
Abstract
Objectives
This study aimed to measure the supraorbital ethmoid cell (SOEC) and characterize the relationship between the degree of SOEC pneumatization and the position of the anterior ethmoidal artery (AEA) in relation to the skull base.
Methods
Computed tomography (CT) scans of 100 patients were analyzed. The correlation between the pneumatization of SOEC and the distance of the AEA from the skull base was explored by Spearman’s correlation rho efficient test.
Results
The distance of the AEA from skull base was 3.10 (2.60,3.60) mm in patients with SOEC compared with 0.6(0.40,2.10)mm in those without(P < .001). In 50.5% of the patients, the AEA was located below the skull base; the incidence of this localization was significantly higher in those with SOEC than in those without (78.79%vs22.77%, P < .001). Compared to female patients, male patients owned greater SOEC height (9.65vs8.20mm, P = .007). The SOECs volume (r = 0.45, P < .001), height (r = .30, P = .003), and transverse diameter (r = 0.28, P = .005) were all significantly correlated with the distance of the AEA from the skull base.
Conclusions
The pneumatization of SOEC critically impact the distance between the AEA and skull base. The higher the degree of pneumatization, the farther from the skull base the AEA will be, increasing the risk of complications during nasal endoscopic surgery. These results provide an important reference for protecting the AEA during nasal endoscopic surgery.
Keywords
Introduction
Nasal endoscopic sinus surgery (NESS) is the main surgical method in rhinology. 1 Successful surgery depends on the removal of the blockage in the absence of severe surgical complications. Therefore, it is of great importance for surgeons to identify and protect important structure, such as the anterior ethmoidal artery (AEA).
The AEA is a significant anatomical structure of the anterior cranial fossa and passes through the anterior ethmoidal foramen of the medial orbital wall and enters the anterior cranial fossa. 2 The transethmoid position of the AEA in relation to the anterior skull base shows anatomic variability and has been well studied.3,4 Lannoy-Penisson et al. classified the AEA based on the location of AEA relative to the skull base. 5 Grade I AEA is located within the skull base. It is regarded as grade II when AEA is prominent at the skull base. Grade III AEA is located below the skull base. The risk for arterial injury is increased with grade III AEA. Thus, the factors leading to the position of the AEA below the skull base deserve to be explored. Some researchers have investigated AEA positioning, including the effects of the presence of SOEC and the length of lateral lamella of the cribriform plate (LLCP)on the position of the AEA.3,4,6
The supraorbital ethmoid cell (SOEC) is the anterior ethmoid cell located above the orbital plate immediately posterior to the frontal sinus. SOEC pneumatization extends beyond the most medial plane of the lamina papyracea and is closely related to anterior ethmoidal artery (AEA) anatomy.7,8 The anatomical relationships between the SOEC and frontal sinus can be recognized on coronal, axial, and sagittal computed tomography (CT) images of paranasal sinuses. The SOEC has been demonstrated to be an important anatomical landmark for the location of the AEA. 9
However, to date, only the effect of the SOEC presence on the distance between the AEA and skull base has been evaluated; the relationship between SOEC pneumatization and AEA location has yet to be analyzed deeply. We aimed to analyze the relationship between SOEC pneumatization and the distance of the AEA from the skull base by measuring SOEC-related parameters (the volume, height, and transverse diameter of SOEC). Identifying the location of the AEA before surgery is critical and may help protect the AEA from injury during nasal endoscopic surgery.
Materials and Methods
Data collection and study population
This radiological study was conducted on patients at Nanjing Drum Tower Hospital from February to October 2021. All patients included were over 18 years of age. 100 patients with temporal CT scans were included in this study. Patients with nasal trauma, severe nasal inflammatory disease, nasal tumor, a history of nasal and paranasal sinus surgery, congenital nasal deformities, or other factors that distorted the anatomy of the sinus bone were excluded. CT scans with an unqualified scanning range and poor image quality were excluded. The study was approved by the ethics review committee at the Nanjing Drum Tower Hospital (2022-610). We conducted the research with the verbal consent of the patients.
