
Abstract
Objectives
Brainstem auditory evoked potential (BAEP) monitoring was used to identify the influence of auditory function during cerebellopontine angle (CPA) surgery for cranial neuropathy via the retrosigmoid approach.
Methods
This prospective study included 20 patients who underwent CPA surgery for cranial neuropathy via the retrosigmoid approach with intraoperative BAEP monitoring and pure tone audiometry (PTA). The latency and interpeak latency were analyzed at each surgical step in combination with the pre- and postoperative PTA.
Results
Follow-up data were available for 17 patients. The mean pre- and postoperative PTA values were 25.65 dB and 20.70 dB, respectively. Two patients (2/17, 11.76%) developed hearing loss postoperatively. The latency of wave І significantly changed during direct auditory nerve manipulation and at the end of the surgery, while that of wave III only changed during direct auditory nerve manipulation. The appearance of wave V peak was delayed during CPA surgery.
Conclusions
CPA surgery for cranial neuropathy via the retrosigmoid approach can cause hearing loss to varying degrees, and intraoperative BAEP monitoring can reduce the occurrence of hearing loss. Intraoperative hearing function can be estimated by the latency of wave I. Hearing loss due to stretching of the brainstem can be estimated by the latency of wave III, and wave V is an early indicator of intraoperative hearing loss. Waves I and III remained stable both pre- and postoperatively, whereas wave V was unstable despite no surgery. Therefore, a precise operation and well-defined operative steps for surgeons during CPA surgery could facilitate maximal preservation of the anatomical structure and function.
Keywords
Introduction
Cerebellopontine angle (CPA) surgery for cranial neuropathy via the retrosigmoid approach, including microvascular decompression (MVD) and/or neurocombing and partial sensory rhizotomy (PSR), has become generally acknowledged as the main treatment method for idiopathic trigeminal neuralgia (TGN), hemifacial spasm (HFS), Meniere's disease, glossopharyngeal neuralgia, and other diseases. 1 -4 In recent years, the widespread use of minimally invasive surgical techniques and improvement in surgical methods have led to effective surgical performance around the nerve roots in the CPA area, with lower risks of complications and postoperative mortality. 5,6 However, this surgery has the risk of non-fatal functional diseases because of the complex structure of this area, which involves the brainstem, nerve roots, and important blood vessels. It is particularly important to ensure the maximal safety and surgical efficiency to avoid and reduce complications as much as possible.
A common surgical complication in patients undergoing CPA surgery is hearing impairment associated with damage to the vestibulocochlear nerve (CN VIII), such as postoperative hearing loss and often accompanied by tinnitus. 1 Hearing loss after this surgery ranged from 20 to 50 dB (1%–24%), but cases of total deafness was rare. 7 -10 In China, the reported rate of postoperative hearing loss was 12%, 11 and that in our own case series was approximately 10%. The exact cause of hearing loss is unclear, and the incidence of total deafness has drawn considerable attention. Most scholars believe that hearing loss is caused by a variety of factors, 12,13 one of which is excessive stretch and direct trauma to the CN VIII by instruments or a nearby coagulation during surgery. The other factors include excessive leakage of cerebrospinal fluid, which reduces the perilymph capacity; and manipulation of the labyrinthine artery and/or the anterior inferior cerebellar artery, or exposure of the labyrinthine artery, which causes vasospasm and inner ear hypoxia-ischemia. In short, regardless of the cause, the complications of functional CPA surgery are very serious. Hearing preservation during CPA surgery is one of the most intriguing and interesting aspects for oto-neurosurgeons.
Over the past decade, intraoperative neurophysiology has significantly evolved and currently offers live monitoring of neural structure integrity. Hearing preservation has been achieved by significant advances in skull base microsurgical techniques and intraoperative neuromonitoring. 14,15 Thus, dysfunction can be identified early and the surgical management or operating conditions can be modified promptly to prevent permanent structural damage. The use of intraoperative brainstem auditory evoked potential (BAEP) monitoring is generally acknowledged to reduce the risk of hearing impairment. Many studies have reported the effectiveness of intraoperative BAEP monitoring to reduce hearing loss with posterior fossa surgery (especially acoustic neuromas/vestibular schwannoma) in western countries; this has also been applied in the neurosurgery discipline in a few tertiary hospitals in China.
To reduce the complications of postoperative hearing loss, we conducted an application study on intraoperative auditory monitoring of sigmoid sinus via the retroorbital surgical approach.
In the current study, we analyzed the intra and postoperative BAEP findings during specific microsurgical actions, especially the waves I, III, and V were monitored for changes in the amplitude, latency, and interpeak latency. We compared the latency of waves I, III, V, I-III, III-V, I-V, and that between the preoperative, intraoperative, and postoperative waves of patients with side BAEPs. Additionally, we assessed the preoperative and postoperative changes in waves I and V, and the auditory brainstem threshold (ABRt). We further explored the main factors underlying intraoperative auditory changes during the sigmoid sinus functional surgery of the CPA region to provide a theoretical basis for the avoidance and reduction of complications of intraoperative hearing loss and for judging the requirement of timely treatment for postoperative hearing loss. Thus, the results of these assessments could provide the most significant monitoring value for clinicians when making decisions on positive treatment.
Methods
Selection of patients
Demographics of the patient.
