
Abstract
Branchial cleft cyst arising within the parotid space is considered an extremely rare phenomenon. In contrast, cystic squamous cell carcinoma in the lateral neck is not an uncommon presentation of HPV-related head and neck cancer. Although they have singly been narrated in literature, simultaneous expression of these anomalies has yet to be reported. We describe a case of synchronous presentation of branchial cleft cyst of the right parotid gland and cystic metastatic squamous cell carcinoma of the left neck. These findings are discussed in light of the challenges in fine needle aspiration biopsy of cystic masses, and the risk of two distinct pathologic entities presenting as cysts in the head and neck.
Background
Squamous cell carcinoma (SCC) accounts for the majority of all head and neck malignancies and is the sixth most common cancer worldwide.1,2 Most are derived from the mucosal epithelium of the head and neck and their increased incidence may be attributed to rising tobacco use, alcohol consumption and human papillomavirus (HPV) infections, primarily HPV-16.3-5 In some patients, HPV-related oropharynx cancer can present as a cystic mass, usually located in level 2a of the neck. In contrast, parotid branchial cysts are congenital malformations of the first branchial cleft which are exceptionally uncommon and poorly understood. 6 Due to their rare nature and similar signs and symptoms, many are initially mistaken as parotid tumors.
While FNA biopsy is the mainstay of diagnostics for parotid neck masses, this modality can be limited in the evaluation of cystic masses because of the paucicellular nature of the cyst fluid. In patients with multiple cystic masses in various spaces of the head and neck, the limitations of FNA biopsy can create a diagnostic challenge.
To our knowledge, we report the first case of a coexisting presentation of parotid branchial cyst and SCC of the neck.
Case Presentation
Patient Information
A 66-year-old female patient seeking medical consultation with complaints of two masses in her head and neck arising simultaneously over 2 months. Physical examination confirmed a cystic mass of the left neck and the right parotid. The patient reported tenderness on the right parotid cyst but not the left neck. She had a body mass index (BMI) of 33.48 kg/m2 and disclosed no previous alcohol or tobacco use. The remainder of her medical history was noncontributory.
Diagnostic Assessment