Radiological measurements
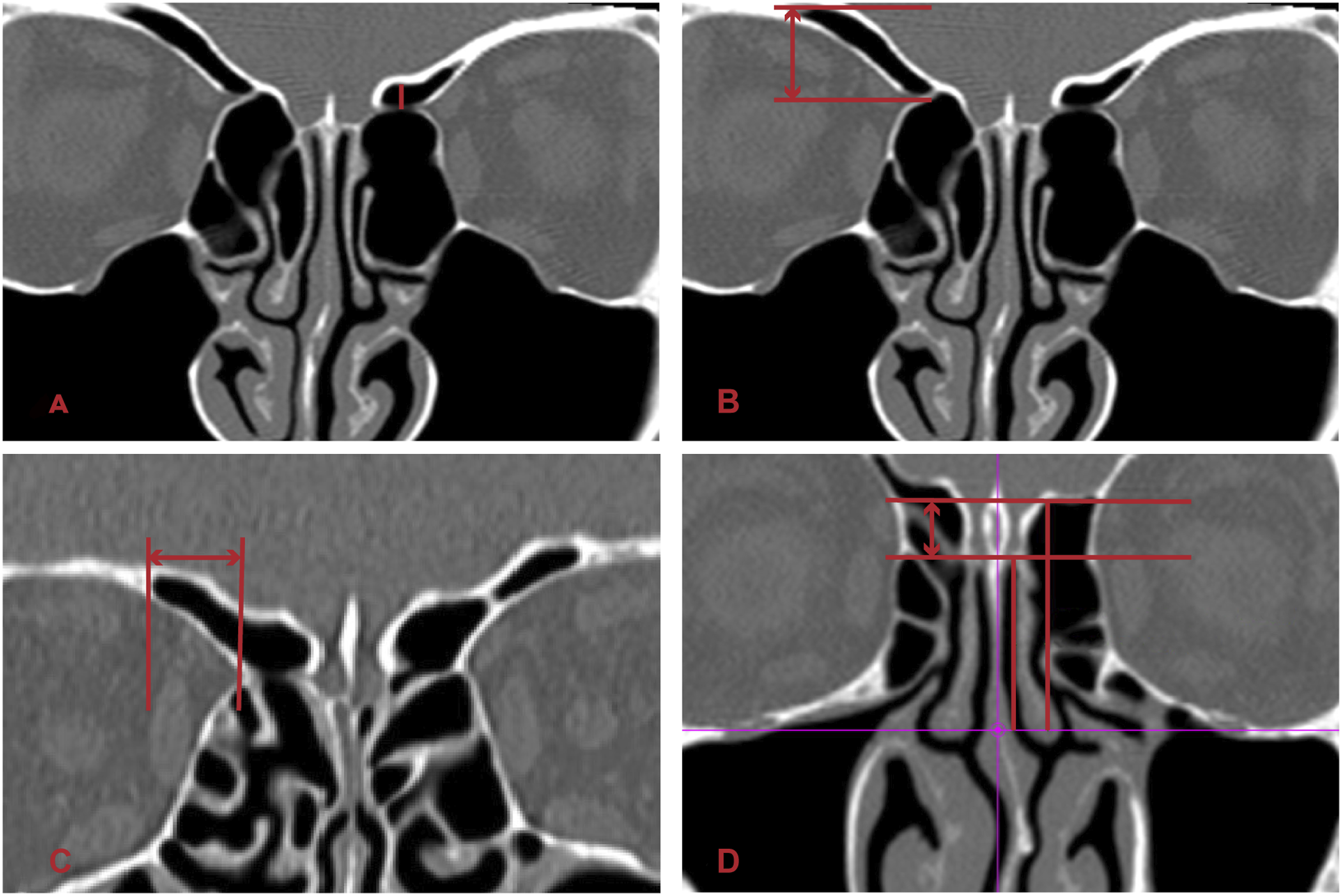
The data were collected from the NEUSOFT PACS system at Nanjing Drum Tower Hospital. All CT scans were reconstructed with the axial reference perpendicular to the level of the hard palate by the United image system (Shanghai, China—slice gap, 0.6mm; slice thickness, 1.1 mm) (Figure 1). The first author determined whether the AEA was below the skull base. When the AEA was far from the skull base, the vertical distance from the midpoint of the intranasal ethmoidal canal to the skull base on coronal views was regarded as the distance from the AEA to the skull base (Figure 2A). The SOEC was recognized by the first author and the attending physician. SOEC height refers to the vertical distance from the highest point of the cell to the exophthalmoid point of the AEA on the horizontal plane (Figure 2B). SOEC transverse diameter (TD) is the distance from the outermost point of the SOEC to the exophthalmoid point of the AEA on the sagittal plane (Figure 2C). To measure LLCP length, we identified the medial ethmoid roof point (MERP), which corresponded to the medial extension of the ethmoid roof (joined