
Abstract
Cemento-ossifying fibroma (COF) is a rare fibro-osseous tumor. The lesion is most commonly seen in people in the third and fourth decade. There are three variants of ossifying fibroma; juvenile trabecular ossifying fibroma, juvenile psammomatoid ossifying fibroma, and COF. COF is highly cellular and contains a fibrous tissue that has different amounts of calcified tissue. Although histologically benign, it has a significant growth potential.
Keywords
Significance Statement
Cemento-ossifying fibroma (COF) is a rare fibro-osseous tumor. The lesion is most commonly seen in people in the third and fourth decade. There are three variants of ossifying fibroma; juvenile trabecular ossifying fibroma, juvenile psammomatoid ossifying fibroma, and COF. COF is highly cellular and contains a fibrous tissue that has different amounts of calcified tissue. Although histologically benign, it has a significant growth potential.
Introduction
Cemento-ossifying fibroma (COF) is a rare fibro-osseous tumor that usually involves maxilla, mandible, and other bones of the face and head including the ethmoid sinuses and nasal cavity, but the mandible is the most common location. The lesions are mostly solitary. It is most commonly seen in people in the third and fourth decade and is five times more common in females than in males.1,2
There are three variants of ossifying fibroma; juvenile trabecular ossifying fibroma, juvenile psammomatoid ossifying fibroma, and COF, the last of which is usually termed shortly as “ossifying fibroma.” 1 It is claimed that COF originates from multipotent cells of the periodontal membrane that have a potential of differentiating to bone, cementum, and fibrous tissue. COF is highly cellular and contains a fibrous tissue that has different amounts of calcified tissue which appears like bone, cementum, or both. 3
