
Abstract
Atresia of the anterior nares is usually caused by acquired disorders such as iatrogenic damage, burns, and postoperative scar, but congenital cases are relatively rare. Here, we report a rare case of congenital anterior nostril atresia in an aged person with bilateral nasal congestion and snoring. The patient underwent surgery, and no recurrence was observed after a 2-year follow-up. To increase our understanding on this condition, we performed a literature review and discussed its associated clinical features, differential diagnoses, and treatment methods.
Introduction
Although anterior nostril atresia is usually caused by trauma, infection, surgery, burns, tumor resection, nasal intubation, and radiotherapy, congenital cases are rare. 1 During embryonic development, the anterior nostril is typically filled with epithelial plugs during the seventh week. After the plug is absorbed and disappears by the 13th–15th weeks, the nasal passages become fully developed and are open by the 16th week. However, if the plug is not completely absorbed and disappears, this leads to congenital anterior nostril atresia. 2
This project’s protocol was approved by the Ethics Committee of Gongli Hospital, Second Military Medical University.
Case Report
A 72-year-old man presented with a life-long history of bilateral nasal congestion and snoring.
Herein, we report the case of an aged patient who presented at the Otorhinolaryngology Outpatient Department of our hospital. He was recommended to undergo an anterior rhinoscopy which revealed almost complete atresia of both anterior nostrils (Figure 1A). (A) Preoperative photos of the anterior nostril. (B) Photo of the anterior nostril one week after the surgery. (C) Photo of the anterior nostril one month after the surgery.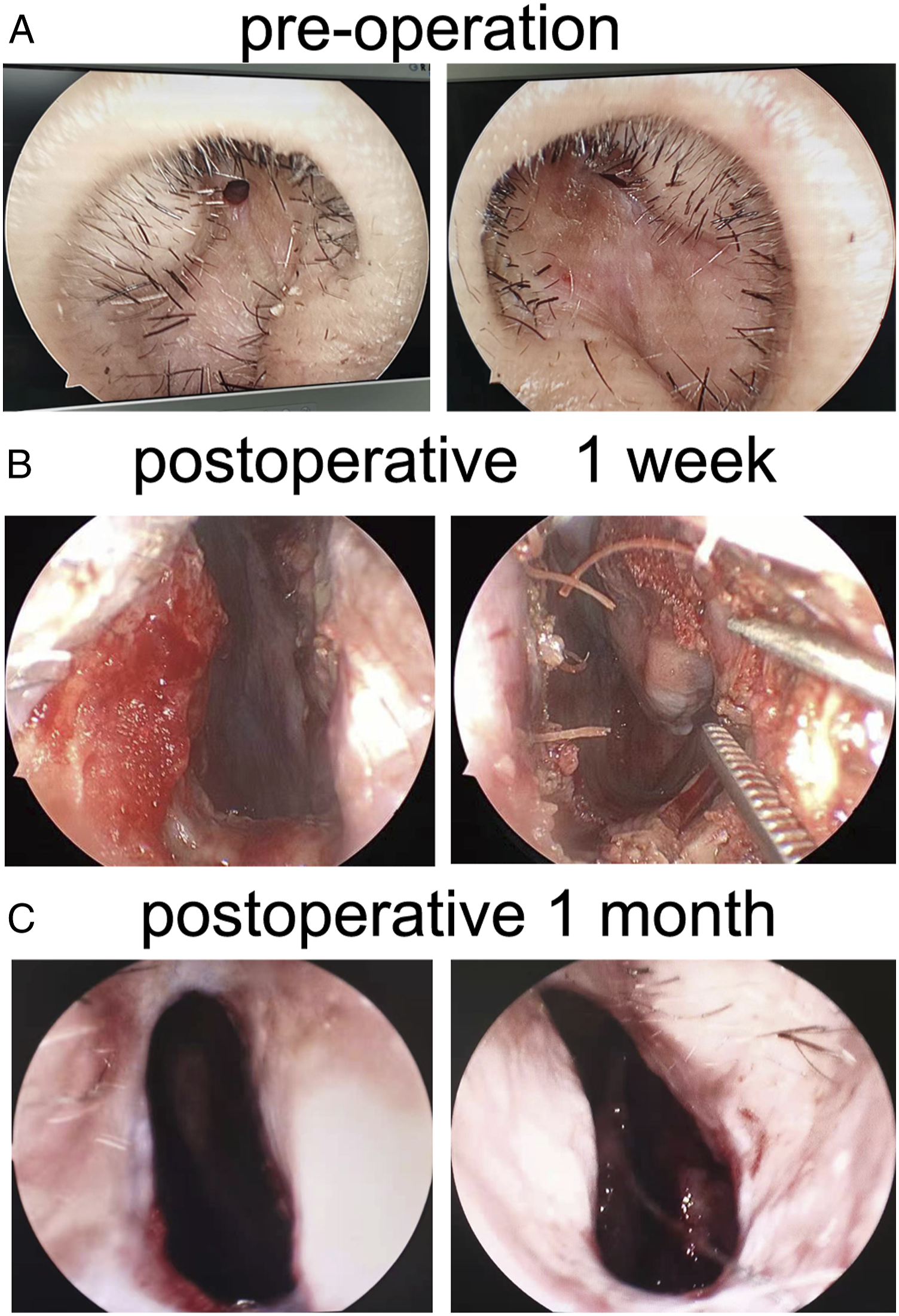