Ultrasound-guided fine needle aspiration (FNA) using a 23 G needle was performed for both masses. Three passes were made in the left neck and one in the right parotid mass. All four specimens grossly revealed a thick, yellow, cystic-like fluid. The right parotid FNA showed non-specific inflammatory cells and cystic debris. The left neck FNA was reported as “metastatic squamous cell carcinoma positive for HPV-16/18” (Figure 1). A contrasted computed tomography (CT) scan demonstrated a cystic necrotic mass or conglomerate of necrotic lymph nodes situated posterior-inferior to the right mandible and additional enlarged lymph nodes in bilateral upper necks. Of note, a positron-emission tomography (PET)/CT scan demonstrated a standardized uptake value (SUV) of 13.2 in the left level 2a cystic mass but no obvious mucosal primary and faint uptake in the right parotid cyst. Metastatic squamous cell carcinoma to the neck lymph node. (A) fine needle aspiration smear (papanicolaou stain, original magnification × 200); (B) cell block section (CB) (H&E stain × 200); (C) Immunohistochemistry for p16 is positive (CB, × 200); (D) HPV high-risk 16/18 by HPV RNA in-situ hybridization is positive (CB, × 200).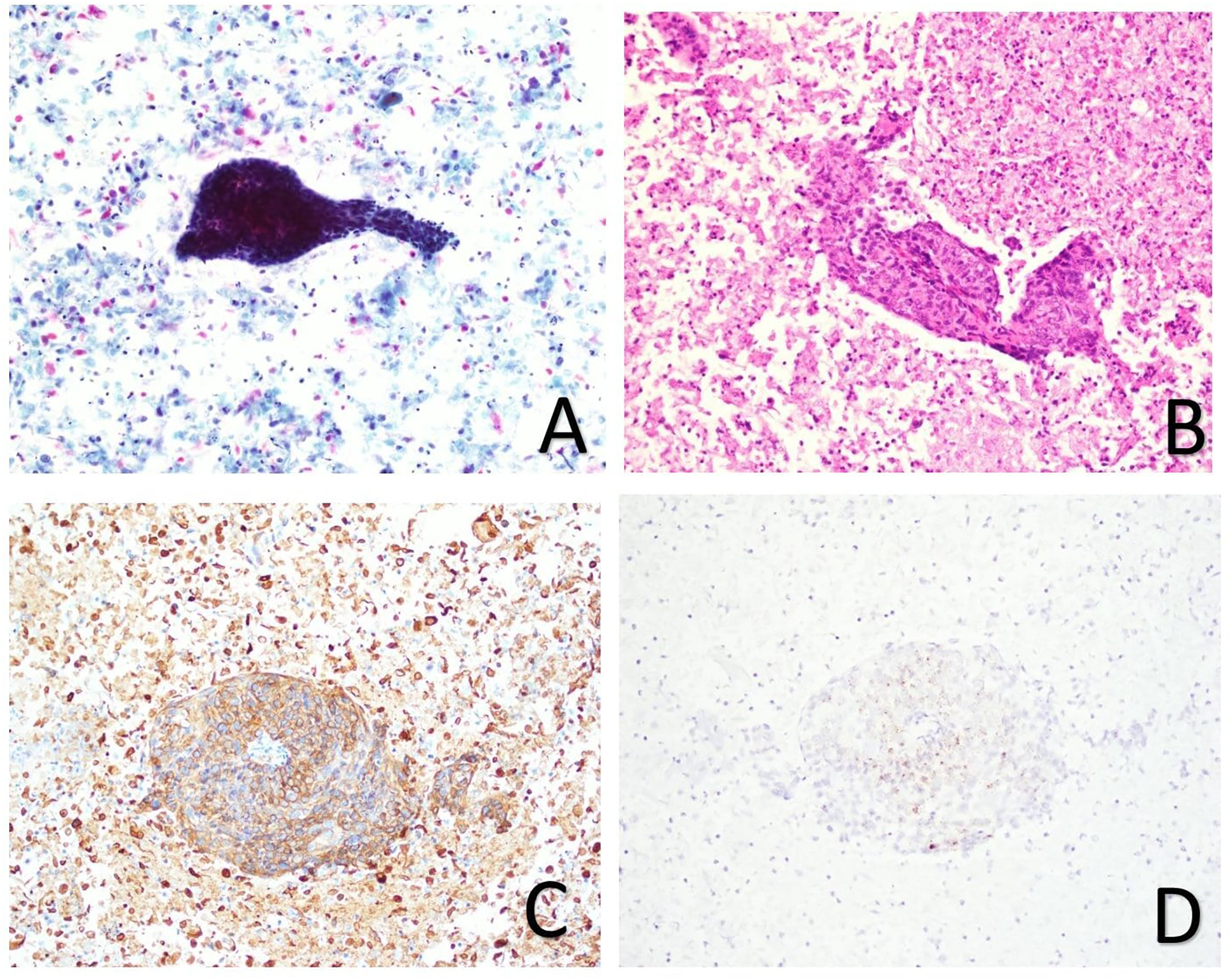
Therapeutic Intervention
The patient underwent a right parotidectomy with facial nerve dissection and laryngoscopy with biopsies. The final pathology revealed a parotid ruptured branchial cleft cyst (Figure 2). Diagnostic palatine tonsillectomy and laryngoscopy with directed biopsies did not reveal a primary site of squamous cell carcinoma. Parotidectomy specimen showing branchial cleft cyst. (A) Squamous cell lined cyst (H&E stain, × 100); (B) immunohistochemistry for CK5/6 is positive, confirming squamous cell lining (× 40); (C) immunohistochemistry for p16 is negative (with some non-specific staining) (× 40).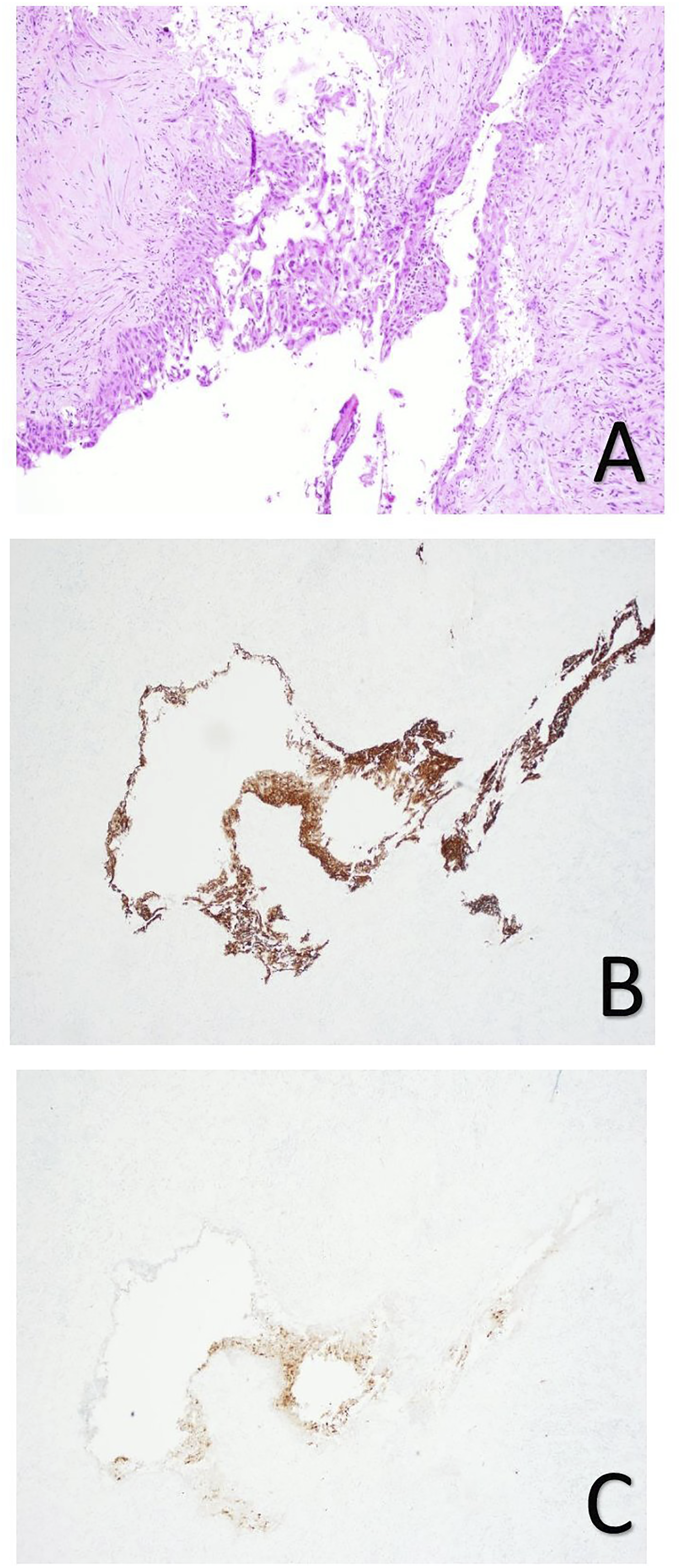
Discussion
Branchial cleft cysts (BCCs), also known as lymphoepithelial cysts, are remnants of the branchial arch that clinically present as enlarged masses. 7 Although they are categorized as congenital anomalies, BCCs have an uncommon tendency to occur later in life. The anatomical location of these lesions is dependent on which branchial cleft fails to obliterate during embryological development. The first case of a parotid gland BCC was reported by Hildebrant in 1895. 8 They are extremely rare accounting for <1% percent of all diagnosed BCCs. 9 Their manifestation within the parotid gland makes them a diagnostic challenge, often initially being misdiagnosed as parotid tumors. Various preoperative techniques may be used to aid in establishing the diagnosis. Ultrasound-guided fine needle aspiration is typically performed first. This is followed by supplementary imaging such as CT scan and/or magnetic resonance imaging (MRI) which are helpful due to their ability of differentiating solid from cystic lesions within the parotid gland. 10 Following diagnostic confirmation, surgical excision is the gold-standard for treating parotid gland BCCs. Careful and meticulous planning and execution by the surgeon is critical to avoid collateral damage to the facial nerve and other nearby structures.