Surgical procedure
We preferred the retrosigmoid approach in the functional CPA surgery for cranial neuropathy because it offers a series of advantages, such as adequate control of bleeding, direct and adequate exposure of the CPA, easy identification of the facial and cochlear nerves at their root entry zone, and at the distal end in the internal auditory canal. All patients underwent surgery via the retrosigmoid approach under general anesthesia with propofol and fentanyl. Patients underwent CPA surgery in the park-bench position through a circular craniotomy (maximum diameter, 20-25 mm) centered around the emissary vein followed-up to the posterior margin of the sigmoid sinus.
In the 10 cases of HFS, these procedures additionally included facial nerve root combing in 3 patients and microvascular decompression neurocombing (MVDC) in 7 patients. Among the 6 cases of TGN, MVD was performed in 2 patients and MVD + PSR in 4 patients. A vestibular neurectomy was performed in one patient with recurrent MCS of the vestibulocochlear nerve who underwent MVD 2 years preoperatively. Intraoperatively, the body temperature of the patients was monitored continuously and maintained within 37 ± 0.5°C.
Study design
Preoperative auditory investigations
The charts and operation records of these patients were collected. Preoperative hearing evaluation consisted of pure tone audiometry (PTA) performed one week preoperatively. PTA was calculated as the average of the thresholds at 0.5, 1.0, 2.0, and 4.0 kHz. The patients were explained of the tests in detail, and all patients voluntarily participated in the audiometry. Hearing status was considered normal when PTA corresponded to the absence of loss or a loss ranging between 0 and 25 dB. 12 Patients with significant hearing loss usually underwent audiometric follow-up within 1–4 weeks after their first audiometric evaluation. A significant audiometric change at the last follow-up was considered permanent hearing loss. 13 ABR was recorded in all patients by the same clinical investigator who performed the intraoperative monitoring. None of the 17 patients had a preoperative hearing disability. 3
Intraoperative BAEP monitoring
Intraoperative BAEP monitoring was performed using a Nicolet Spirit system (Nicolet Biomedical, Wisconsin). Three subcutaneous needles were placed for recording—the active electrode on the ipsilateral earlobe, reference electrode at the vertex, and earth on the forehead. With a duration of 10 ms, the stimulation parameters consisted of alternating condensation with an intensity of 90 dB and contralateral white nose of 50 dB to avoid contributions from the contralateral ear. ABR obtained after averaging up to 2,000 click stimulations were analog-filtered using a filter with a bandwidth of 100–1500 Hz. 3,4
The main concern in BAEP monitoring was the ability to identify changes in the responding components to measure ABRt, amplitudes of the waves of interest (Wave I and V), latency of the waves of interest (Wave I, III, and V), and interpeak latencies of interest (Wave I-III, III-V, I-V) for each trial.
This study attempted to demonstrate the changes in intraoperative ABR findings under surgical stress. For this purpose, four surgical time points from the usual sequence of surgical maneuvers were investigated as follows: (1) the time after induction of anesthesia (IOA), (2) time point of nerve foot exposing (NFE), (3) time point of nerve foot manipulation (NFM) (MVD and/or neurocombing and/or PSR), and (4) at the end of surgery (EOS).
Postoperative auditory investigations
PTA was performed in all patients before discharge, usually within two weeks after surgery. A decrease of more than 15 dB in the postoperative average PTA threshold, compared with the preoperative value, was considered significant. 13 Control ABRt recordings were performed simultaneously (at the end of the first postoperative week) by the same clinical investigator. Postoperative tympanometry and otoscopy were performed before the audiometry to detect middle ear dysfunction associated with the opening of mastoid cells during craniotomy.
Comparison of preoperative, intraoperative, and postoperative BAEP
The ABRt and amplitudes of waves I and V were measured to identify the pre- and postoperative changes in hearing. Moreover, we compared the latencies of the waves of interest (wave I, III, and V) and the interpeak latencies of interest (Wave I-III, III-V, and I-V) among the pre-, intra- (four sections/stages/phases), and postoperative values to identify the predominant factors that influence the auditory function in functional CPA surgery performed via the retrosigmoid approach.
Statistical analyses
The statistical significance of differences in wave latency was determined by analysis of variance, and the least significant difference was used for each variable by comparison of mean wave delay at successive time points during the surgery.
Results
Results of hearing tests
The average pure tone thresholds of 0.5, 1.0, 2.0, and 4.0 kHz were compared pre- and postoperatively in all patients. The mean postoperative PTA value in the series was 21 dB (standard deviation [SD], 8) and that preoperatively was 26 dB (SD, 13) (data not shown in tables or figures). Two (12%) patients developed deafness postoperatively. One patient with trigeminal MVD manifested a 20-dB hearing loss in the high-pitch range. Another patient experienced a 45-dB hearing loss; this patient had an adhesion between the acoustic and facial nerve, which was identified intraoperatively during MVDC. Both patients with hearing loss had this adhesion on the ipsilateral side and all of these were of the sensorineural type. These two patients showed no improvement in hearing during the follow-up period.
