
Abstract
Association of developmental venous anomaly (DVA) and cavernous malformation (CM) of the posterior fossa is rare. If bleeding occurs, it must be assigned to the CM. Developmental venous anomalies, considered as normal vascular variation, are rarely symptomatic. Indeed, the CMs are true malformations and have a high bleeding potential.
Significance statement
Association of developmental venous anomaly (DVA) and cavernous malformation (CM) of the posterior fossa is rare. If bleeding occurs, it must be assigned to the CM. Developmental venous anomalies, considered as normal vascular variation, are rarely symptomatic. Indeed, the CMs are true malformations and have a high bleeding potential.
Introduction
Cavernous malformation (CM) associated with developmental venous anomaly (DVA) of the posterior fossa is rare vascular anomaly.1,2 The diagnosis of both vascular anomalies is easy in most typical cases although some lesions may present unusual radiologic features. Huge CMs can rarely mimic neoplastic masses because of their size. 1 Herein, we present an interesting case of huge CM mimicking a neoplastic mass on computed tomography (CT) scan and conventional magnetic resonance (MR) imaging. We discuss advanced MR imaging findings and histopathological features of this lesion.
Case presentation
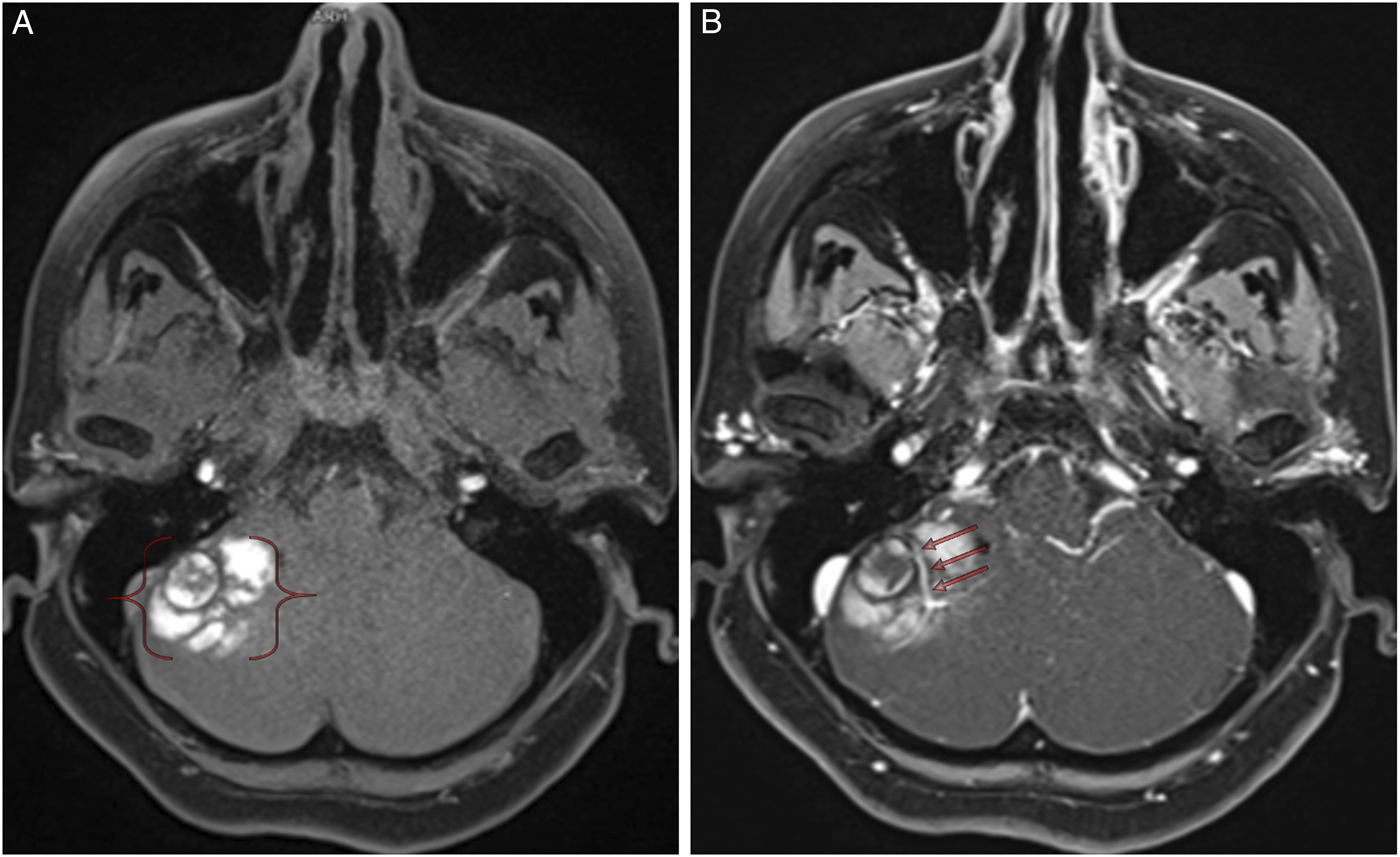
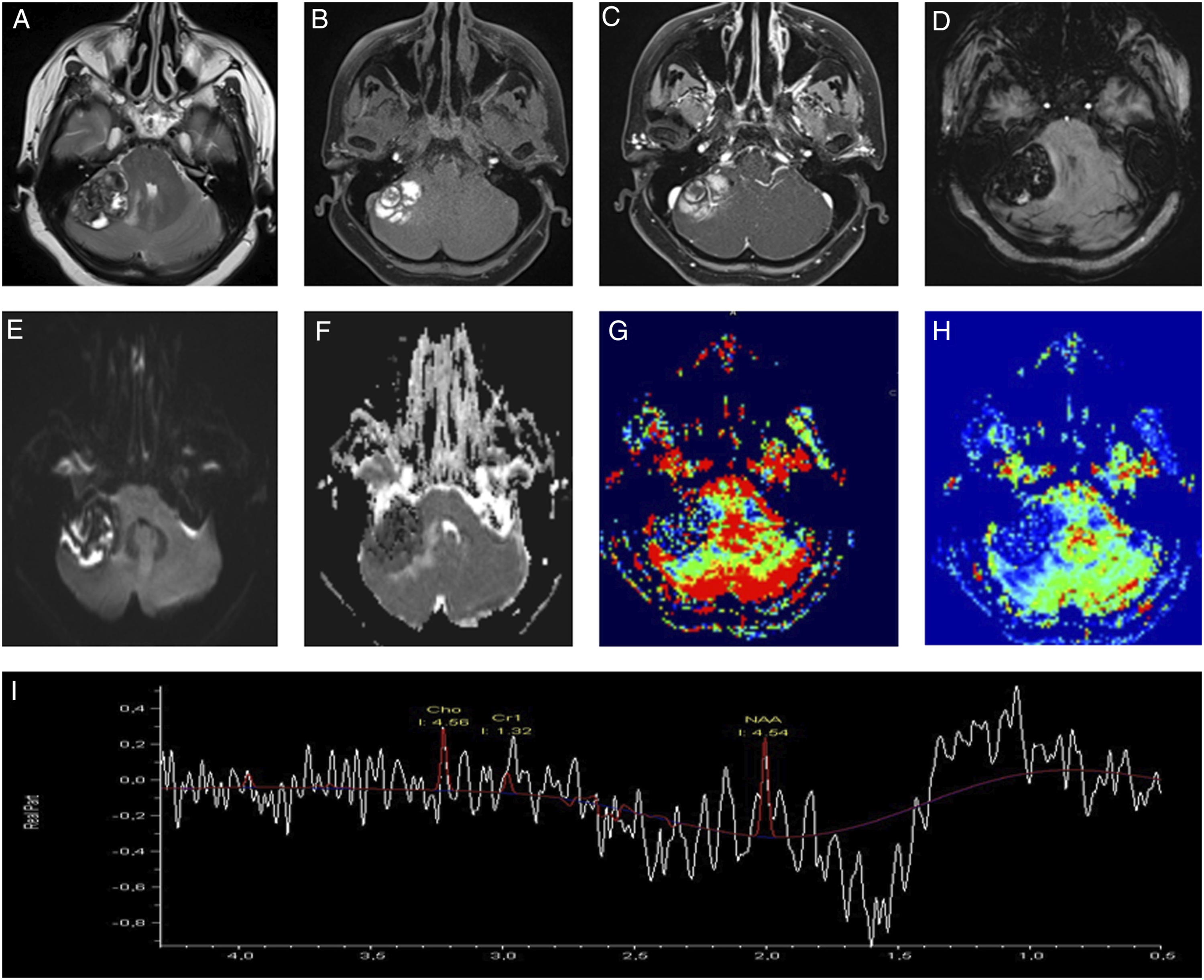
A 49-year-old woman was referred to our department with a history of progressive headache and acute ataxia. Non-contrast CT scan showed a hyperdense lesion in the right cerebellopontine angle cistern (Figure 1). Conventional MR imaging: Routin cerebral MR sequencesAdvanced MR imaging: