
Abstract
Around 75% to 90% of people who experience a traumatic brain injury (TBI) are classified as having a mild TBI (mTBI). The term mTBI is synonymous with concussion or mild head injury (MHI) and is characterized by symptoms of headache, nausea, dizziness, and blurred vision. Problems in cognitive abilities such as deficits in memory, processing speed, executive functioning, and attention are also considered symptoms of mTBI. Since these symptoms are subtle in nature and may not appear immediately following the injury, mTBI is often undetected on conventional neuropsychological tests. Current neuroimaging techniques may not be sensitive enough in identifying the array of microscopic neuroanatomical and subtle neurophysiological changes following mTBI. To this end, electrophysiological tests, such as auditory evoked potentials (AEPs), can be used as sensitive tools in tracking physiological changes underlying physical and cognitive symptoms associated with mTBI. The purpose of this review article is to examine the body of literature describing the application of AEPs in the assessment of mTBI and to explore various parameters of AEPs which may hold diagnostic value in predicting positive rehabilitative outcomes for people with mTBI.
Keywords
Introduction
Traumatic brain injury (TBI) is an acquired injury to the brain that can occur following sudden trauma to the head (National Institute of Neurological Disorders and Stroke, 2017). The extent of brain injury is typically determined during the acute phase following neurotrauma. Based on the clinical indices of the Glasgow Coma Scale (GCS) and the post-traumatic amnesia (PTA) duration, severity of TBI is categorized as mild, moderate, or severe. The GCS is recorded as a composite score consisting of three individual components: eye-opening, verbal response, and motor response. A GCS score in the range of 13 to 15 is interpreted as mild TBI (mTBI), 9 to 12 as moderate TBI, and 3 to 8 as severe TBI (Teasdale & Jennette, 1974). The duration of PTA refers to the time interval between the injury and when the person is oriented and able to form and recall new memories. A PTA of less than 24 h is categorized as mTBI, 1 to 7 days as moderate TBI, and more than 7 days as severe TBI (Friedland, 2013; Nakase-Richardson et al., 2011). mTBI is used interchangeably with other terms, such as mild closed head injury, MHI, or concussion, all of which represent the same level of brain dysfunction (Nuwer, Hovda, Schrader, & Vespa, 2005). The Mild Traumatic Brain Injury Committee of the American Congress of Rehabilitation Medicine (1993) defines mTBI as: A condition in which a person has sustained a traumatically induced physiological disruption of brain function, as manifested by at least one of the following: 1) any period of loss of consciousness; 2) any loss of memory for events immediately before or after the accident; 3) any alteration in mental state at the time of accident; and 4) focal neurological deficit(s) that may or may not be transient. (p. 86)
People with mTBI often experience postconcussion syndrome, characterized by a complex set of symptoms that may appear and persist for days, weeks, and even months following brain injury. These secondary symptoms mainly include nausea, confusion, dizziness, blurred vision, headaches, agitation, and mood changes (Centers for Disease Control and Prevention, 2017; National Institute of Neurological Disorders and Stroke, 2018). In addition, people with mTBI may also experience problems in cognitive abilities including memory, attention, executive functioning, and processing speed (Gaetz & Bernstein, 2001; Mathias, Beall, & Bigler, 2004; Mathias & Wheaton, 2007; Tulsky et al., 2017). The availability of a wide spectrum of neuropsychological instruments for assessing these cognitive domains has made it possible to identify and differentiate cognitive impairments associated with moderate and severe TBI (Benedict, 1997; Delis, Kaplan, & Kramer, 2001; Gronwall, 1977; Heaton, Chelune, Talley, Kay, & Curtiss, 1993; Shallice, 1982; Wechsler, Coalson, & Raiford, 2008). However, detecting cognitive profiles associated with mTBI still remains a challenge. There are two potential reasons for this limitation. First, mTBI symptoms may be transient and not appear immediately following the injury, making it difficult to obtain a reliable cognitive profile of the individual with suspected mTBI. Second, cognitive impairments associated with mTBI often show significant variability within an individual and across groups of individuals with a similar mTBI profile, as determined by premorbid cognitive functioning levels, heterogeneity in the etiology of mTBI (e.g., motor vehicle accident vs. a blast exposure during combat), and diffuse neuronal damage. This variability poses limitations to standardizing neuropsychological tests for use in mTBI assessment protocols (Iverson, Holdnack, & Lange, 2013; Prince & Bruhns, 2017; Tulsky et al., 2017).