Analysis of BAEP changes for each component
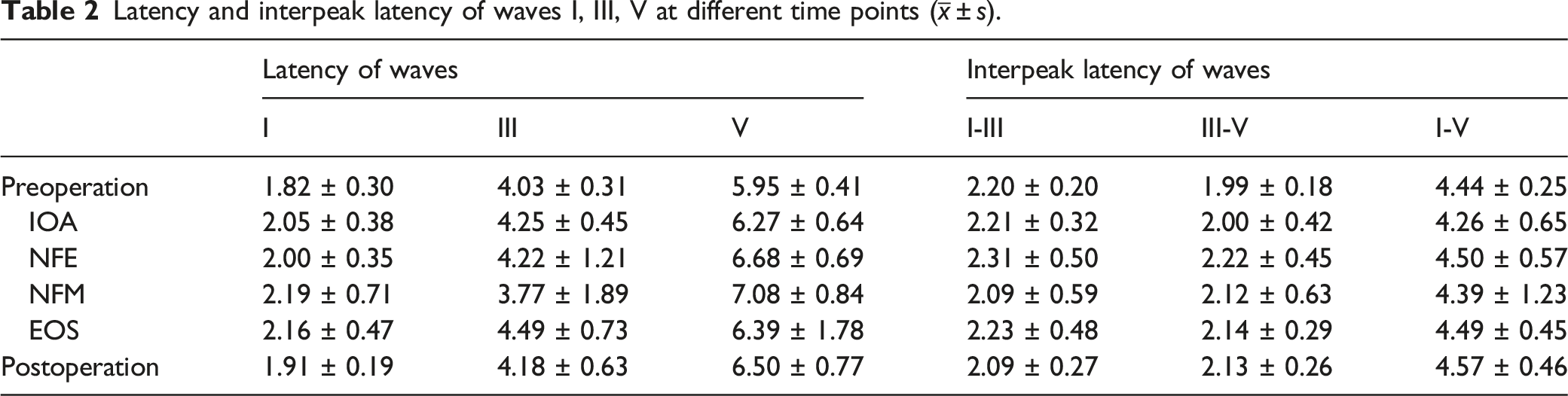
To intraoperatively assess the changes in BAEP components and the factors influencing them, ABRt, wave amplitudes, latencies, as well as the interpeak latencies of waves I, III, and V were measured during each step of the surgery as aforementioned in the methods section. The latency and interpeak latencies of waves I, III, and V measured pre-, intra- (IOA, NFE, NFM, and EOS), and postoperatively are presented in Table 2.
Latency and interpeak latency of waves I, III, V at different time points (
ABRt values
Preoperative ABRt in the group of 17 successfully monitored patients ranged from 30 to 50 dB HL (mean, 41; SD, 7 dB HL), whereas postoperative ABRt elevations ranged