with the LLCP) and measured the vertical distance from the MERP to the horizontal plane of the Cribriform Plate (CP) at the first coronal cut to obtain the LLCP length (Figure 2D). We adopted the classification created by Keros
10
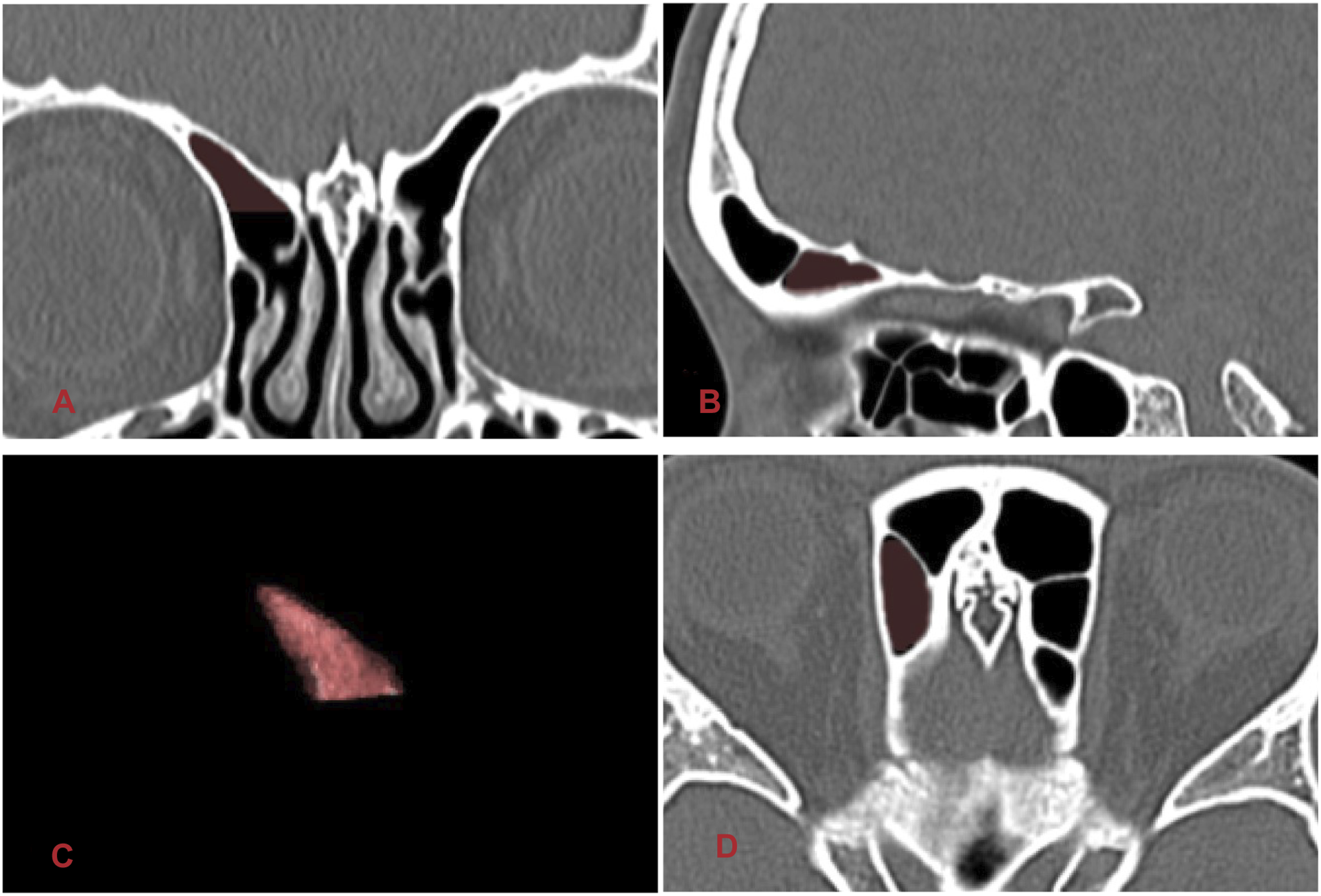
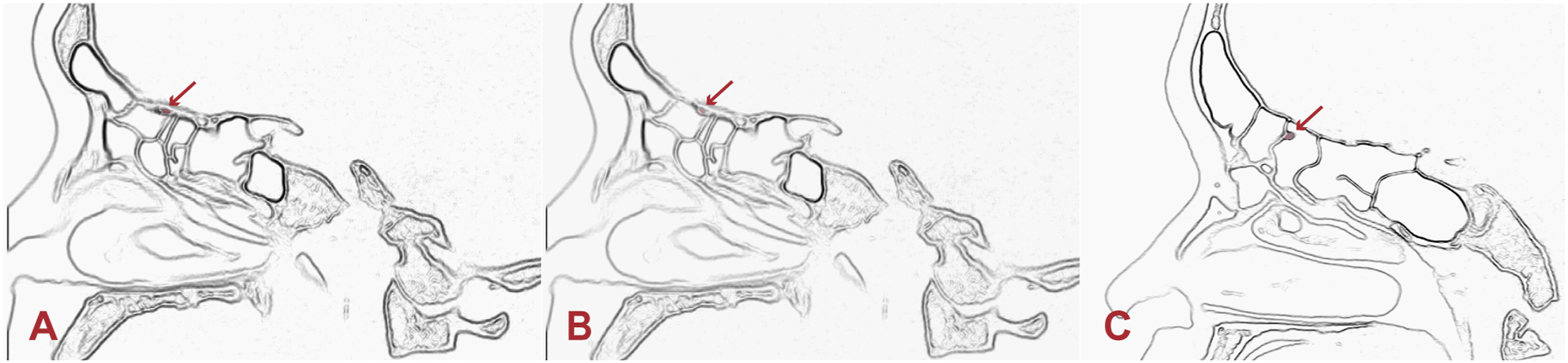
according to the length of LLCP. It belongs to Keros type I when the LLCP length is 1–3mm. The length of 4–7mm is in type II and greater than 7mm in type III. The length of 3.1–7mm was included in type II in our study. There are no clearly defined boundaries among the paranasal sinus cells, which are connected to each other. Therefore, the SOEC volumes reported here represent the volume of all cells above the level of anterior ethmoidal foramen (Figure 3). The AEA can be classified into three grades according to its position relative to the skull base (Figure 4). We adjusted the imaging angle, contrast, and brightness on the image workstation to improve bone resolution. Representative image of the reconstruction of CT images on the axial basis parallel to the level of the hard palate. Radiological measurements on coronal CT. (A)Measurement of the vertical