Small lesions are usually asymptomatic. Although histologically benign, it has a significant growth potential. 1 COF may enlarge and eventually present as a facial swelling and a sometimes as a gross facial deformity. 1
Due to its similar clinical and histological features, differential diagnosis from other fibro-osseous lesions like fibrous dysplasia becomes difficult. 2 COF must be surgically removed and an incomplete removal may lead to recurrence. 4
Here, a case of giant COF with cerebral involvement was presented and discussed because of its seldom occurrence and important characteristic radiological features that help in the correct diagnosis.
Case Presentation
A 12-year-old girl patient was admitted to our hospital with the complaints of headache, nasal congestion, and left facial asymmetry that had progressed slowly for eight months. In the ophthalmologic examination, a significant left exophthalmos was observed, while her vision and fundus examination were normal. Her left eye movements were limited medially. On the nasal examination, there was a mass, which had a semisolid consistency and a dirty pale color, that completely obliterated the left nasal cavity and caused a slight deviation of the septum to the right.
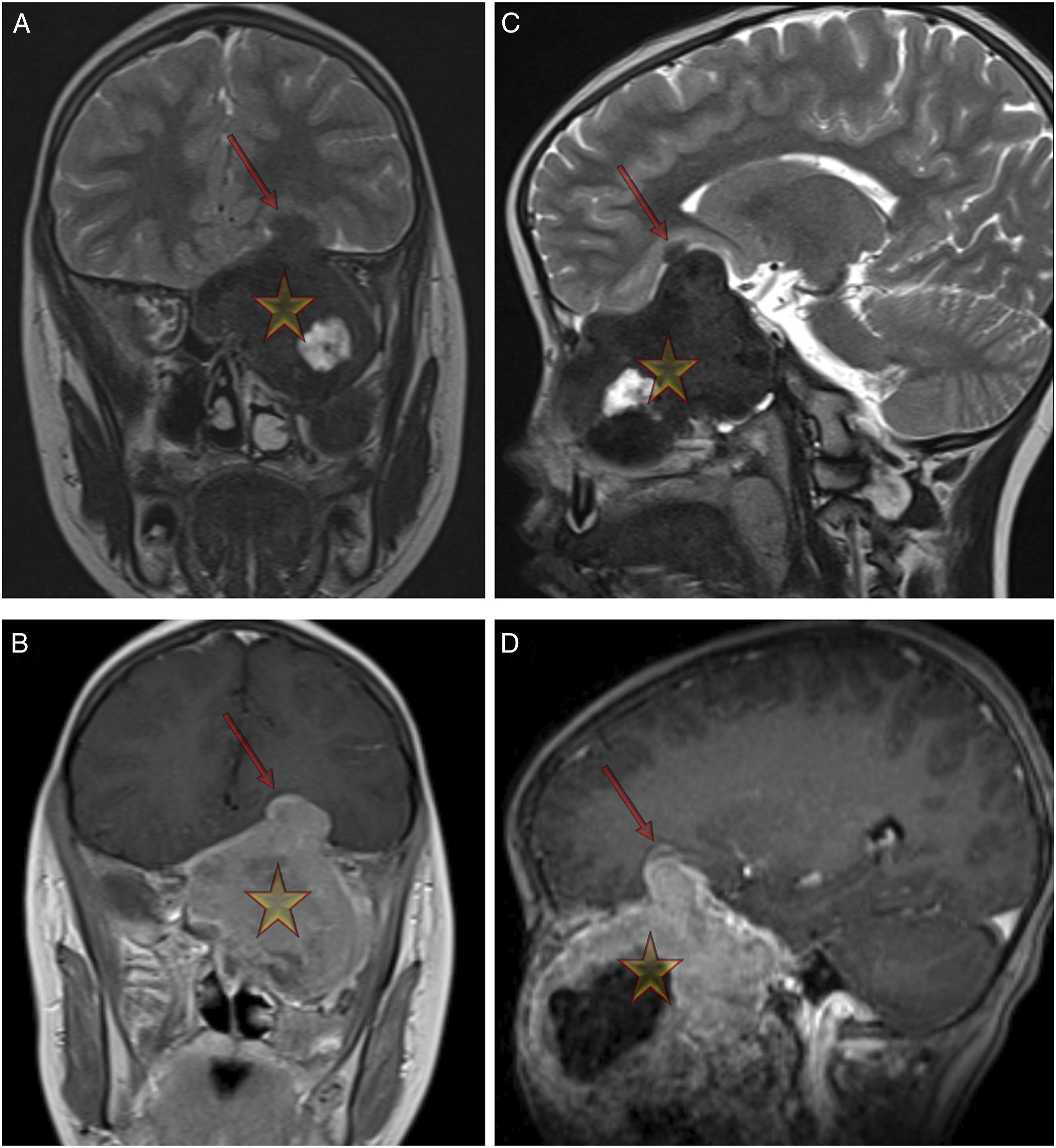
Computed tomography (CT) scan demonstrated an intensely sclerotic lesion with central hypodensity in the left sinonasal cavity (Figure 1A and B). In magnetic resonance (MR) imaging examination (Figure 2), a prominent cystic mass of a dimension of 7 × 8 cm was observed which had a smooth lobulated contour and extended to the maxillary sinus, ethmoid cells, and sphenoid sinus on the left. It was obliterating the left nasal cavity pushing the nasal septum to the right. It was extending to the left orbit, the