MR spectroscopy, perfusion MR, SWI and DWI. Conventional MR imaging revealed a right cerebellar hemispheric mass with evidence of hemosiderin staining within and in the surrounding areas of the lesion (Figure 2A). Post-contrast T1-weighted imaging showed a relationship between DVA and CM (Figure 2B). Advanced cerebral MRI revealed a giant cerebellar cavernous angioma associated with DVA (Figure 3A-I). She underwent suboccipital craniotomy for resection of the lesion located in the right cerebellum. A dark reddish and mulberry-like cerebellar mass was observed intraoperatively, allowing the diagnosis of a CM. The feeding artery was identified in the right cerebellar hemisphere and was coagulated. Three months after surgery, she had near complete resolution of her symptoms. CT scan shows a hyperdense mass in the right cerebellopontine angle cistern. (A) Pre-contrast T1-weighted MRI reveals a right cerebellar hemispheric mass with evidence of hemosiderin staining within and in the surrounding areas of the cavernous malformation (parenthetical). (B) Post-contrast T1-weighted imaging shows a relationship between the developmental venous anomaly (red arrows) and cavernous malformation. MRI reveals a cavernoma associated with developmental venous anomaly (arrow) (A-C). Susceptibility-weighted imaging shows bleeding products within the mass (D). Diffusion and dynamic perfusion images show non-restricted (E-F) and hypoperfused lesion (G-H). MRS reveals no choline peak (I).
Conclusion
The association of CM and DVA was not well recognized until the advent of CT and MR imaging of the brain. 3 These anomalies are low flow vascular malformation of the brain. The DVAs are found in up to 2.6% of all autopsied brains.4,5 CMs have been reported in 0.3% to 0.5% in autopsy series and of patients undergoing MR imaging.4,5