distance of the AEA from the skull base. (B and C) Representative measurement of the height and TD of the SOEC. (D) Representative measurement of the length of the LLCP. The volume model of SOEC. (A) SOEC on the coronal section; (B) SOEC on the sagittal section; (C) 3D model showing the reconstructed SOEC; (D) SOEC on the horizontal section. Positions of three grades of AEA (red arrow). (A) Grade I: the AEA is within the skull base; (B) II: the AEA protrudes from the skull base; (C) III: the AEA is below the skull base.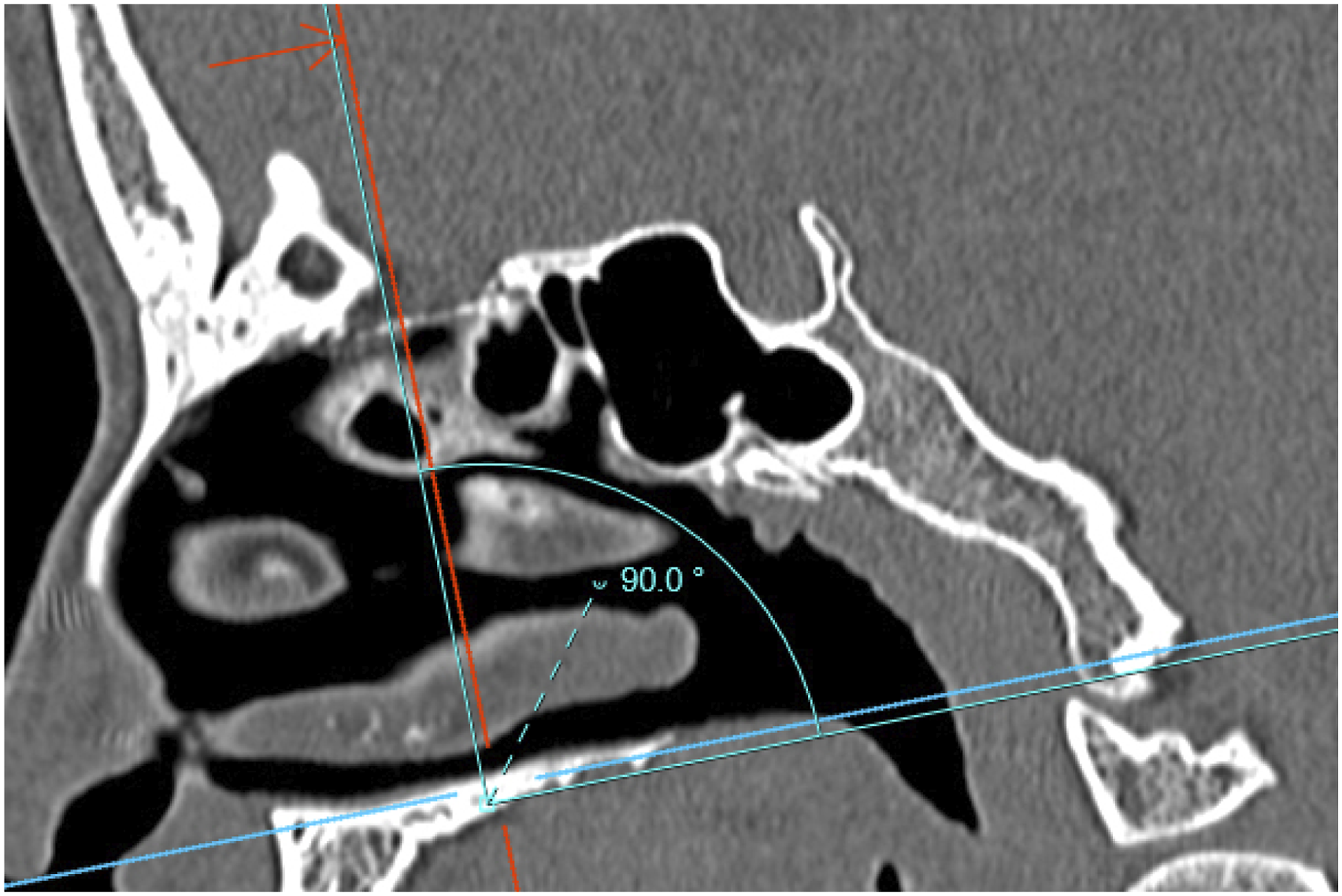
Statistical analysis
SPSS Statistics Premium v26.0 software was used for the statistical analyses. The data were described as M (P25, P75) for numerical variables while rate (%) for categorical variables. We included SOEC, LLCP, and sex data as predictive variables to obtain the odds ratio (OR) with 95% confidence interval. The intra-group correlation coefficient (ICC) was calculated using a two-way mixed-effects model to evaluate the consistency and reliability of the measurements of AEA distance, the height and TD of SOEC, and the depth of LLCP conducted by the first author and the attending physician.