from 30 to 75 dB HL (mean, 47; SD, 10 dB HL). Results of paired t-test showed no statistically significant difference in ABRt values between the pre and postoperative periods (P = .799).
Wave I
The mean pre- and postoperative amplitudes of wave I and wave V in the series were 0.25 µV (SD, 0.04) and 0.30 µV (SD, 0.11), respectively. There was no statistically significant difference in the pre- and postoperative wave I amplitudes (P = 0.394, paired t-test). On analyzing the latency of wave I at different surgical time points by LSD test, a statistically significant prolongation was revealed only in NFM and EOS intraoperatively, as compared with preoperative values (P = .014 and P = .025, respectively) (Figure 1). This prolonged was less pronounced in repeated measures, and 2 weeks later, the latencies of wave I returned to preoperative values. Latency of wave I at different time points.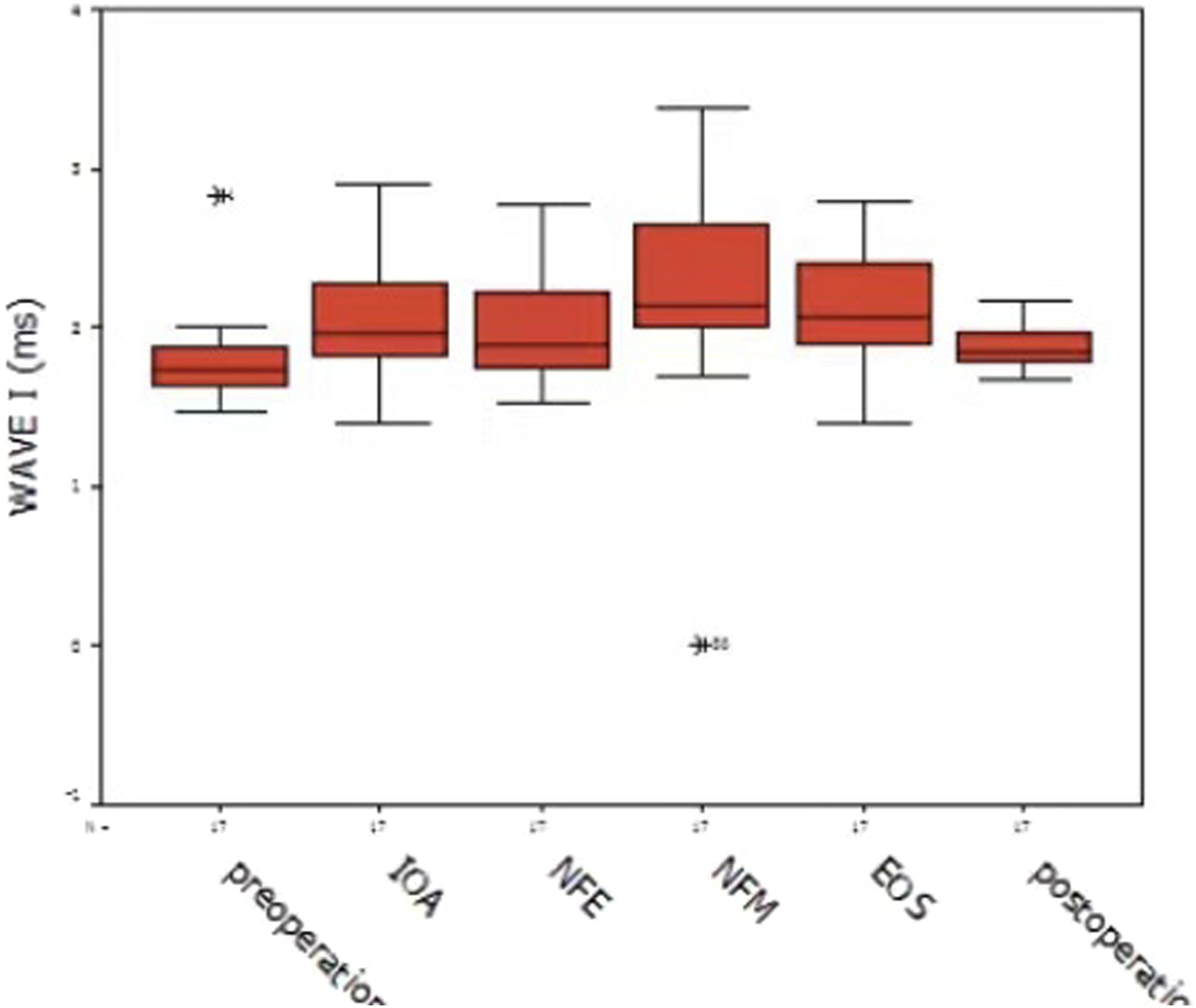
Wave III
The LSD test found a statistically significant difference in wave III latency between NFM and EOS (P = .042) (Figure 2). Compared with EOS, there was a slight increase in wave III latency at NFM and at postoperative recovery. No statistically significant difference was found among the preoperative, postoperative, and other surgical time points. Latency of wave III at different time points.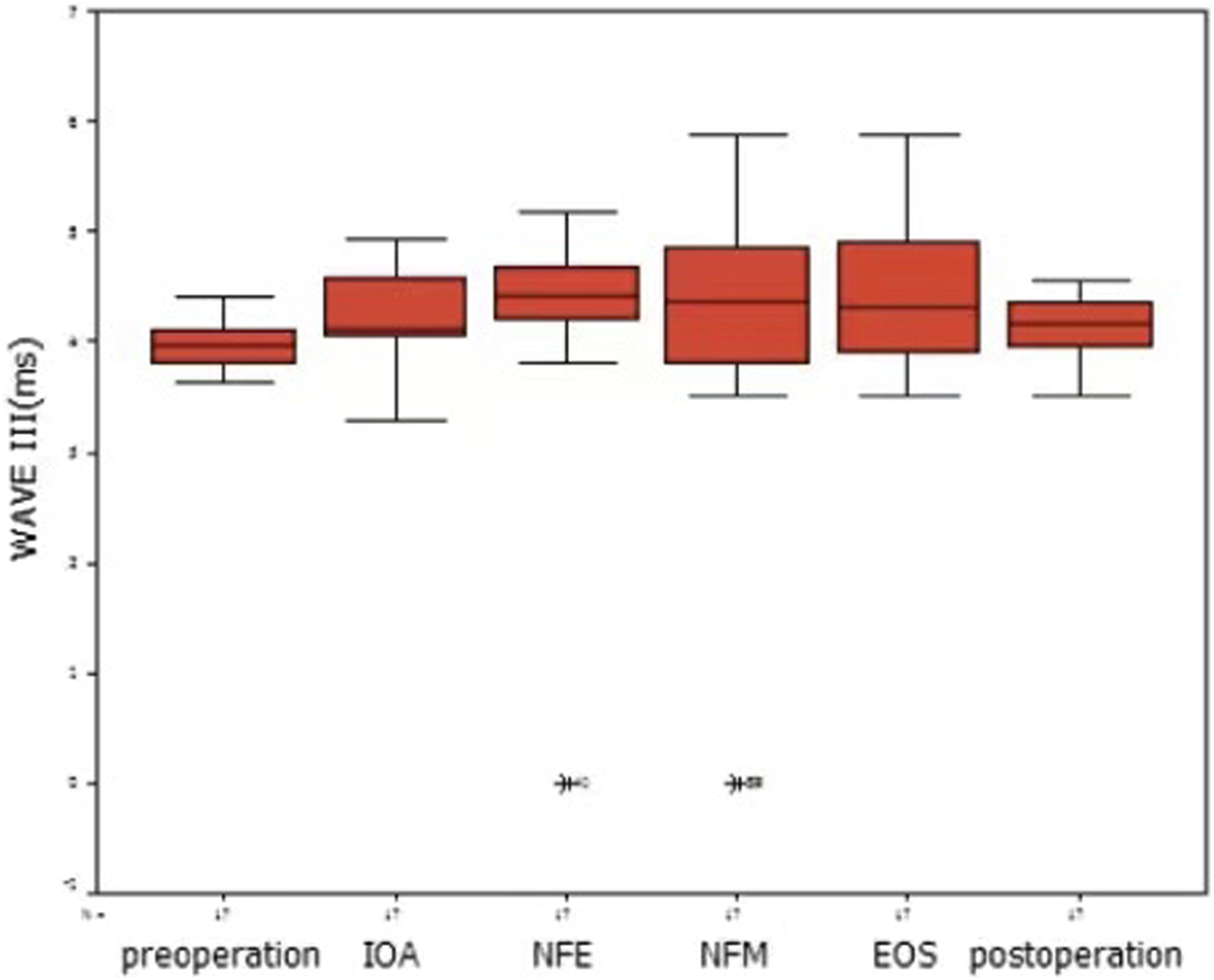
Wave V
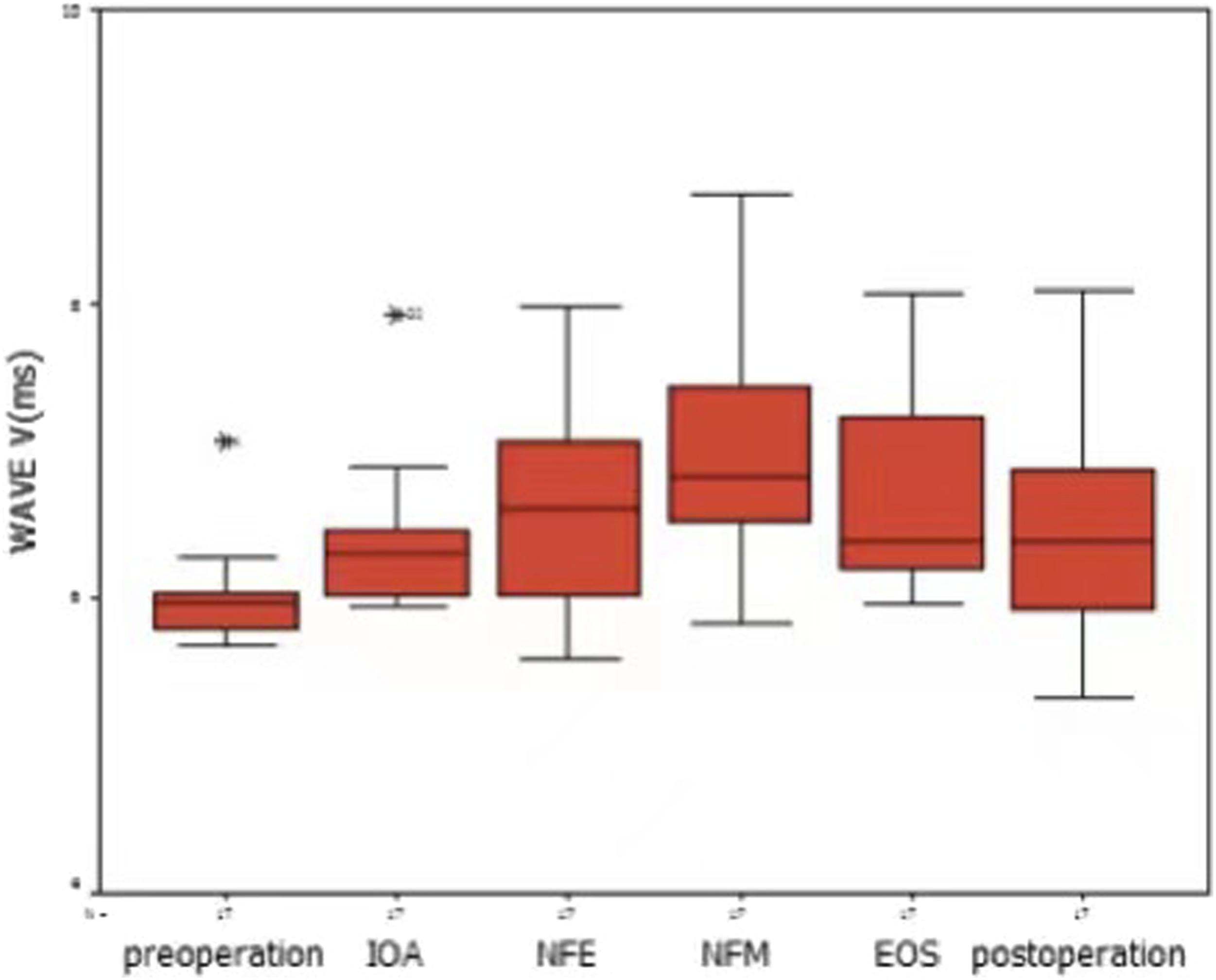