Computed tomography (CT) scan showed regularly shaped bilateral anterior nostrils, bilateral maxillary sinus, ethmoid sinus, frontal sinus, sphenoid sinus, no obvious abnormality in the nasopharynx and pharyngeal recess, but a significant deviation of the nasal septum. No choanal atresia was observed (Figure 2). Computed tomography showed atresia of anterior nostrils, bilateral maxillary sinus, ethmoid sinus, frontal sinus, sphenoid sinus cavity shape is standard, no obvious abnormality in the nasopharynx and pharyngeal recess, and nasal septum deviation. No atresia was observed in the posterior nostril.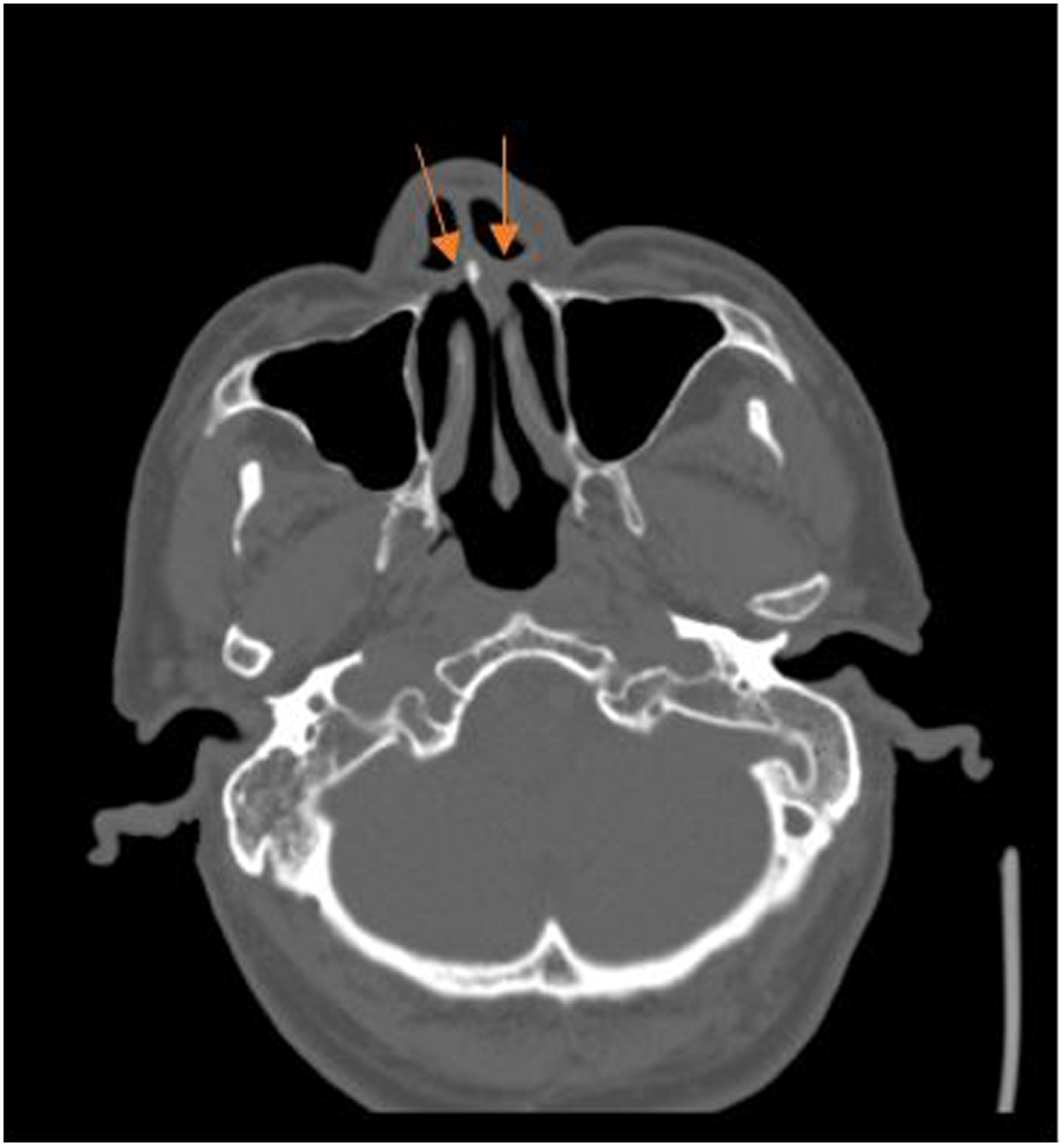
To secure a clear airway, we repaired the bilateral anterior nostril atresia via endoscopy. Anesthesia was performed on the subcutaneous tissues of the membranous atresia using 2% tetracaine. Under nasal endoscopy, the skin was cut in a circular arc along the left nasal apex hole to the nasal base of the nasal column. Then, the membranous skin was completely separated. The subcutaneous scar tissues were removed, the hyperplasia and protrusion of the nasal septum in the anterior nasal floor of the lower turbinate were ground with an electric drill, and the bony anterior nostrils were expanded. Next, we covered the anterior nasal septum with the membranous flap and sutured them with two stitches. Lastly, we applied a gelatin sponge to the anterior nostril wound and placed a silicone snorkel in the nasal cavity, which was then filled with a Vaseline gauze (Figure 3). Apply a gelatin sponge to the anterior nostril wound, place a silicone snorkel in the nasal cavity, and fill it with Vaseline gauze.