Results
Analysis of SOEC and AEAs between the sexes.
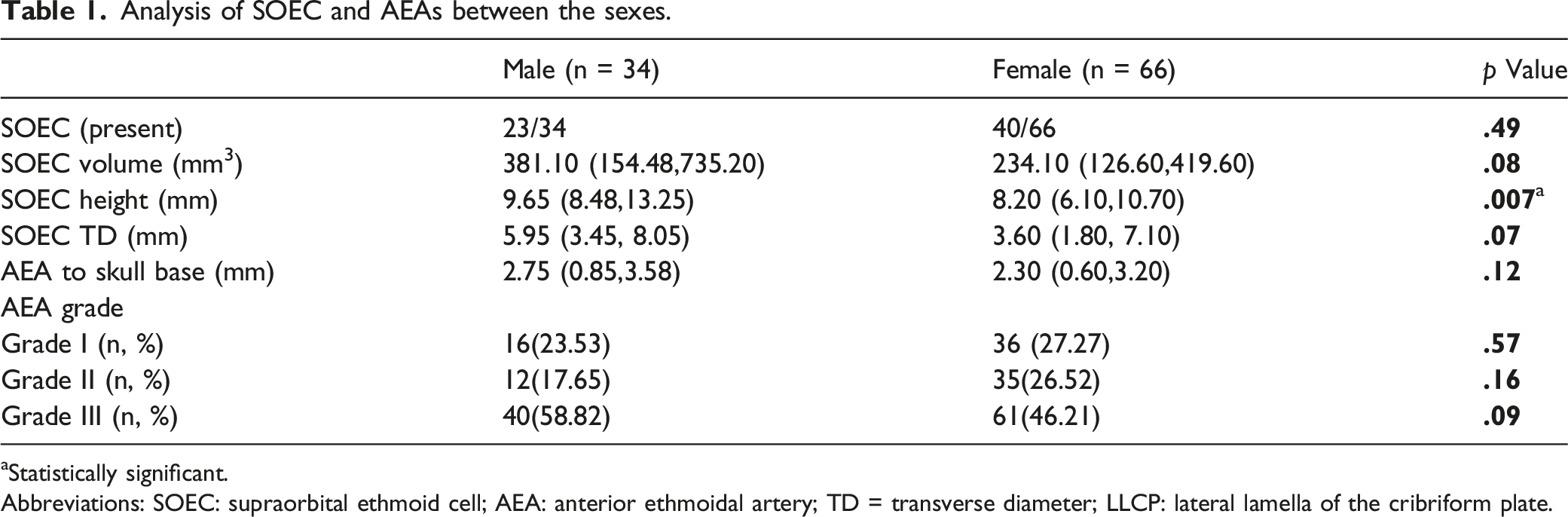
aStatistically significant.
Abbreviations: SOEC: supraorbital ethmoid cell; AEA: anterior ethmoidal artery; TD = transverse diameter; LLCP: lateral lamella of the cribriform plate.
Analysis of AEA and LLCP in patients with and without SOEC.