To address some of the limitations related to existing neuropsychological tests, the National Institutes of Health Toolbox for the Assessment of Neurological and Behavioral Functioning Cognition Battery (NIHTB-CB; Gershon et al., 2013) was tested in a group of 182 individuals with TBI (Tulsky et al., 2017). The authors identified that a small assortment of neuropsychological tests may provide a robust estimate of cognitive functioning in people with TBI, regardless of the severity. These tests included a set of composite scores indexed across multiple measures of various cognitive domains, including memory, attention, and executive functioning. The aim of the study was to establish a construct validity and clinical utility of using NIHTB-CB in people with mTBI. However, three main challenges remain in adapting the toolbox in the evaluation of people with mTBI. First, participants were tested for a total of 8 h over a period of 2 days. This type of test duration poses a serious concern regarding the ecological validity of using this battery of tests in people with mTBI, given that extensive testing may lead to declines in cognitive performance, which may be incorrectly attributed to cognitive impairments. Second, the authors testing NIHTB-CB suspect that the assessment may underestimate cognitive impairment in some domains such as processing speed. Third, the assortment of tests within NIHTB-CB fails to account for previous exposure to similar neuropsychological tests that might have influenced test performance in current testing sessions.
Conventional neuroimaging techniques are designed to identify structural and functional brain changes. Neuroimaging findings of a person with suspected TBI are often linked with neuropsychological data for the purposes of obtaining concurrent validity (Eierud et al., 2014). Some of the common neuroimaging techniques used in the evaluation of moderate to severe TBI are computerized tomography (CT), functional magnetic resonance imaging (fMRI), single photon emission computed tomography, magnetoencephalography, and positron emission tomography. However, these tools may not be sensitive enough to detect the array of microscopic neuroanatomical and subtle neurophysiological changes that occur at the micron and nanometer cellular level in mTBI.
Neuroanatomical changes in mTBI are attributed to the acceleration or deceleration forces that cause diffuse neuronal injury—an important factor that presents additional challenges for injury detection using neuroimaging techniques. While the CT scan has been recommended as the neuroimaging procedure of choice in TBI assessment, repeated exposure to harmful ionizing radiation and difficulties in assessing children and young adults pose additional limitations to wider use of the procedure. Conventional fMRIs in clinical setups such as T-2 and T-1 weighted structural scans index both structural and functional data of neuronal changes following mTBI and pose no health risk to people undergoing the procedures. However, fMRI scans are time-consuming, expensive, and insufficient in providing supplemental information beyond findings obtained from CT scans. Taken together, limitations concerning the lack of sensitivity and specificity at the individual patient level and concerns with ecological validity have presented important challenges to developing mTBI diagnostic tools based on neuroimaging techniques (Bigler, 2004; Eierud et al., 2014; Holmes, Goodacre, Stevenson, Pandor, & Pickering, 2012).
Electrophysiological tests, such as auditory evoked potentials (AEPs), offer hope as potential sensitive assessment tools in identifying the fine-grained neurophysiological changes and diffuse neuroanatomical aberrations accompanying mTBI deficits. The purpose of this review article is to provide an overview of the application of AEPs in the assessment of mTBI and to explore various parameters of AEPs which may have diagnostic value in the assessment of mTBI. To this end, the review covers important AEPs which have shown promise in testing people with mTBI. They include auditory brainstem response (ABR), complex ABR, auditory middle latency response (AMLR), and auditory late latency response (ALLR) subsuming N2 and P300. The review excludes AEPs that were not tested in mTBI, such as mismatch negativity, N-400, P-600, and auditory steady-state response.