On analyzing the amplitude of wave V by one-way analysis of variance, NFM was the only surgical time point to achieve statistical significance compared with the preoperative value (P = .016, LSD test) (Figure 3). Wave V amplitudes decreased significantly at NFM and returned to preoperative values at EOS. There was a statistically significant difference in wave V latency between NFM and preoperative values, IOA, and EOS (P = .001, P = .016, and P = .038, respectively; LSD test) (Figure 4). Amplitude of wave V at different time points. Latency of wave V at different time points.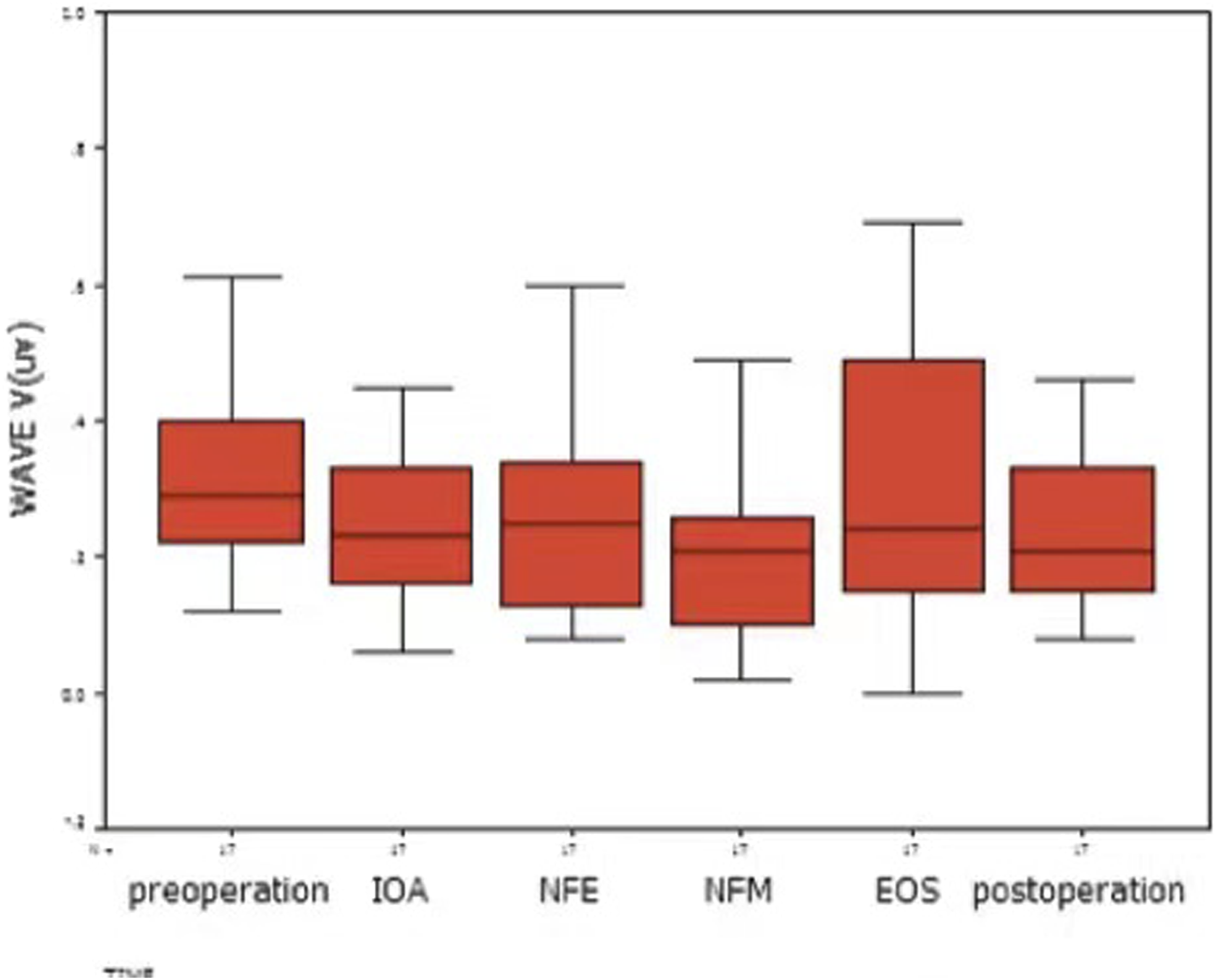
Interpeak latencies of waves I-III, III-V, and I-V
The LSD test found no statistically significant difference in the interpeak latencies of waves I-III, III-V, and I-V among the preoperative, postoperative, and other surgical time points (Figure 5).