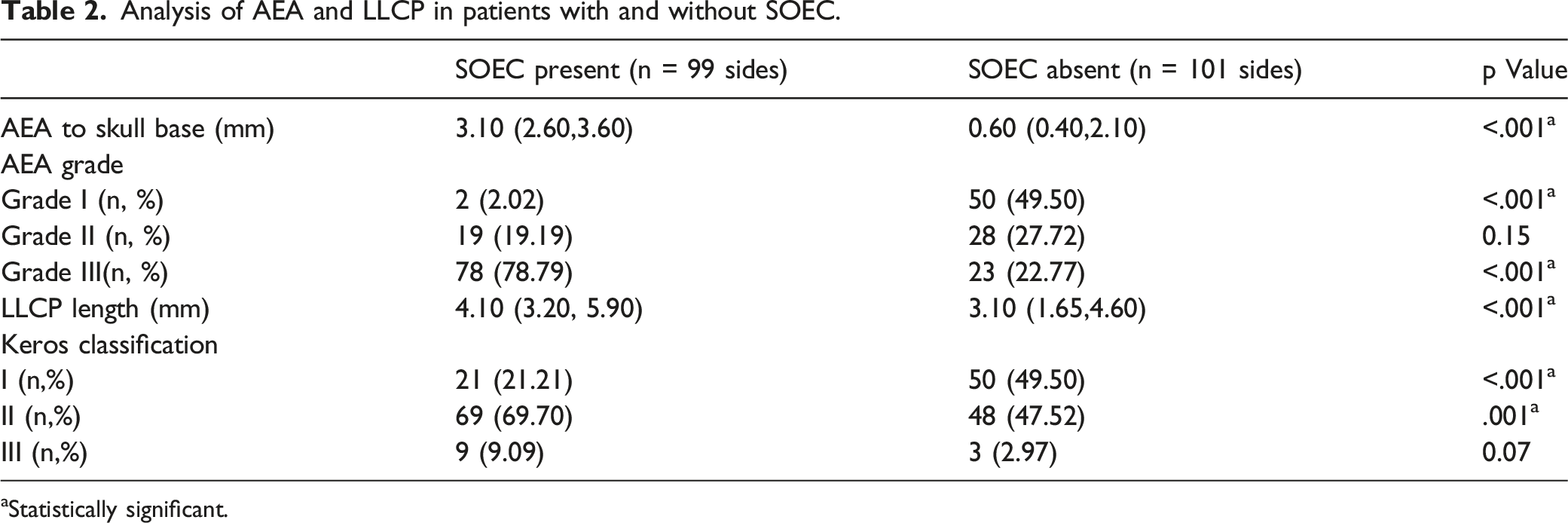
aStatistically significant.
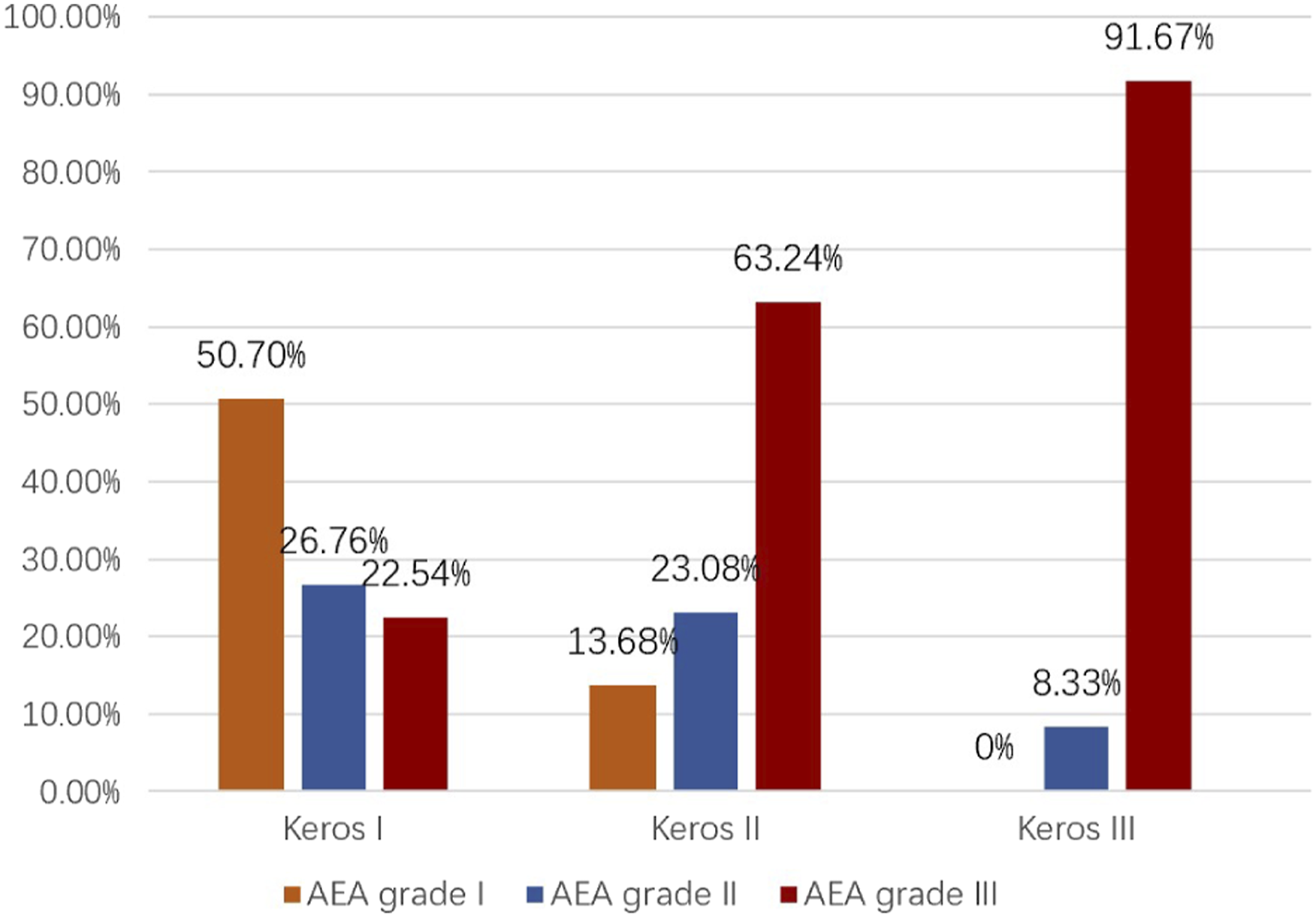
The incidence of AEA grades among Keros classifications. The incidence of AEA grade III among keros classification showed differences (P < .001).
