension may invade the thyroid gland directly. In our study, the subglottic extension was emphatically analyzed as a categorical variable and a continuous variable. However, the P-values obtained showed no statistical correlation with thyroid gland invasion, regardless of the tumor site. Thus, our current study might not suggest that subglottic extension was the predictor in thyroid gland invasion. We hypothesized that subglottic invasion might be less important than previous studies had thought, and thyroid cartilage invasion was more valuable. It may be the same as Strome et al’s claim that tumor progression occurs mainly in the paraglottic space and extralaryngeal compartments and the potential for mucosal diffusion is limited. 14 LSCC may spread to extralaryngeal tissue via a variety of paths. 15 Lesions spread downward through thyroid cartilage, cricoid cartilage, and cricothyroid membrane; laterally through paraglottic space along the conus elasticus of the trachea; and laterally outside the skeletal framework of the larynx through the cricopharyngeal muscle, cricothyroid muscle, and surrounding fascia. 16 Also, it might be related to the inadequate number of cases and the ethnicity of the study group. More cases and studies of different human species are needed to explain this.
Cartilage invasion has been reported to be a predictor of thyroid gland invasion. 17 However, the difference in our study was that there was no statistical relationship between thyroid cartilage invasion and thyroid gland invasion (P = 0.167). Considering that most cases of thyroid gland invasion occur by direct extension, 18 and the thyroid gland is adjacent to the lower part of the thyroid cartilage, we believe that the lower part of the thyroid cartilage may be more related to thyroid gland invasion. We then analyzed the relationship between invasion of the lower half and lower third of thyroid cartilage invasion and thyroid gland invasion, respectively. Univariate analysis revealed that invasion of the lower third of thyroid cartilage could be used as a predictor of thyroid gland invasion. It indicated that whether a thyroidectomy was performed in a patient with LSCC could not be predicted by invasion of the upper and middle part of thyroid cartilage.
Preoperative CT is an effective method for ruling out thyroid gland invasion. 19 The negative predictive value in our study (88.9%) supports this concept. However, local control of the tumor is critical. The sensitivity (52.9%) predicted by thyroid gland invasion on CT/MRI means that nearly one-half of patients were underdiagnosed according to thyroid gland invasion, which would lead to a poor prognosis for these patients. As a solution, we introduced invasion of the lower third of thyroid cartilage, which was a more sensitive predictor related to thyroid gland invasion for joint prediction. When patients with advanced LSCC exhibited invasion of the lower third of thyroid cartilage or/and thyroid gland invasion on CT/MRI, the predictor was markedly positive and thyroidectomy was recommended. Its sensitivity increased to 88.2% and negative predictive value increased to 95%. This indicated that 88.2% of patients with thyroid gland invasion could be identified using this new predictor, which demonstrated a correct probability of 95% that the new predictor reflected an uninvaded thyroid gland.
In previous studies, the incidence of thyroid gland invasion in advanced laryngeal cancer ranges from 1% to 30%.20,21 The incidence of thyroid gland invasion fell within this range in the present study. In 2013, a meta-analysis reported an overall pooled incidence of thyroid gland invasion in 1287 patients of 10.7%. 22 In other words, it is unnecessary for nearly 90% of patients to undergo thyroidectomy during total laryngectomy. Thyroidectomy must not be performed routinely. 23 Therefore, thyroidectomy may only be required during total laryngectomy for selected cases involving tumors invading the lower third of thyroid cartilage or/and thyroid gland invasion on CT/MRI. The new predictor may inform surgeons as to whether to perform thyroidectomy during total laryngectomy for patients with advanced LSCC. It emphasizes the importance of preoperative evaluation and made a tradeoff between ensuring local control of tumor(s) and reducing postoperative complications, which would promote individualized treatment.
There were limitations to the present study, the first of which were its retrospective, single-center design. Second, the study population was the one that selected for thyroidectomy with laryngectomy by the surgeon’s existing criteria and the data has selection bias relating to the prevalence of thyroid gland invasion. Third, because some patient medical records were incomplete, the number of cases that were analyzed was reduced. Moreover, there may have been latent thyroid gland invasions that remained undetected. The caution should be exercised among potential predictors such as T-classification (P = 0.056), N-classification (P = 0.063), and lower-half thyroid cartilage invasion (P = 0.071) as their P-value was close to 0.05 in our results. Large-scale, prospective, and multicenter studies are needed in the future.
Conclusion
In the present study, 25.7% of patients with advanced LSCC exhibited thyroid gland invasion. A new predictor that combined invasion of the lower third of thyroid cartilage and thyroid gland invasion on CT/MRI was associated with thyroid gland invasion. Thyroidectomy may be required during total laryngectomy for selected cases involving tumors that invade the lower third of thyroid cartilage and/or thyroid gland invasion on CT/MRI. In the future, more validation studies are needed to confirm this.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Science and Technology Program of Guangzhou City, China (201707010489 to Z.L.) and the Matching Scientific Research Fund for Guangdong Provincial Outstanding Young Medical Talent by Guangdong Provincial People’s Hospital (KJ012019453 to Z. L).