In contrast to parotid BCC, human papillomavirus-related squamous cell carcinoma (HPSCC) of the head and neck is one of the most common malignancies worldwide. It typically presents as large cystic metastases with a known or unknown primary. While overall incidence of head and neck HPSCC is declining, oropharyngeal HPSCC is steadily on the rise. 11 Lifestyle choices of increased alcohol and tobacco (smoking, chewing) use are the two most important risk factors. Diagnostic tools such as CT, MRI and/or PET scan, along with surgical biopsy are used to confirm disease presence, tumor burden and assess the current stage of the disease process. Treatment for HPSCC is multimodal consisting of surgery, chemotherapy, and radiation. Patients often receive only palliative care due to advanced age, delayed diagnosis and increased disease severity.
There are a wide variety of pathologic entities that may present with cystic masses in the head and neck, including HPV-related SCC, papillary thyroid carcinoma, salivary gland tumors such as Warthin’s, lymphangiomas, ranula, HIV-related parotid cysts as well as other infections and congenital lesions. In this patient, it would have been false to assume that one pathologic entity was responsible for both right parotid and left neck cyst. The diagnostic workup is confounded by the relatively low sensitivity of FNA biopsy for cystic masses. While the PET scan suggested a left neck malignancy, the lack of uptake in the right parotid does not definitively exclude malignancy. Complete surgical excision of the right parotid cyst was warranted to confirm that this indeed was a simultaneous presentation of HPV-related SCC and a congenital type 1 branchial cleft cyst. The patient was subsequently referred for chemoradiation of the left neck. This case demonstrates that in the diagnostic evaluation of multiple head and neck cysts, one must resist the temptation to assume that all cysts are derived from the same pathologic process.
Conclusion
This case demonstrates the importance of careful and methodical analysis to correctly identify coexisting pathologies of parotid branchial cleft cyst and metastatic SCC of the neck. We share our experience of successfully diagnosing these synchronous masses of independent etiologies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for this article’s research, authorship, and publication.
Ethics Approval and Consent to Participate
All clinical specimens were obtained under the approval of the Institutional Review Board. Informed consent was obtained from the subject.
Consent for Publication
Informed consent was obtained from the patient for publication of this case report. A copy is available upon reasonable request.
Availability of Data and Materials
All data and materials used for this case report are available from the corresponding author upon reasonable request.