Correlation between SOEC volume, height, TD, LLCP length, sex, and age, and AEA distance from the skull base.
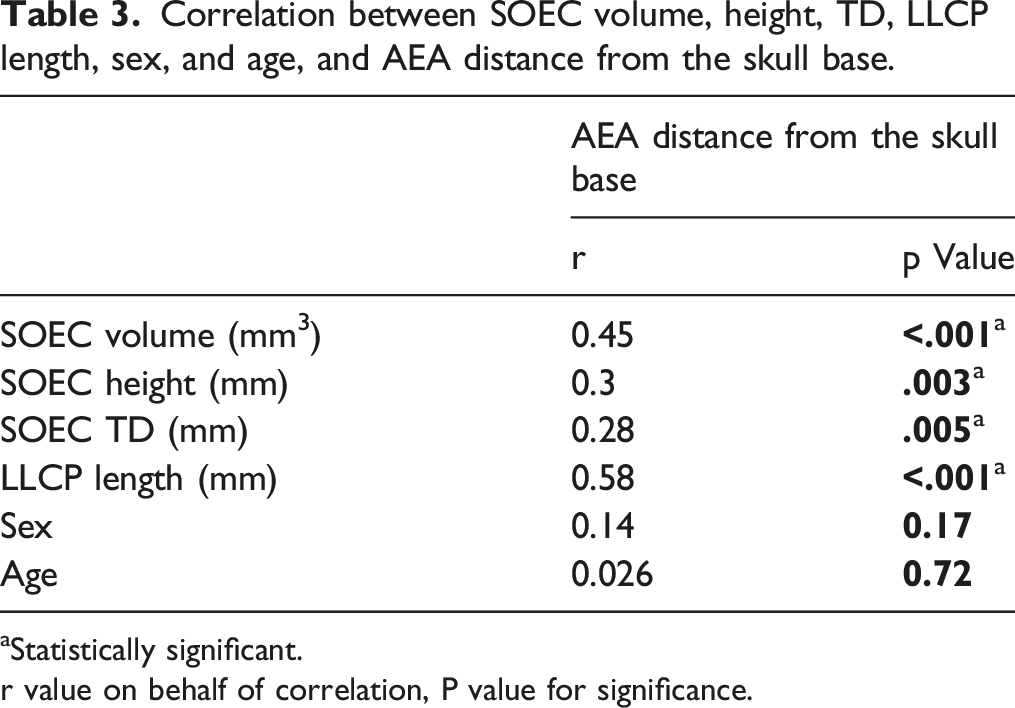
aStatistically significant.
r value on behalf of correlation, P value for significance.
Risk factors for the presence of AEA grade III.

aStatistically significant.
Discussion
The AEA is a significant anatomical structure of the anterior cranial fossa and plays an important role in endoscopic sinus surgery. Severe complications such as intraorbital hematoma and blindness may accompany AEA injury. 11 The injury increases with the increasing distance of the AEA from the skull base. Perry et al. 12 studied 101 CT scans and reported that the AEA below the skull base was in 25.7%. Mohamed et al. 4 showed that the prevalence of AEA suspension on the left was 62% and 48% on the right. The rate of the AEA below the skull base in this study was 50.5%. The rate of grade III AEA varies in different studies. These outcomes warn surgeons that the artery may be at a high risk during the endoscopic nasal surgery. Several methods have been studied to locate the AEA including the SOEC and keros classification.3,6 Mingsi Li et al.3 found that the presence of SOEC increased the distance from skull base (1.32 ± 1.5mm vs 0.47 ± 1.08mm). Adnan özdemir et al. 13 demonstrated that the higher the Keros grade is, the farther the AEA will be from the skull base. Either the presence of SOEC or a higher Keros grade increases the risk of injury to the AEA. The research of David W et al. 9 suggested that overexpanded SOEC on AEA distance from the skull base was farther than normal SOEC (6.57 ± 5.17 vs 1.32 ± 1.51mm). However, the influence of pneumatization parameters, such as SOEC height and volume, on the position of the AEA remains unknown. Therefore, we focused on the SOEC and studied the correlation of SOEC pneumatization and AEA position by measuring SOEC volume, height, and TD.
