
Abstract
Objective
Our aim is to describe the location and course of the greater palatine canal (GPC) by analyzing its relationship with anatomical landmarks that can be used during endoscopic sinus surgery. This information might help prevent injury to the neurovascular bundle.
Methods
A retrospective evaluation of paranasal sinus CT scans of 100 consecutive random patients, 200 sides, was performed. Five measurements related to the course of the GPC were conducted, from cranial to caudal. The anatomical landmarks were the inferior bony border of the sphenopalatine foramen to the cranial entrance of the GPC, the distance from the most dorsal, and inferior bony insertion of the middle turbinate and the inferior turbinate bones to the anterior margin of the GPC. The angle between the horizontal palatine bone and the GPC, its length, and the prevalence of osteophytes in GPC was also assessed.
Results
The mean distance of the inferior border of the sphenopalatine foramen to the cranial entrance of the GPC was 9.39 ± 1.72 mm. The mean distance of the dorsal insertion of the middle turbinate to the anterior margin of the GPC was 3.89 ± 0.93 mm. The distance of the dorsal insertion of the inferior turbinate to the anterior margin of the GPC was 3.16 ± 0.81 mm. The mean angle between the horizontal palatine bone and the GPC was 114.33 ± 10.92º and the mean length of the GPC was 30.23 ± 3.74 mm. None of the measurements showed a significant difference between the two sides.
Conclusions
The landmarks used are easy to locate and assess on CT scans. These findings may help to make dissection safer in pathologies related to the pterygopalatine fossa, lateral sphenoid sinus or adjacent skull base.
Keywords
Introduction
Endoscopic surgery has many advantages in managing tumors and other pathologies around the pterygopalatine fossa or the lateral recess of the sphenoid sinus. Improved visualization by endoscopic access enables the surgeon to locate and more readily preserve the contents of the pterygopalatine fossa compared with traditional craniofacial procedures such as en bloc resection. 1 Surgery of this area requires detailed knowledge of its anatomy to avoid injury to the maxillary artery, the maxillary nerve, and the branch of the greater palatine nerve (GPN). 2
The pterygopalatine fossa has the shape of an inverted cone, with the greater palatine canal (GPC) leading to the greater palatine foramen. The GPC neurovascular bundle emerges from the canal in the posterolateral region of the hard palate, in the perpendicular plate of the palatine bone, supplying this region.3,4 The descending palatine artery arises from the third segment of the maxillary artery within the pterygopalatine fossa and it continues as greater palatine artery (GPA) and lesser palatine artery (LPA). 5 Together with the GPA and LPA, the GPN and the lesser palatine nerves (LPN) course within the GPC leading to the maxillary nerve (V2).6-8 The LPN leaves the GPC in the posterior direction via small lesser or accessory palatine canals. Furthermore, the GPC carries parasympathetic fibers from the nerve of the pterygoid canal (vidian nerve) in the floor of the sphenoid sinus.
Our aim is to describe the location and course of the GPC by analyzing its relationship with anatomical landmarks readily visible during endoscopic surgery of this area.
Materials and Methods
Patients
A retrospective evaluation of paranasal sinus CT scans was performed in 100 randomly selected patients, 200 sides with a provisional diagnosis of chronic rhinosinusitis without polyposis (CRSsNP). The CT-Scans had been conducted on a Medical Radiological Institute, on a Siemens Definition AS 128 multislice scanner (Siemens Medical Systems), as a spiral data set reconstructed with 0.63mm slice thickness in axial/coronal/sagittal planes. Patients with prior endonasal surgical procedures were excluded from the analysis.
The measurements were executed by an ENT surgeon and a neuroradiologist.
Patients’ informed consent was obtained. The study was conducted according to the Helsinki Declaration guidelines of good clinical practice.