Interpeak latency of waves I-III, III-V and I-V at different time points.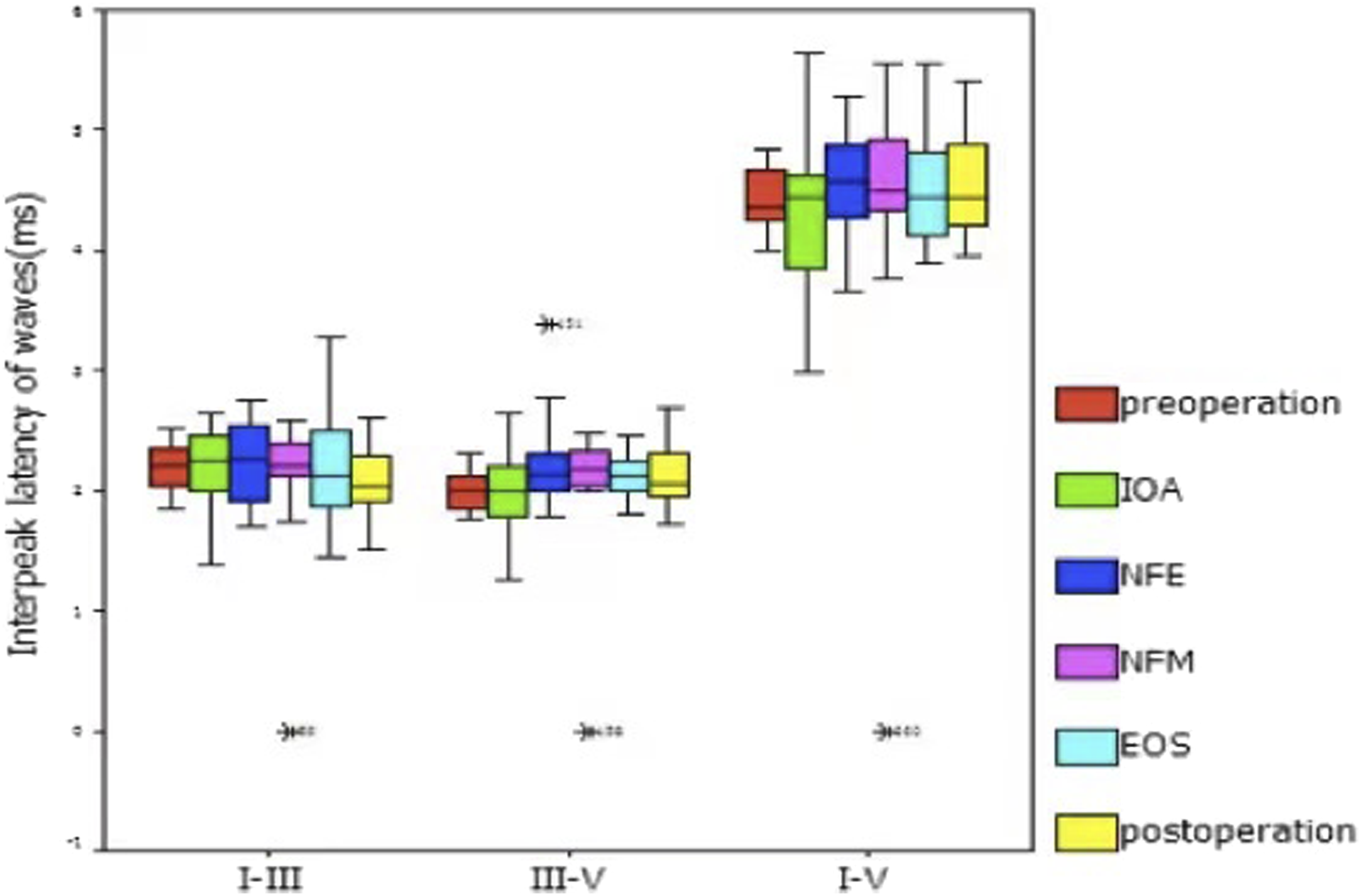
Discussion
Intraoperative monitoring of BAEP has been shown to reduce the risk of hearing impairment with surgery in the region of CPA. 16 -19 Radtke et al 17 retrospectively compared the auditory morbidity of 152 patients with posterior fossa microvascular decompressive surgery before and after the introduction of intraoperative BAEP, which found 6.6% patients suffered a profound hearing loss in the nonmonitored group, while none of patients suffered a profound hearing loss in the monitored group. Similar findings were reported by Schramm et al 18 and Wiedemayer et al. 19 These reports are strong demonstration of a significant decrease in postoperative deficit directly associated with the use of intraoperative monitoring.
BAEP monitoring has been used during surgery via the retrosigmoid approach since the mid-1980s. This surgery eliminates the lesion to the maximum extent and preserves neurological function. Although the retrosigmoid approach for acoustic tumors facilitates better intraoperative monitoring of the acute facial nerve, it can improve the accuracy and safety of surgery via the retrosigmoid approach. Hearing preservation is key to successful surgery. The latency of waves I, III, and V and interpeak latency of I–III, III–V, and I–V are important signs of a successfully preserved hearing function. The auditory structures that generate the auditory brainstem responses are believed to be as follows 20,21 : (i) waves I, II, and III are generated by the auditory branch of the cranial nerve VIII and lower brainstem; and (ii) waves IV and V are generated by the upper brainstem. Pathological changes, both in the auditory nerve and brainstem, affect BAEP.
Traction of the cochlear nerve in the medial direction results in amplitude reduction or loss of wave I, whereas pulling the nerve in the lateral direction results in amplitude reduction or loss of wave III, which is the most sensitive and earliest sign of hearing loss. 21 Wave I and III disappear before wave V during surgery. We should pay more attention to the amplitude change of wave III during neural surgery. The present study showed that the latency of wave I significantly changed during and at the end of the neural surgery, but showed no difference after induction of anesthesia, on neural exposure, or postoperatively. 20 The present study suggests that the latency of wave I is relatively stable and remains the same postoperatively, and it is only affected by direct trauma, but not by anesthesia or neural exposure. Therefore, presumably, the latency of wave I could estimate intraoperative hearing function. The most stable sign is the latency of wave III, which only changes during neural operation, and is not affected by after anesthesia induction, on neural exposure, or postoperatively. This reversible change may be related to the stretching of the brainstem, which recovers after the surgery without any damage to the acoustic nerve. Therefore, it is expected that hearing loss resulting from stretching of the brainstem can be estimated by the latency of wave III.