The occurrence rate of SOEC varies greatly across different studies and different races, ranging from 1.7% to 64.4%,9,14,15 which may be related to the different criteria applied and the number of patients included in different studies. SOEC was present in 63% of the patients in this study, which is higher than in previous research for Asians and close to the rate seen in Westerners. The reason included the difference in criteria of inclusion and exclusion and the slice thickness of CT scans. Joshi et al. 16 and Mohamed et al.4 showed that the presence of SOEC could significantly affect the distance between the AEA and the skull base. In our study, the distance of the AEA from the skull base in patients with SOEC was significantly greater than in those without SOEC (3.1 vs 0.6mm, P < .001), further confirming the above conclusion. We adopted the classification method of Lannoy et al. to refer to the AEA position relative to the skull base. 5 The AEA is suspended below the skull base in grade III, which is associated with the highest risk for injury during surgery. The rate of grade III AEA in our study was 50.5%; grade III AEA was the most common, consistent with the conclusion of Pan ZhY. 17 The incidence in our study was higher than that found by Abdullah et al. 18 and SHI Muhan. 19 The result may be caused by the high occurrence rate of SOEC in the patients included in our study. Sample size and ethnicity differences cannot be ruled out. We further found that the rate of grade III AEA in the SOEC group (78.79%) was significantly higher than that in the non-SOEC group (22.77%) (P < .001), consistent with the conclusion of SHI Muhan. 19 We compared the difference in LLCP length in those with or without SOEC. LLCP length was increased in those with SOEC (P < .001), and there were significant differences in Keros classification I(P < .001) and Keros classification II (P = .001) between the two groups. Thus, SOEC significantly affects LLCP length. Recent studies have indicated that Keros classification has a significant effect on the position of the AEA.3,20 Our study confirmed a significant difference in the incidence of type III AEA among Keros classification (P < .001), further confirming this result.
Different from previous studies, our research more comprehensively represented the pneumatization of SOEC by measuring two-dimensional height, TD parameters, and three-dimensional volume parameters and analyzed the pneumatization of SOEC between sexes. The results demonstrated that SOEC height was greater in males than females (P = .007). This finding is likely due to the larger head size and circumference universally found in males versus females.
In addition, we explored the correlation between SOEC volume, height, TD, LLCP height and sex, and the distance from the AEA to the skull base by Spearman's correlation analysis. SOEC volume, height, TD, and LLCP were prominently correlated with the distance from the AEA to the skull base; SOEC volume and LLCP were moderately correlated with the distance from the AEA to the skull base, while SOEC height and TD were weakly correlated. We hypothesized that SOEC volume, height, TD, and LLCP all could predict the position of the AEA relative to the skull base. We included SOEC and LLCP to construct a multivariate logistic regression analysis. The results showed that the SOEC presence(OR 10.814, 95%CI 5.274-22.175, P < .001) and the increased LLCP length(OR 1.583, 95%CI 1.294–1.936, P < .001) were independent risk factors for the AEA below the skull base. These results were unprecedented and provided a more comprehensive reference for locating the AEA.
However, there are limitations in our study. We couldn’t find proper standard to classify the SOEC like Keros classification. It is possible to type it according the pneumatization or the position of SOEC for further research. What’s more, patients with nasal sinus were excluded from our study, and the influence of SOEC pneumatization on drainage of frontal sinus wasn’t observed. We will further verify it in future study.
According to our results and those of previous studies, it can be inferred that in the case of SOEC, the greater the volume of the SOEC and the length of the LLCP are, the more cautious surgeons must be when evaluating the location of the AEA to prevent serious complications associated with arterial injuries, such as nosebleed, intraorbital hematoma, and blindness. 11
Conclusion
The results of this study suggest that up to 50.5% of the Chinese population may have grade III AEA. Therefore, identifying SOEC, evaluating SOEC pneumatization, and confirming the AEA location by CT scans before surgery is critical for preventing intraoperative arterial injury. Increased SOEC volume, height, and TD increase the distance of the AEA from the skull base. This study is an important reference for clinical surgeons performing nasal endoscopic surgery, promoting safety.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Nanjing Medical Science and Technique Development Foundation (YKK20070 to C.J.Y.); Nanjing Drum Tower Hospital Clinical College of Nanjing Medical University 2021 Educational Research Project (20210ZC078 to C.J.Y.).
Data available statement
The data that supports the findings of our study are available from the corresponding authors upon reasonable request by mail.