Measurements
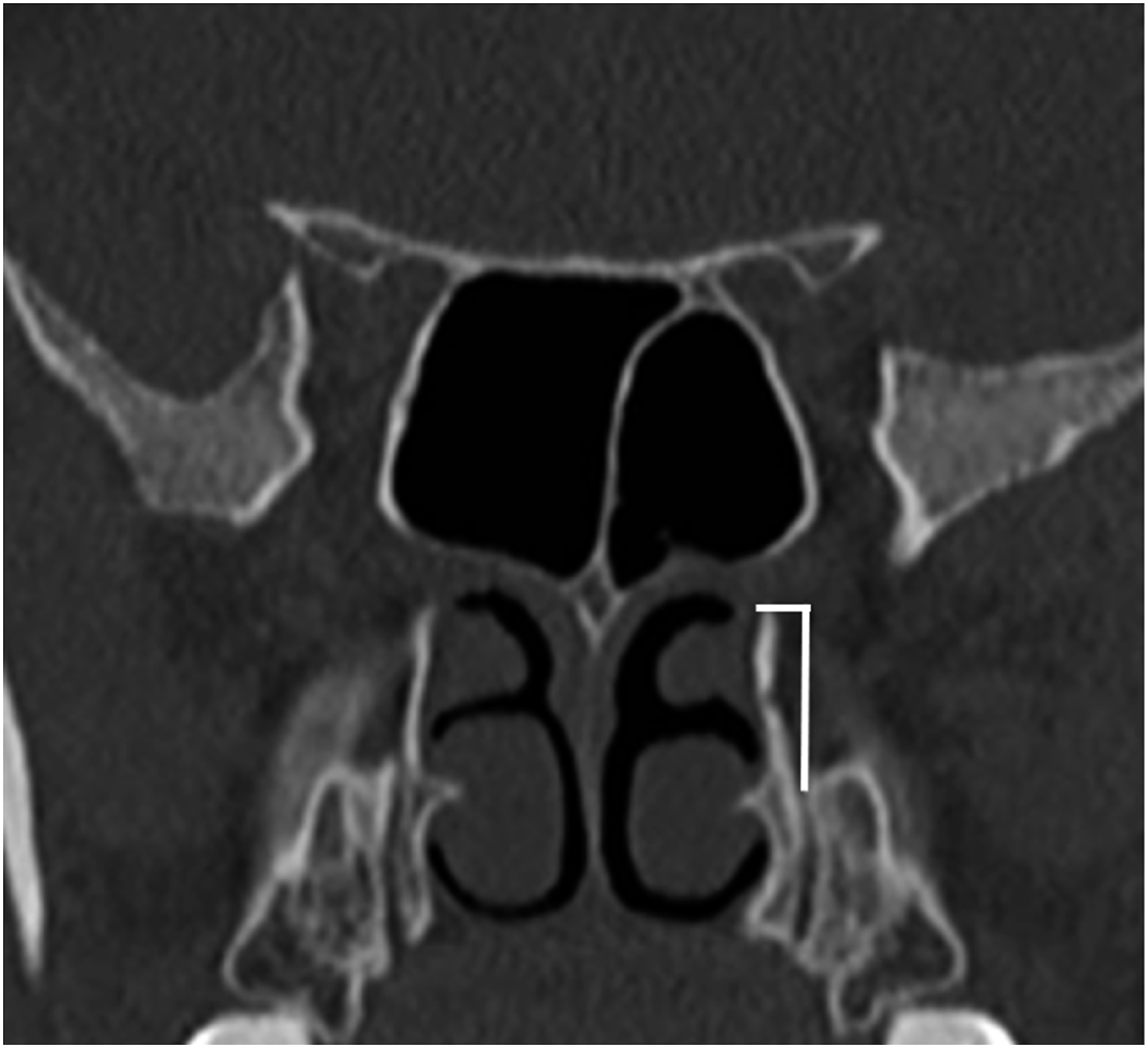
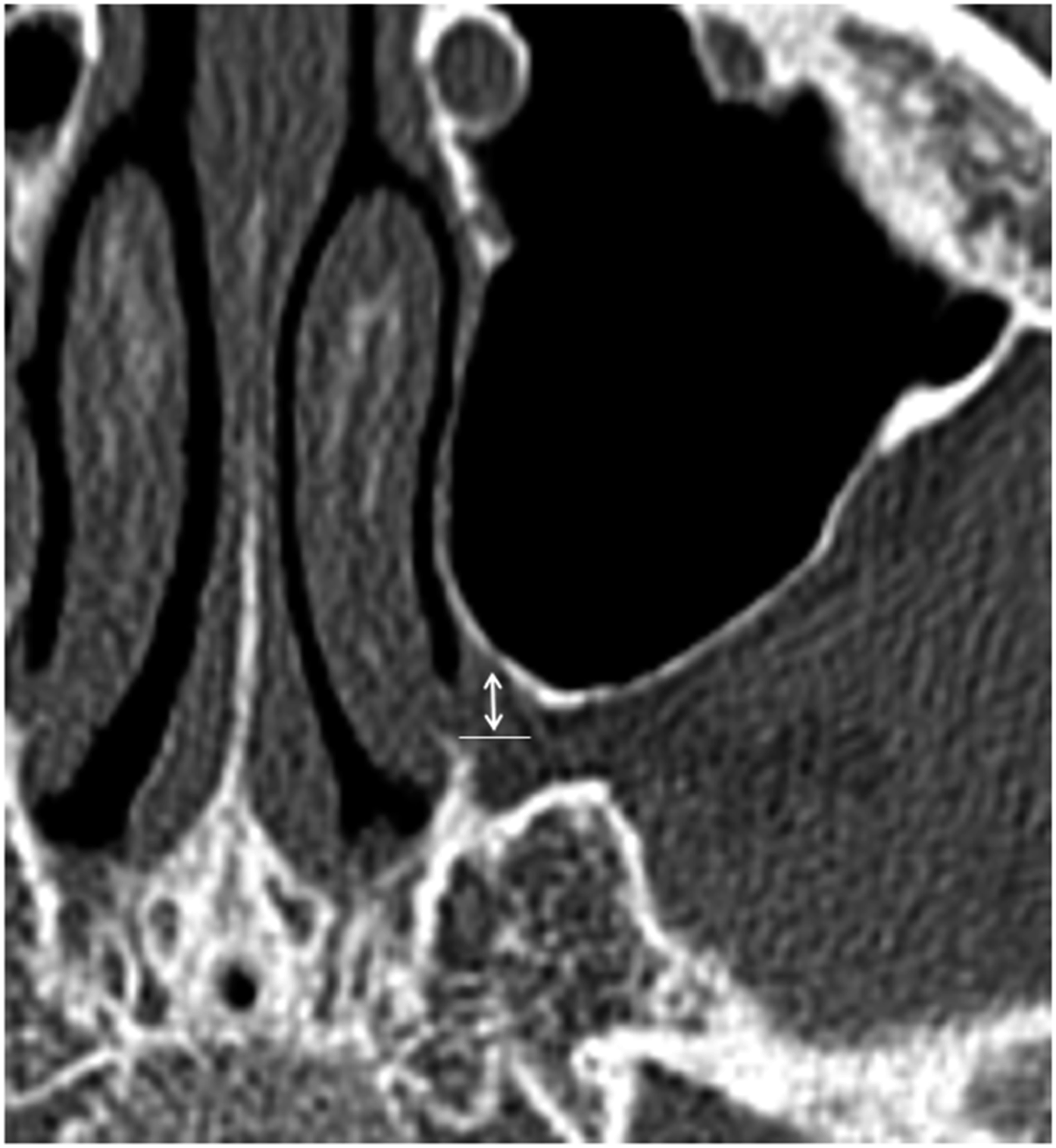
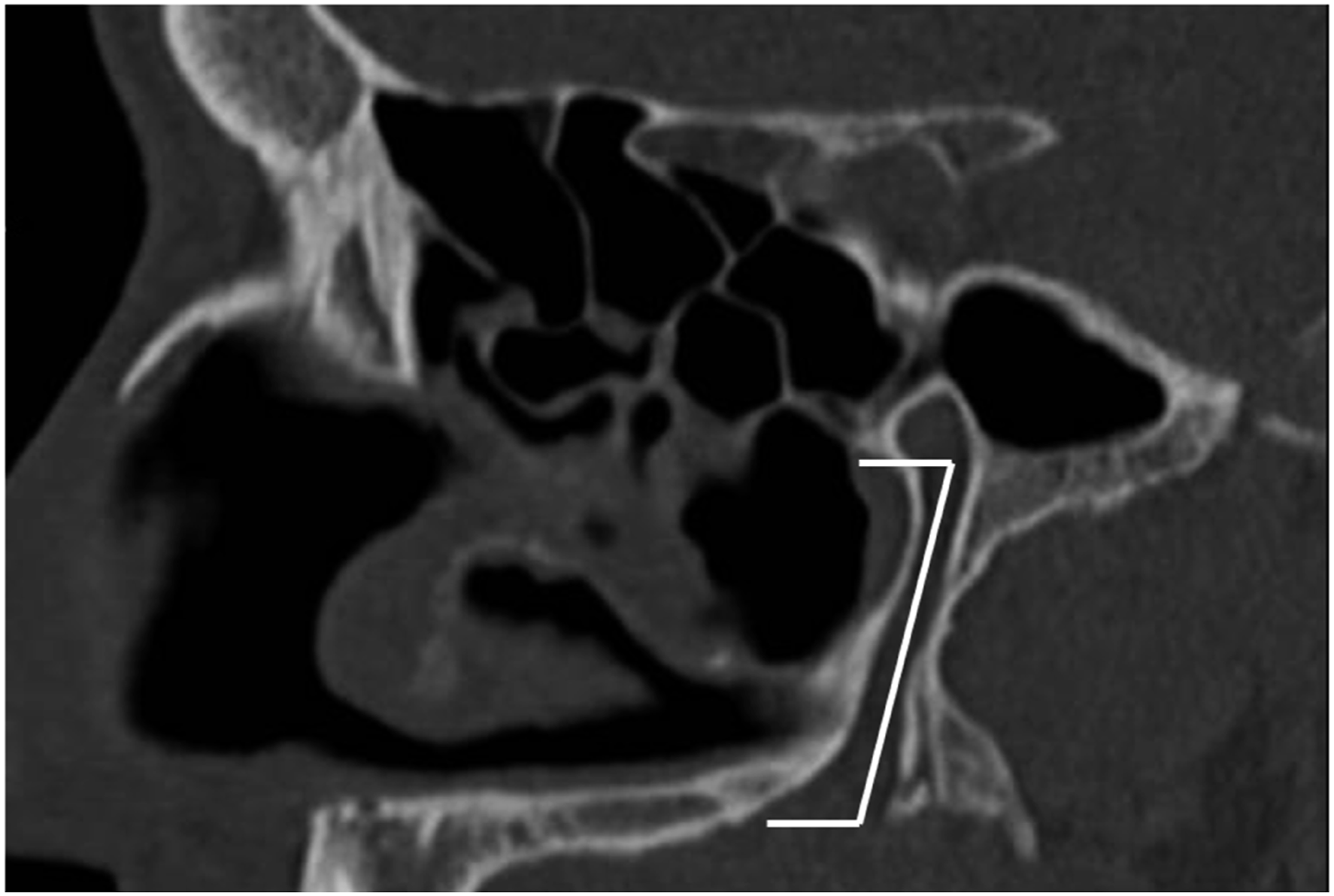
Five measurements targeted to the course of the GPC were conducted: 1. Coronal plane: distance from the inferior bony border of the sphenopalatine foramen to the cranial entrance of the GPC (Figure 1) 2. Axial plane: distance from the most dorsal and inferior bony insertion of the middle turbinate bone to the anterior margin of the GPC (Figure 2) 3. Axial plane: distance from the most dorsal and inferior bony insertion of the inferior turbinate bone to the anterior margin of the GPC (Figure 3) 4. Sagittal plane: angle between the horizontal palatine bone and the GPC (Figure 4) 5. Sagittal plane: length of the GPC from its entry point in the pterygopalatine fossa (measured at the level of the center of the pterygoid canal) to its exit point in the palatine foramen (Figure 5) Coronal plane: Distance from the inferior bony border of the sphenopalatine foramen to the entrance of the GPC, «Sphenopalatine foramen to GPC» - vertical white line. Axial plane: Distance from the most dorsal and inferior bony insertion of the middle turbinate bone to the anterior margin of the GPC, «Middle turbinate to GPC» - orange line. Axial plane: Distance from the most dorsal and inferior bony insertion of the inferior turbinate bone to the anterior margin of the GPC, «Inferior turbinate to GPC» - green line. Sagittal plane: Angle between the horizontal palatine bone and the GPC, «Angle hard palate - GPC» - White angle. Sagittal plane: Length of the GPC from its entrance in the pterygopalatine fossa to its exit point at the lower point through the greater palatine foramen, «Length of GPC» - vertical white line.