As wave V of BAEP was the most unstable, we also analyze wave V, consistent with previous studies. 9,16,22 -24 The appearance of wave V peak was delayed during CPA surgery, especially during the decompression step of MVD and during cerebellar retraction, and it is recognized as a sign of cochlear nerve damage. 3,6,25 The current study shows that the latency of wave V significantly changes at 6 time points (intraoperatively, after anesthesia induction, on neural exposure, during the neural operation, at the end of the operation, and postoperatively), especially during neural operation. The amplitude of wave V changed significantly only during the neural operation. The type of surgery is important when interpreting significance of changes of wave V, in non-CPA surgery, hearing loss occurs usually only with permanent loss of wave V; even in this situation, a large number of patients may have preserved hearing. 16 Loss of wave V during CPA surgery was the warning sign that associated with postoperative HL, and the latency prolongation of 1.0 milliseconds with an amplitude decrement of at least 50% is also an important warning sign associated with postoperative HL. 9,16,24 It is believed that wave V is the most sensitive and unstable sign, affected by multiple factors. The results of this study suggest that wave V is an early but not the only indicator of intraoperative hearing loss.
The study of auditory function examined 84 consecutive patients with hemifacial spasm after microvascular decompression, and the results are expressed as a pure tone average for all patients. Eight patients (10%) had hearing impairment with a decrease in pure tone average of >20 dB, and two patients (2%) experienced a definitive and complete hearing loss on the operated side. 5 Our study compared the pre and postoperative pure tone tests of 17 patients. Two patients (12%) developed postoperative hearing loss. One patient with trigeminal MVD had hearing impairment with a 20-dB decrease in pure tone average. One patient with hemifacial spasm in whom an acoustic-facial nerve adhesion was identified intraoperatively, experienced hearing loss with a decrease in air conduction threshold of 45 dB and a bone conduction threshold of 35 dB.
The current study investigated auditory function through at 6 time points during the operation and found that auditory function was mainly affected by the operation. The delay of latency and interpeak latency, as well as the reduction in the amplitude of each wave (especially the latency of wave V and interpeak latency of waves I-V and III-V) are closely related to tumor removal, stretching of brainstem, and electric coagulation. Both latency and amplitude are important in the alarm system that warns surgeons to operate gently, with intervals (pause the operation for 10-30 minutes for recovery of the ordinary wave), to avoid irreversible neural damage. Improvement in surgical techniques can help to achieve good surgical results (without any serious complications) and maximally preserve the anatomical structure.
Although BAEP represents the standard and main tool for intraoperative monitoring of hearing, this far-field technique has some limitations due to the necessity of signal amplifying and averaging, and the failure of recordings during sensitive maneuvers such as electrocautery and drilling of the internal auditory canal. 26 -29 Electrocochleogram (ECochG) is a near-field auditory evoked potential test, which takes little additional clinic time following stimulus onset and may improve the neurodiagnostic utility of the BAEP. 30 -32 ECochG is no global test for hearing since its action and summating potential reflects the neuronal activity of the cochlea and the most distal part of the auditory nerve, nevertheless, ECochG may be a helpful supplementary tool for preserving functional hearing during surgery. 5 Whether combined application of ECochG and BAEP monitoring is effective for auditory function preservation during CPA surgery via the retrosigmoid approach is worth further investigation.
In summary, hearing preservation is important for a successful operation. The results of intraoperative BAEP monitoring depend on the size, histological type, and location of the lesions, as well as on the adopted surgical approach. Improved hearing preservation can be achieved by the following: (1) controlling the monitoring environment, technique, and other influencing factors; (2) Information should be provided to surgeons in time (avoiding redundant error information while discovering useful messages), providers should also notify surgeons in a timely and accurate manner; and (3) Surgeons should be well aware of the operative steps and subtle shifts of waves.
Conclusion
The current study reports that auditory function is mainly affected by surgery. CPA surgery via the retrosigmoid approach for cranial neuropathy can cause hearing loss to varying degrees. BAEP may be a valuable tool for monitoring patients undergoing such surgeries. Intraoperative hearing function can be estimated by the latency of wave I. Hearing loss resulting from stretching of the brainstem can be estimated by the latency of wave III, and wave V is an early indicator of intraoperative hearing loss. Waves I and III remain stable at all time points before, during, and after the surgery, whereas wave V wave is unstable even without any operation. A precise operation and well-defined operative steps during CPA surgery may modify the surgical maneuvers intraoperatively. Vigilant intraoperative BAEP monitoring and adequate analysis of the recorded BAEP changes could maximally preserve the anatomical structure and function. More extensive studies with large sample size are needed to validate the intraoperative BAEP changes during CPA surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by a grant from the Academic Leader Program of Pudong Health Bureau of Shanghai (PWRd2018-05), the Scientific Research Program of Shanghai Municipal Health Commission (202140405), the Youth Medical Talent Training Program of Pudong Health Bureau of Shanghai (PWRq2020-50), the Key Specialty Construction Project of Health Bureau of Shanghai (ZK2019C06), Subject Construction Project of Pudong Health Committee of Shanghai (Grant No. PWZy2020-06), Pudong New Area Clinical Characteristic Discipline (PWYts2021-15).
Research ethics and patient consent
This is a retrospective original research. Approval for the release of data for this project was conducted according to the World Medical Association Declaration of Helsinki and granted by the Ethical Committee of Shanghai Pudong New Area Gongli Hospital. These patient provided written informed consent.
Data availability
Some or all data, models, or code generated or used during the study are available in a repository or online in accordance with funder data retention policies.