
Abstract
Cemento-ossifying fibromas (COFs) are benign fibro-osseous tumors usually found in the mandible and maxilla that can show malignancy in rare situations. COFs usually grow slowly and asymptomatically until they produce local bulges, pain, headaches, and visual impairment, and have a Ki-67 index within 3%, even in aggressive and recurrent cases. Surgical resection can usually provide a satisfactory prognosis. However, no cases of COF transforming into osteosarcoma have been reported. We present a case of COF involving a 58-year-old woman whose initial symptom was hearing loss in the right ear accompanied by tinnitus. Enhanced magnetic resonance imaging revealed a 3.1 cm x 3.2 cm mass centered on the right pterygoid process of the sphenoid bone. Postoperative pathology revealed a COF with a high Ki-67 index (8%–10%). Over the next two years, the tumor relapsed repeatedly. The patient underwent nine endoscopic surgeries and radiotherapy. The sixth postoperative biopsy showed that the COF had transformed into an osteosarcoma. The patient subsequently experienced respiratory and cardiac arrests and was receiving treatment in the intensive care unit with a poor prognosis at the time of writing this manuscript. Thus, a high Ki-67 index may be a risk factor for malignant transformation for COFs.
Introduction
According to the 4th edition of the World Health Organization’s Classification of Head and Neck Tumors published in January 2017, ossifying fibromas are categorized under odontogenic tumors. 1 Ossifying fibromas are histopathologically subcategorized into conventional ossifying fibroma, also called cemento-ossifying fibroma (COF), and two distinctive juvenile ossifying fibromas, namely, juvenile psammomatoid ossifying fibroma and juvenile trabecular ossifying fibroma, which are commonly seen in younger patients.1,2 COF has a lower recurrence rate of 8% and 20%, in comparison with the 30% recurrence rate of juvenile ossifying fibroma.2,3 COF is a benign fibro-osseous tumor that is usually found in the mandible and maxilla. Although COFs may develop malignancy in rare situations, cases of malignant transformation have not been reported. 4 In most cases, surgical resection can provide a satisfactory prognosis for the patient.
Case Presentation
A 58-year-old woman who had been experiencing hearing loss in the right ear for two months visited our otolaryngology outpatient department. Nasal endoscopy revealed bulging of the right torus tubarius and pharyngeal recess in comparison with the left side. Computed tomography (CT) revealed a mass of soft-tissue density in the right nasopharynx with bone destruction of the right pterygoid process and the posterior wall of the maxillary sinus and middle cranial fossa (Figures 1A and 1B). An enhanced magnetic resonance imaging (MRI) examination showed a 3.1 cm × 3.2 cm marginal enhancement mass centered around the right pterygoid process and involving the cavernous sinus