The prevalence of osteophytes in the GPC was also assessed.
Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Science (SPSS) (v:27). The Shapiro-Wilk test was used to see whether the results were distributed normally. For normally distributed values, descriptive results are expressed as mean ± SD. The Independent t-test/Mann Whitney test was used to compare continuous variables between two groups. A Pearson correlation coefficient/Kendall’s tab analysis was used to examine the relationship of two related variables. A chi-squared test was used for comparison between two attributes. The distribution of the samples was assessed by histogram and plot visual analysis, and based on this, a non-parametric test, the Mann-Whitney, was used to compare the two sides. A two-sided P-value < .05 was considered statistically significant.
Results
Our study series consisted of 56 women and 44 men, aged between 18 and 80 years (mean 42.03 ± 13.99 years).
Measurements obtained in the series, being Sphenopalatine foramen to GPC – measurement 1, middle turbinate to GPC – measurement 2, inferior turbinate to GPC – measurement 3, angle hard palate - GPC – measurement 4, and Length of the GPC – measurement 5.
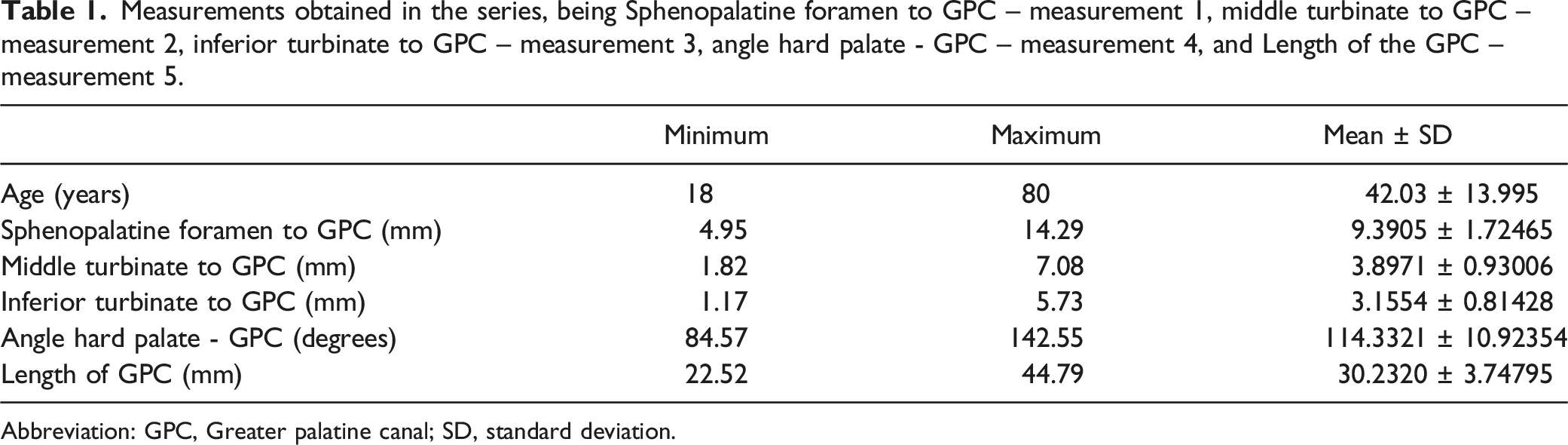
Abbreviation: GPC, Greater palatine canal; SD, standard deviation.