Abe et al. 6 found a 23% rate of occurrence of the coexistence of CMs with DVAs by using unenhanced and contrast-enhanced MR imaging. The clinical presentation of these two cerebrovascular malformations is highly variable, ranging from an asymptomatic incidental discovery through radiographic imaging for nonspecific symptoms to associated headache, epilepsy, hemorrhagic stroke, and focal neurologic deficits.3,7
MR imaging is considered the most sensitive and specific method of detecting CMs.6,8,9 Typical MR findings of a CM include well-demarcated areas of mixed signal intensities with a hypointense rim on T1- and T2-weighted studies. 9 CT imaging of CMs has the ability to demonstrate calcifications and hemorrhage products.
DVAs can be missed on unenhanced MR and CT images as a result of slow venous blood flow and the low volume of blood. They are seen much more easily after contrast enhancement. Contrast material helps delineate the dilated medullary veins and the venous drainage pattern of the lesions. 6
This is a rare case of coexistence of cerebellar CM and DVA presenting with acute ataxia. Findings such as large size, smooth margin, hemorrhagic nature, and compression in the surrounding parenchyma may indicate a CM. The CM associated with DVA can be successfully imaged with MR imaging. A combination of proton MR spectroscopic imaging and cerebral perfusion MR imaging seem very useful to make differential diagnosis between the CM and hemorrhagic mass.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.