and Eustachian tube (Figures 1C and 1D). The mass was considered to be of osteogenic or fibrous tissue origin on MRI and CT. The patient was then admitted to the hospital for surgical treatment. The intraoperative frozen section revealed spindle-cell hyperplasia and a small amount of ossification in the tissue. Complete excision was performed during the first surgery. Subsequent immunohistochemical findings supported a diagnosis of aggressive COF, indicating a benign but aggressive tumor. Six months later, the patient's eyesight started to decrease with epistaxis. CT and MRI revealed a 3.0 cm x 2.6 cm x 2.1 cm mass recurring in the operative area and invading the right orbit apex. Relapse of COF was confirmed by postoperative biopsy. The eyesight of the patient improved three days after endoscopic surgery. Considering the higher growth velocity and shorter interval between relapses in comparison with conventional COF, intensity-modulated radiotherapy was recommended with a total dose of 50.4 Gy in daily fractions of 1.8 Gy. Within 7 months after radiotherapy, the patient was admitted to our department with weakness in eyesight and diplopia. A third surgery was performed to prevent more severe complications from progressing. Over the next two years, the tumor relapsed repeatedly, forcing the patient to undergo nine surgeries in total. The latest MRI and CT scans (Figures 1E and 1F) showed that the tumor had relapsed again, and the lesion could not be excised by surgery. The sixth postoperative histopathological examination confirmed that the COF had transformed into an osteosarcoma. Immunohistochemical examination revealed positive results for Ki-67, special AT-rich sequence-binding protein 2 (STATB2), and smooth muscle actin (SMA). Written informed consent was obtained from the patient for the publication of this clinical record. The clinical and surgical principles adopted for her management complied with the ethical standards of the relevant national and institutional guidelines on human experimentation as laid down in the Declaration of Helsinki, 1975, and revised in 2008. (A and B), Preoperative high-resolution computed tomography (HRCT) scans of axial sections of the right sphenoid bone. The scans show a soft-tissue density lesion destroying the right pterygoid process, the posterior wall of the maxillary sinus, and the middle cranial fossa. (C and D), Preoperative axial and sagittal brain magnetic resonance imaging (MRI) sections. A 3.1 x 3.2 cm marginal enhancement mass centered around the right pterygoid process and involving the cavernous sinus and Eustachian tube T1 (C) and T2 (D). (E and F), Postoperative brain CT and MRI. The posterior cranial fossa was destroyed with intracranial extension.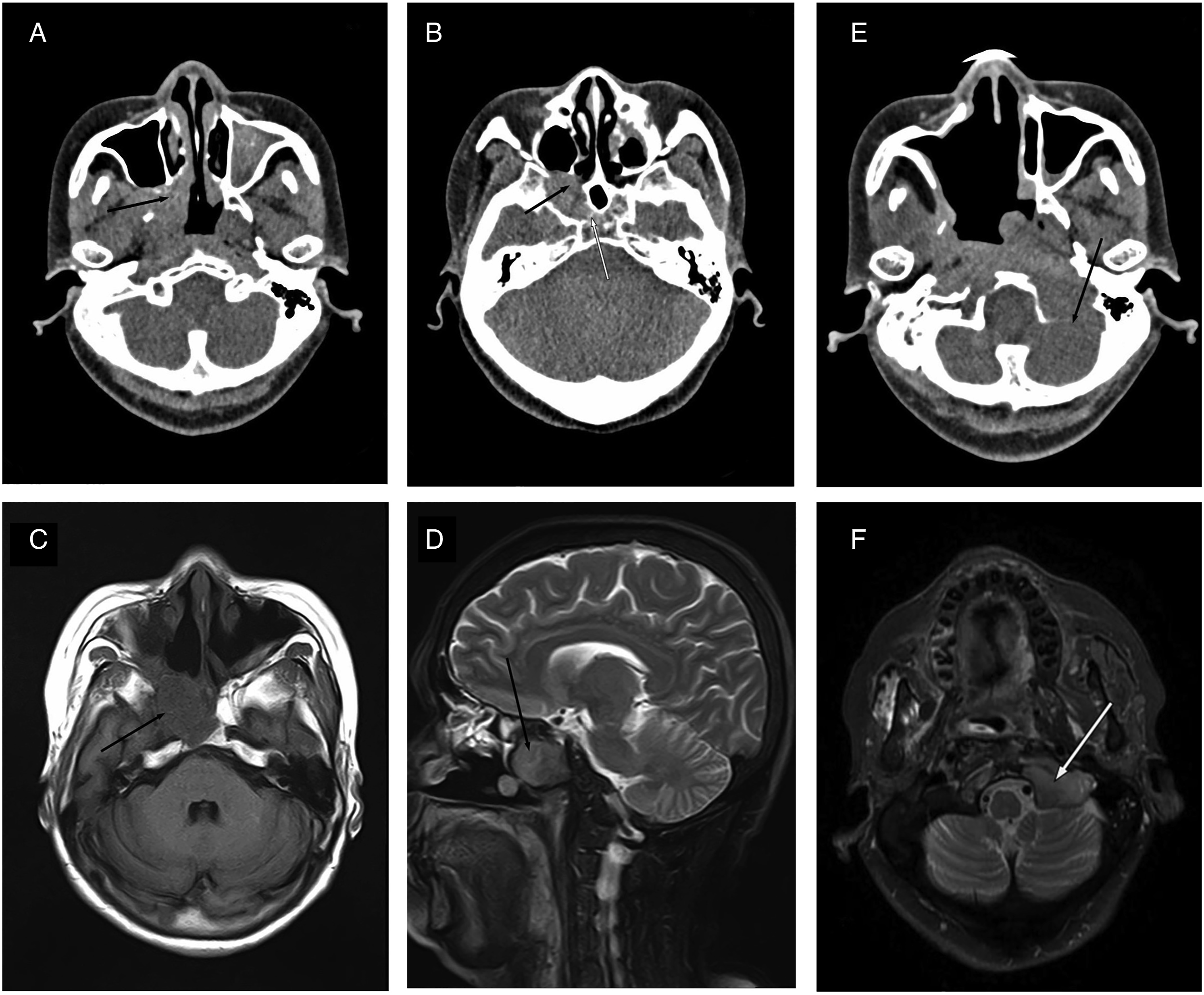
Discussion
To our knowledge, this is the first case in which COF resulted in osteosarcoma with a high Ki-67 index (Figure 2A). Mitotic activity was usually scarce or absent.