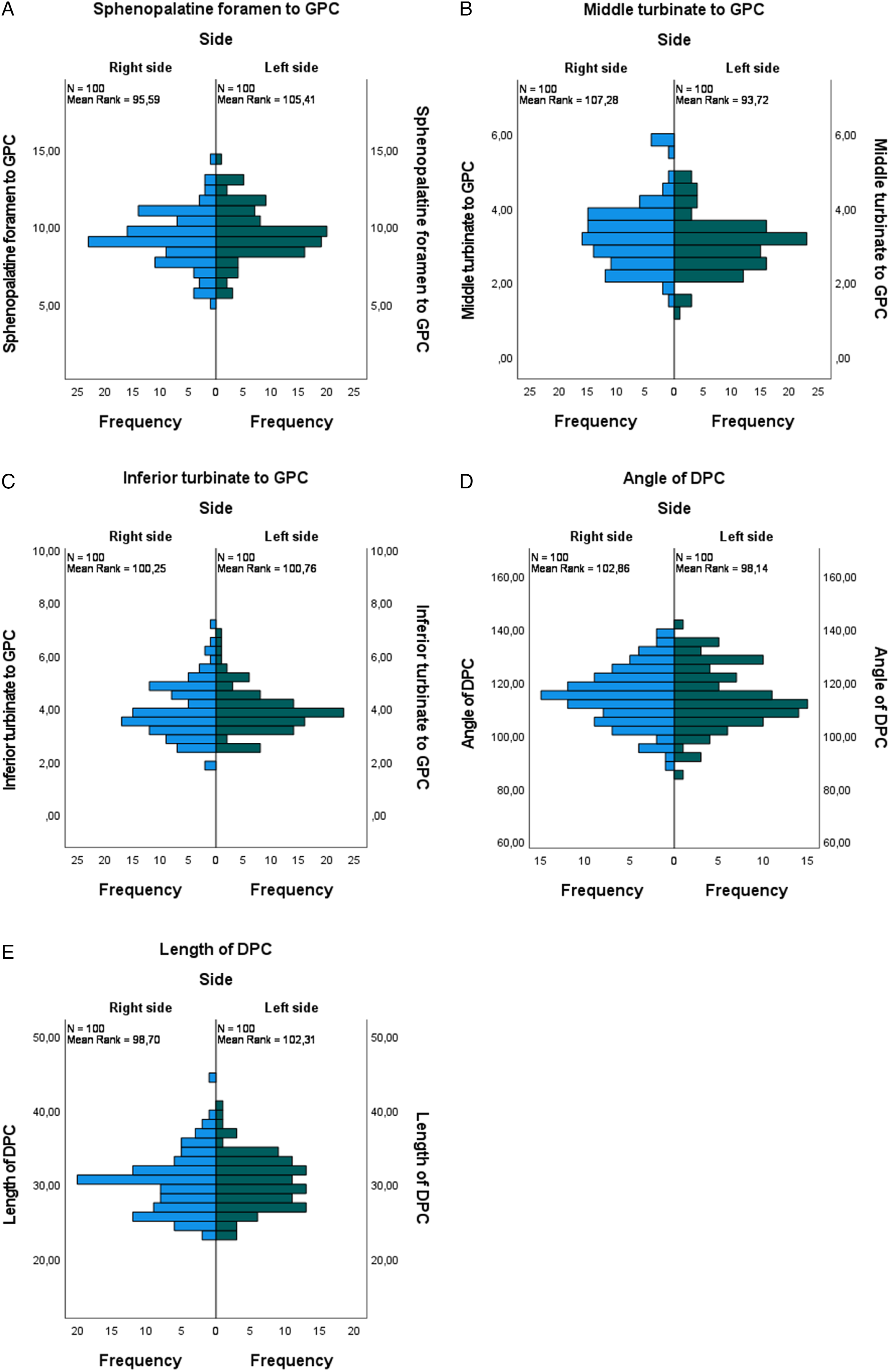
(A) Mann-Whitney test results presented in the plot. We compared the distance from the sphenopalatine foramen to GPC between sides – with no difference between sides. p = NS. GPC – greater palatine canal. (B) Mann-Whitney test results of the distance between the posterior insertion of the middle turbinate and the anterior circumference of the GPC, presented in the plot. There was no significant difference between the sides. p = NS. GPC – greater palatine canal. (C) Mann-Whitney test results presented in the plot. We compared the distances from the inferior turbinate to GPC between sides, with no difference between them. p = NS. GPC – greater palatine canal. (D) Mann-Whitney test results presented in the plot. We compared the angle of GPC on right and left sides, with no difference between them. p = NS. GPC – greater palatine canal. (E) Mann-Whitney test results presented in the plot. We compared the length of the GPC between sides with no difference between them. p = NS. GPC – greater palatine canal.