middle, and anterior cranial fossae and was displacing the pituitary gland posteriorly (Figure 2A-D). An incomplete surgical resection was performed; histopathological diagnosis was reported as COF. Axial (A) and coronal (B) CT scans reveal an intensely sclerotic lesion (yellow stars) with central hypodensity in the left sinonasal cavity. Coronal (A) and sagittal (C) T2-weighted and post-contrast coronal (B) and sagittal (D) T1-weighted MR images show a giant hypointense neoplasm (yellow stars) with a moderate contrast enhancement without central contrast enhancement. The lesion also has trans-skull base extra-axial involvement (arrows).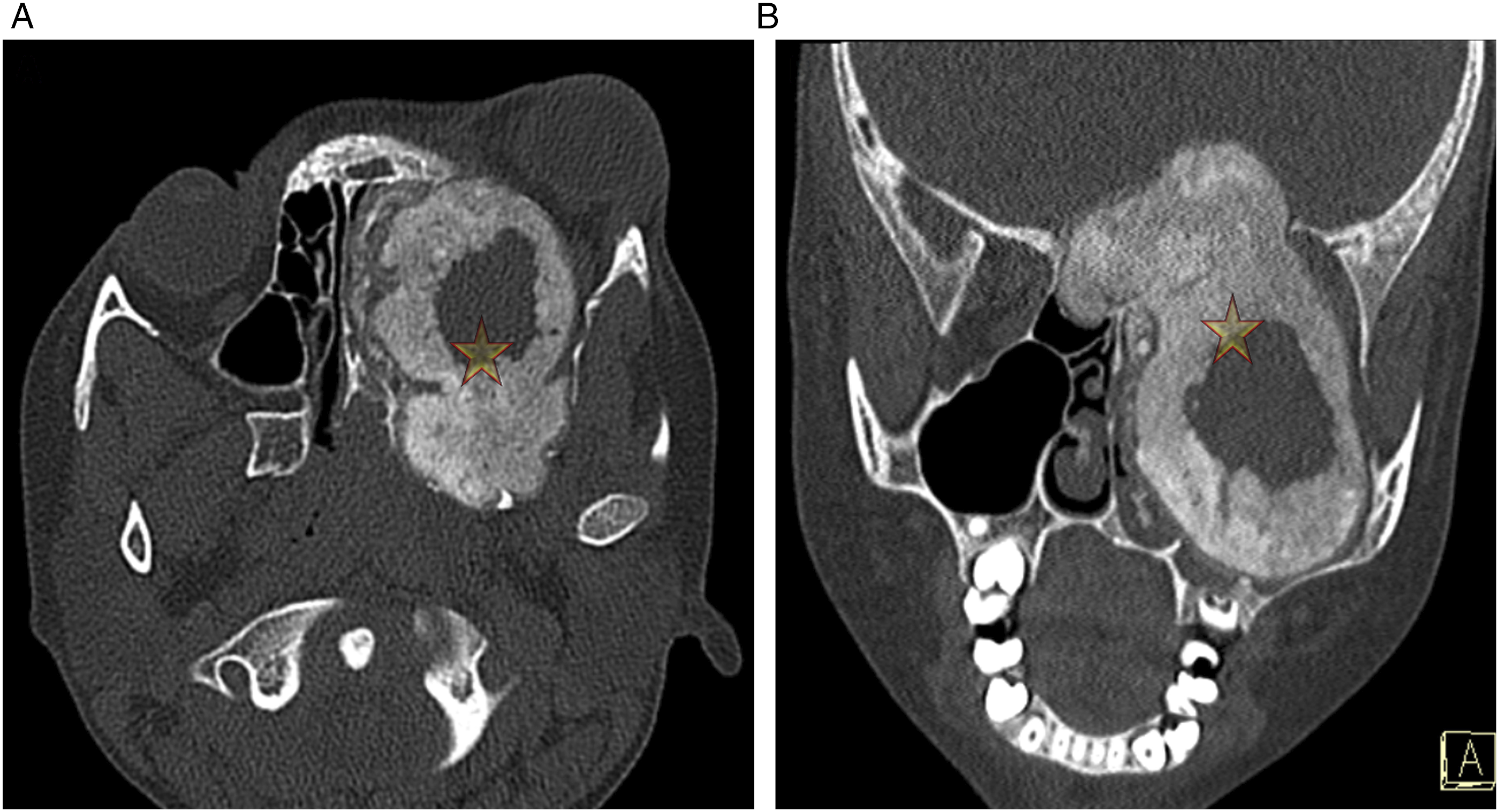
Conclusion
Although the majority of COF cases are encountered in the mandible and maxilla, other craniofacial locations have been reported. 5 In the present case, COF was involving the maxilla and was also extending to the left orbit and even anterior and middle cranial fossae, causing therefore headache, diplopia, and exophthalmos.
In radiological investigations, COF displays different image patterns depending on the content of the mineralized tissue. Different from fibrous dysplasia, it can clearly be distinguished from the surrounding bony structures. Early tumors appear radiolucent and with time bone densities develop and eventually the lesion becomes a radiopaque lesion with a typical halo formed by a less dense tissue. 5
COF is a rare benign tumor, which is usually asymptomatic in early stages, but it may reach great dimensions leading to destruction of surrounding structures and gross facial deformities causing associated sign and symptoms, especially in the juvenile form. Radiologic features are characteristic and are very helpful in the correct differential diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.