Postoperative pathology showed that the resected mucosa was accompanied by hyperplasia of the fibrous vascular tissue (Figure 4). Hematoxylin and eosin staining (HE) of the anterior nostril mucosa (original magnification ×100).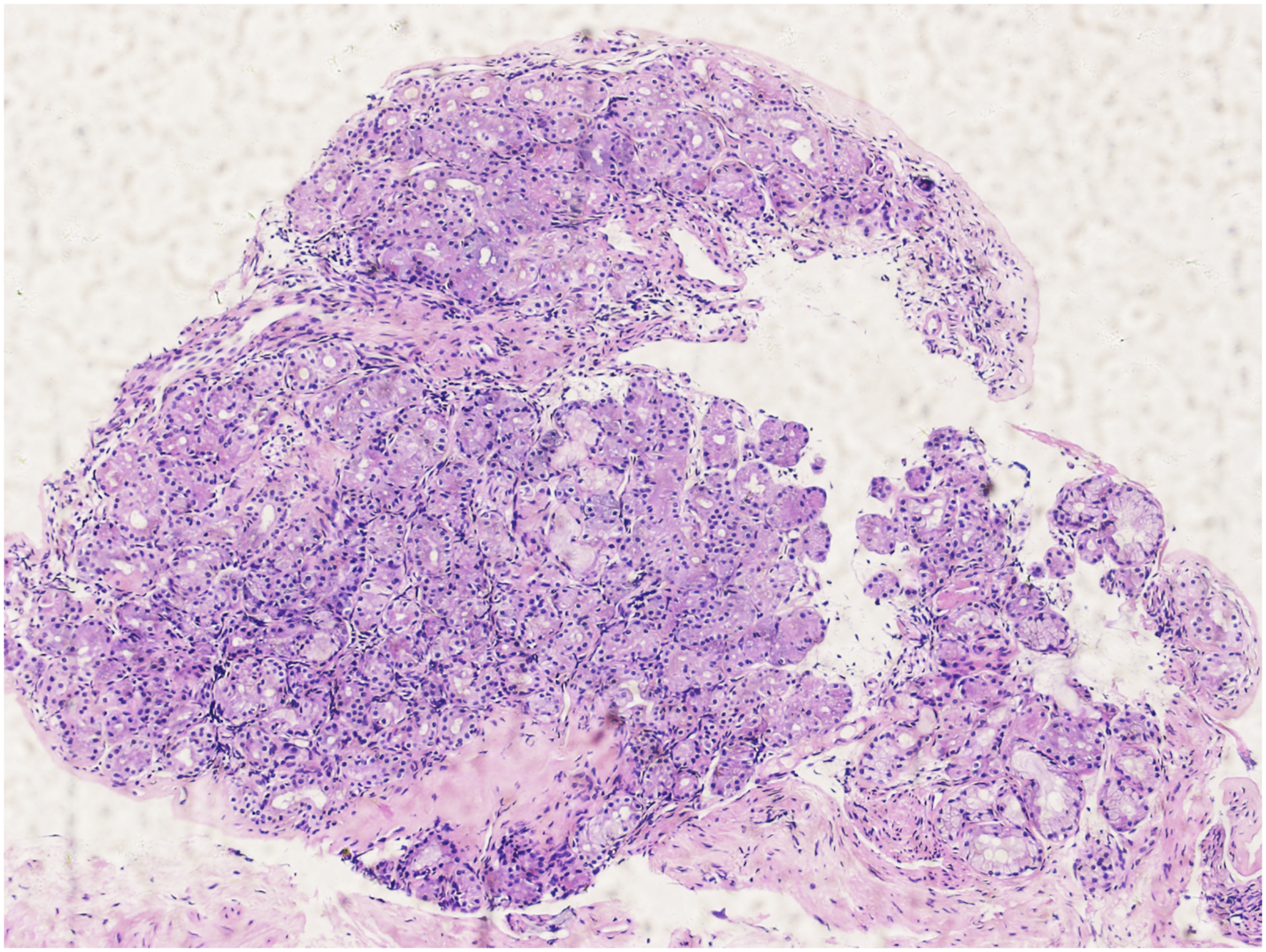
The patient had an uneventful postoperative recovery and was discharged on the fifth day after surgery. One week after the surgery, a follow-up nasopharyngoscopy in the outpatient department showed that the bilateral anterior nostrils were unobstructed (Figure 1B). The 1-month postoperative nasopharyngoscopy follow-up showed that both anterior nostrils were smooth, and no scar contracture was observed (Figure 1C). In the first two weeks after the surgery, the patient could only breathe through his mouth because he did not know how to breathe through the nose without opening his mouth. Two weeks after the surgery, he could breathe entirely through the nose. He had no symptoms of nasal congestion after a postoperative follow-up of more than two years.