The mean distance from the dorsal insertion of the middle turbinate to the anterior margin of the GPC (distance 2), was 3.89 ± 0.93 mm (minimum 1.82 mm, maximum 7.08 mm), with there being no statistical difference between the two sides (P > .05; 0.950) (Table 1, Figures 2, 6B).
The distance between the dorsal insertion of the inferior turbinate and the anterior margin of the GPC (distance 3) was 3.16 ± 0.81 mm (minimum 1.17 mm, maximum 5.73 mm). There was no significant difference between the two sides (P > .05; 0.622). (Table 1, Figures 3, 6C).
The angle between the horizontal palatine bone and the GPC (measurement 4) was 114.33 ± 10.92º (minimum 84.57º, maximum 142.55º). There was no significant difference between the two sides (P > .05; 0.564). (Table 1, Figures 4, 6D)
The length of the GPC was 30.23 ± 3.74 mm (minimum 22.52 mm, maximum 44.79 mm). As in the previous measurements, there was no significant difference between the two sides (P > .05; 0.659). (Table 1, Figures 5, 6E).
We also compared the distances between gender, with no statistical difference between distances 1-5 (P > .05).
The prevalence of osteophytes found in the great palatine canal was 17%.
Discussion
Endoscopic surgery of the pterygopalatine fossa entails risk to its vascular and neural contents. This is especially true for the GPN and the LPN crossing the pterygopalatine fossa from the round foramen (lateral) to the GPC (medial and inferior). Injury of the GPC and the GPA can result in significant blood loss, and whilst this can be controlled during surgery it can occasionally cause a pseudoaneurysm. 9 Postoperative hypesthesia of the gingivae and ipsilateral hard palate may be a sequela of an injury to the GPN and LPN.9,10 The structures of the GPC may be exposed during the radiofrequency of the inferior turbinates or when performing monopolar coagulation of branches of the sphenopalatine artery.11,12 The prevalence of injury to the GPN following endoscopic sinus surgery has not been reported.
Understanding the anatomy of the GPC is also important when a nerve block is required. This has been shown to reduce pain scores following sinus surgery and improve the surgical field due to less bleeding.13-17 It is worth mentioning that GPN can be assessed by endonasal route or transoral route to achieve anesthesia of maxillary nerve in the pterygopalatine fossa, playing a role in regional anesthesia for nasal surgery. 18
The artery and especially the nerves are usually not visible on the CT scan and intraoperative identification of these structures in the pterygopalatine fossa is difficult. A reliable landmark to locate these structures is the GPC. Intraoperative navigation helps to localize the bony anatomy of the pterygopalatine fossa and the GPC. However, additional intraoperative landmarks are needed for a precise and safe dissection. 19
The anatomy of the GPC has been broadly documented in the literature for maxillo-facial surgeons. Rapado-González et al., described the shape of the great palatine foramina and the GPC using a horizontal line drawn on the lower third of the GPC and seeking where it intersects the sagittal plane, and the great palatine foramina shape was simultaneously done in the axial plane.20,21
Mellema et al. in 2004, described a position of the GPN as anterior and inferior in relation to greater palatine foramen but only 11 pterygomaxillary fossae were assessed. 22 Campbell et al. endoscopically studied the GPC and described different landmarks and their relations to the GPC such as the nasolacrimal duct, the posterior edge of the hard palate, and the posterior wall of the maxillary sinus. It emphasized the importance of surgical landmarks when approaching the pterygopalatine fossa, especially when this area was distorted by tumors or destructive lesions. 9
The first three landmarks presented in this paper are chosen because of their proximity to the GPC, so they can be identified intraoperatively. The angle of the GPC in relation to the hard palate and the length of the canal help to predict its anatomical course.