3
However, in this case, the tumor was a cell-rich neoplasm with extremely active proliferation and commonly observable mitotic figures (Figure 2B). Ki-67 is a nuclear protein antigen that is expressed during the G1, S, G2, and M phases, but not during the resting phase G0. Ki-67 levels are low in the G1 and S phases and rise to their peak levels during mitosis, followed by a sharp decrease in the mitotic phase.5,6 This characteristic has made Ki-67 a critical biomarker for assessing tissue proliferation.
7
Ki-67 expression is usually measured on paraffin sections by an immunohistochemical method using the MIB-1 antibody, similar to the approach used in this case. In general, the Ki-67 index is defined as the percentage of the total number of tumor cells with nuclear staining.
8
The Ki-67 index is usually not more than 3% even in aggressive and recurrent cases.9,10 However, the Ki-67 index in this case was 10%. Ki-67 is a potent indicator for prognosis and treatment of renal and breast cancer.11,12 A high Ki-67 index may be a risk factor for malignant transformation. SATB2, a nuclear protein marker of osteoblastic differentiation in benign and malignant mesenchymal tumors,13,14 and SMA were also positive in our case, supporting the diagnosis of COF (Figures 2C and 2D). (A), Immunohistochemistry showed strong staining for Ki-67 (original magnification, ×400. (B), Histopathologically, the neoplasm was cell-rich and mitotic figures were commonly observable (hematoxylin and eosin; original magnification, ×400). (C), Immunohistochemical assessment showed diffuse and strong staining for STATB2 (original magnification, ×400). (D), Immunohistochemical assessment showed diffuse and moderate staining for smooth muscle actin (SMA) in spindle cells (original magnification, ×400).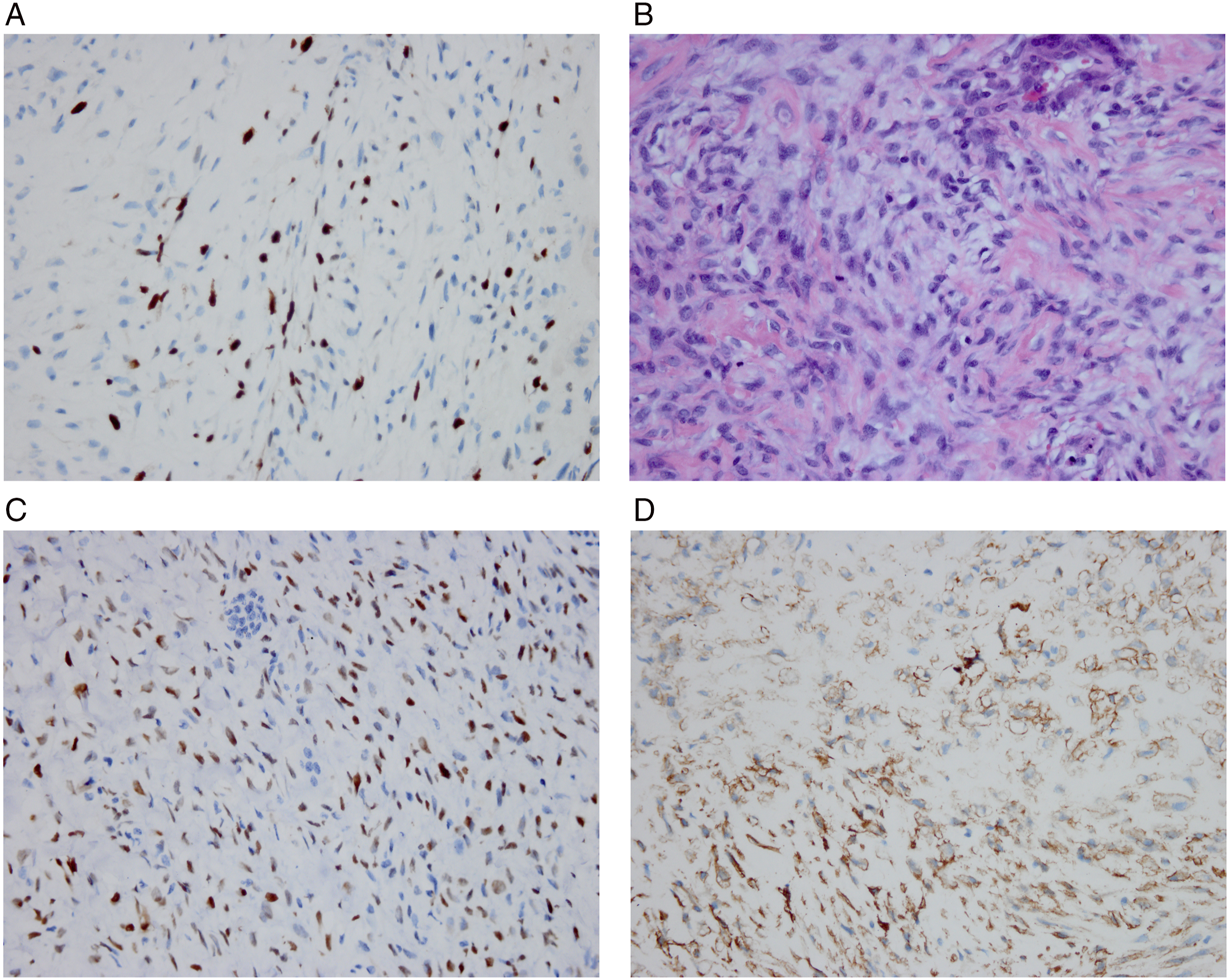
Various surgical options are included in the treatment of choice for COF. Radial resection, including marginal and segmental resection, is associated with much lower recurrence rates than conservative resection. 2 Some studies have insisted that complete surgical removal is the only curative treatment for COF. 15 When the maxilla and skull base are involved, endoscopic surgery is the first choice of treatment. 