Discussion
Anterior nostril atresia is mainly caused by acquired diseases. 3 Congenital anterior nostril atresia occurs if the epithelial plug in the anterior nostril is not absorbed and disappears during embryonic development. Congenital atresia of the anterior nares is a rare condition that results from the failure of canalization of the epithelial plug between lateral and medial nasal processes and is a rare cause of respiratory distress in newborns. 4
The width and depth of stenosis or atresia are often the same, while that of the inner nostril could range from narrow to completely closed. Membranous atresia or atresia tissue is thick and can reach deep into the nasal cavity. Atresia of the anterior nostril does not affect the development of the sinuses but can be accompanied by other malformations, such as nasal deformity of the affected side.
Obstruction of the nose is almost the only symptom and is proportional to the degree of atresia or stenosis. Newborns generally prefer to breathe through their nose. Typically, infants only mouth breathe when they cry. 5 If both sides of the front nostril are entirely closed, this could cause severe dyspnea and even death via asphyxia. For cases with only congenital bilateral nostril stenosis or unilateral anterior nostril atresia, although there is a certain degree of non-life-threatening dyspnea and suckling disorder after birth, such children are prone to aspiration pneumonia, which, in severe cases, could lead to death. 6 Therefore, congenital anterior nostril atresia is less rare in aged people.
The diagnosis of anterior nostril atresia is relatively straightforward, whereby CT can help to detect the presence of bone atresia, posterior nostril atresia, and sinus malformations.
Due to the front nostril and membrane closure, early diagnosis, meticulous evaluation, and expeditious and rational surgical management are essential for properly treating anterior nostril atresia. 7 However, careful attention should be paid to differential diagnosis with proliferative hypertrophy, posterior nostril polyp, nasopharyngeal meningocele, congenital dermoid cyst, and choanal atresia. 8
The principle of treatment is the same with congenital posterior nostril atresia. In neonatal patients with complete atresia, a small metal ventilator is placed in the mouth to maintain an open upper airway. After the ventilation tube is fixed, a gastric tube dropper or a special double-hole pacifier can be used for feeding and breathing. However, most neonates die during feeding due to various complications. Some argue that surgery is appropriate around the age of two years, while others argue that there is no contraindication to surgery within the first few hours of birth since most might not live to the age of two years without establishing a permanent breathing channel. Post-tracheostomy care is also tricky, and serious complications are likely to occur. About 10% of patients have membranous atresia, which can be dilated by puncture through the nasal route. In addition, 90% of the cases are considered osseous atresia, and the most appropriate operation remains through the posterior nasal foramen via the palatal approach. Presently, several types of surgical options are available, including microscopic and endoscopic surgery and intranasal dilatations with stenting. 9
Conclusion
Acquired diseases mainly cause anterior nostril stenosis or atresia, and congenital cases in the aged are less rare. Obstruction of the nose is almost the only symptom. The principle of treatment is the same with congenital posterior nostril atresia. It is more suitable for early surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the Young Medical Talents Training Program of Pudong Health Bureau of Shanghai (grant no. PWRq2021-06), Research Grant for Health Science and Technology of Pudong Health Bureau of Shanghai (grant no. PW2020B-10), Subject Construction Project of Pudong Health Committee of Shanghai (grant no. PWZy2020-06), and Pudong New Area Clinical Characteristic Discipline (PWYts2021-15).
Informed consent
This article has obtained written informed consent from patients for their anonymized information to be published in this article.
Data availability
All data generated or analyzed during this research are included in this published article. Data supporting the findings of this study are available from the corresponding author upon reasonable request.