The first landmark is the vertical distance in the coronal plane from the inferior border of the sphenopalatine foramen to the entrance of the GPC. This landmark can be used to localize the entrance of the GPC and its neurovascular bundle by dissecting from the sphenopalatine foramen inferiorly in the vertical plane. In practical terms, one must first identify the ethmoidal crest, then the sphenopalatine foramen and the branches of the sphenopalatine artery. The GPC can be found inferiorly from the sphenopalatine foramen down to the insertion of the inferior turbinate lateral into the bone.
The second landmark, measured in the axial plane of the CT, is the distance from the most dorsal and inferior bony insertion of the middle turbinate bone to the anterior margin of the circumference of the GPC. This had a mean distance of 3.89 ± 0.93 mm. This indicates their proximity and the care need to avoid injury. If the middle turbinate is resected, the GPC can be compromised by a fracture at the posterior portion of the inferior turbinate overlying the canal. 23
The third landmark, also assessed on the axial CT, is the distance from the most dorsal point of the bony insertion of the inferior turbinate and the anterior circumference of the GPC. We found a mean distance of 3.16 ± 0.81 mm. Also, along with the second landmark, this short distance reminds the endoscopic surgeon to be careful when dissecting this area. In the case of unaltered anatomy of the inferior turbinate, this landmark can act as a guide to delineate the dissection in direction of the GPC.
In summary, these measurements allow us to underline the proximity of the dorsal attachment of the middle and inferior turbinates to the bony canal of GPC, as previously described in the literature.9,17,19
Knowledge of the angle between the hard palate and the GPC of 114,33 ± 10.92º and the length of the canal of 30.23 ± 3.74 mm helps to work out the anatomy of the GPC. There are numerous studies that assessed the length of the GPC, such as those published by Douglas et al. and Aoun et al. with values between 18 mm 10 and 30 mm. 24 The large range may be explained by the fact that the superior “entrance point” to the GPC is difficult to assess and various studies have used different ways of doing this.
The study of Campbell et al. 9 uses different landmarks, not distant to the GPC such as from the anteroinferior aspect of the GPC to the anteroinferior aspect of the orifice of the nasolacrimal duct. This distance and the distance from the anteroinferior aspect of the GPC to the posterolateral free edge of the hard palate are hard to assess endoscopically. 25
The presence of an osteophyte in the GPC can lead to compression of the neurovascular structures. There are few studies that addressed this issue, although it is worth to mention a prevalence of 35.3% in Indian skulls and 24.6% in Nigerian skulls. 26 Despite using a different method of data acquisition, our results resemble the findings of Westmoreland who described a bony projection in 16% of the skulls. 27
The landmarks presented in this study are chosen to support the endoscopic surgeon operating in the pterygopalatine fossa and the surrounding bony structures containing the GPC. From cranial to caudal, the sphenopalatine foramen and the dorsal insertions of the middle and inferior turbinate can easily be found. Even in cases where the anatomy is distorted, for example in cases of small juvenile angiofibroma, these landmarks can be assessed on the preoperative CT and be of help during surgery in the area of the pterygopalatine fossa.
In addition to well-established landmarks in the literature, those presented in this study are easy to assess and may contribute to safer dissection of the pterygopalatine fossa.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.