16 Although radiotherapy is contraindicated for COF because it can increase the risk of malignant transformation, 4 successful outcomes have been reported in patients treated with radiotherapy. In case 1, the tumor originated from the sellar region and showed invasion of the left cavernous sinus, which was treated with subtotal resection surgery, with some remnants in the cavernous sinus. A relapse was identified one month later, and a combined transsphenoidal and transcranial approach was performed to more aggressively remove the tumor, which was followed by adjuvant proton radiotherapy. No recurrence was recorded again. 17 In case 2, the patient was believed to be a poor candidate for a second surgery if the tumor recurred. Radiotherapy was recommended to minimize the risk of recurrence. 18 The total dose in case two was 50.4 Gy, the same as in the case we present. It is reasonable to conclude that malignant transformation was associated with radiotherapy; however, no obvious evidence supported this conclusion because the Ki-67 index remained at the same level after and before malignant transformation. Adjunctive radiotherapy was also shown to be effective in another case of recurrent ossifying fibroma in a horse. 19 The necessity and effectiveness of radiotherapy requires further study. It is crucial to identify the factors that predict malignant transformation. In cases showing a high risk of malignant transformation, more tissue may be excised to maintain the safety border and operate more carefully during the first surgery to reduce the recurrence rate and avoid malignant transformation. Radiotherapy and nine endoscopic surgeries caused considerable pain to the patient. To provide patients with optimal treatment, further studies in terms of pathophysiological mechanisms, high-risk factors for recurrence, and malignant transformation are required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by 1·3·5 project for disciplines of Clinical Research Incubation Project, West China Hospital, Sichuan University [Grant number 18HXFH026].