AEPs in mTBI Assessment
The most common neurocognitive problems observed in individuals with mTBI are associated with memory, attention, and processing speed (Gaetz & Bernstein, 2001; Mathias et al., 2004; Mathias & Wheaton, 2007). The neural correlates corresponding to these cognitive domains are innately intertwined to the auditory pathway, and efficient auditory processing is contingent upon fast and well-coordinated integration of several neural systems. AEPs have been established as sensitive tools for detecting neural aberrations in the auditory pathway. They offer a precise recording of the synchronicity of neural firing events throughout the auditory nerve, from the cochlea to cortex (Kraus & White-Schwoch, 2015). This level of sensitivity is crucial as it has been shown that the physiological functioning may still be impaired despite normal performance on traditional cognitive assessments in mTBI (Segalowitz, Bernstein, & Lawson, 2001). Thus, we infer that AEPs have the potential to be used as assessment tools, in conjunction with other neuropsychological and neuroimaging tests in obtaining a sophisticated mechanistic picture of neurophysiological and neurocognitive deficits in mTBI. We provide a brief review of the commonly used AEPs and their potential role as assessment tools in mTBI evaluation.
AEPs can be classified into early, middle, and late latency types. Early AEPs include the ABR, elicited using simple and complex auditory stimuli; middle AEPs include the AMLR, and late AEPs include the ALLR or auditory event-related potentials. Early AEPs are used to evaluate the integrity of the cochlea, auditory nerve, and brainstem auditory pathways, while middle AEPs are used to measure auditory cortical functions. Late AEPs are used to evaluate functional brain activity and record changes in information processing due to diffuse axonal injury (Gaetz & Bernstein, 2001).
Early AEPs
Noseworthy, Miller, Murray, and Regan (1981) conducted one of the earlier ABR studies in people with TBI. Participants included 11 people with postconcussion status and 12 matched controls. A significantly delayed latency of Waveform III was recorded in people with postconcussion. These results indicated the involvement of higher neural centers, such as the superior olivary complex (a generating site for Waveform III) in a concussion. In another study, Munjal, Panda, and Pathak (2010) recorded binaural ABRs from 290 participants with TBI (150 with mTBI, 100 with moderate TBI, and 40 with severe TBI) and 50 matched participants with no hearing or neurocognitive problems. ABRs were recorded in both ears separately. GCS was used to classify participants into mild, moderate, and severe TBI groups. The results showed positive associations between the severity of TBI and prolonged Waveform V and I–V interwave latencies in the right ear. The side of impact on the head was not documented in the study, making it difficult to explain differences between the right and left ears in terms of absolute and interwave latencies. In summary, the findings of this study indicate the involvement of the brainstem as a direct consequence of the severity of TBI.
Gallun et al. (2012) studied the efficacy of ABRs in detecting deficits in the cochlear structures and central auditory pathway in 19 military personnel with a history of mTBI following blast exposure and 29 control participants with no history of mTBI. The authors reported no significant differences in the latencies and amplitudes of Waveforms I, III, and V between the blast-exposed and the control group. In some studies, researchers have suggested that ABRs offer no significant prognostic information in the assessment of individuals with mTBI or even with those with severe TBI (Cusumano et al., 1992; Gaetz & Weinberg, 2000; Haglund & Persson, 2009; Keren, Sazbon, Groswasser, & Shmuel, 1994; Nölle, Todt, Seidl, & Ernst, 2004; Werner & Vanderzant, 1991). It should be noted here that such inconsistencies in results across the studies may stem from the variability in time intervals between the brain injury and ABR assessment, as well as the variability in the site of lesion among participants with mTBI (e.g., brainstem vs. cortical lesions; Hall, Speilman, & Gennarelli, 1982; Musiek, Baran, & Shein, 2004).
Another important parameter in ABR acquisition is the rate of stimulus presentation. A high rate ABR protocol is typically used in diagnosing retro-cochlear pathology. Thus, it can be expected that high rate ABRs may have better sensitivity in detecting changes in neural synchrony due to a lesion or injury following mTBI. Podoshin, Ben-David, Fradis, and Pratt (1990) examined ABR recordings in 15 people with minor head trauma and 35 people without a history of brain injury. ABRs were elicited at two different stimulus rates (10/s and 55/s). Follow-up ABR recordings were performed on the same individuals with minor head trauma after 2 months. It was observed that there were no significant differences in interwave latencies V-I, III-I, and V-III at a stimulus rate of 10/s. However, there was a significant delay in all three interwave latencies at a stimulus rate of 55/s, specifically recorded in the first testing session. It can be noted here that an ABR with an increased stimulus rate is sensitive to changes in synaptic efficiency secondary to ischemic changes, while an ABR with a low stimulus rate (e.g., 10/s) is more sensitive to white matter lesions in TBI (Podoshin et al., 1990; Rosahl, Schuhmann, Thomas, Brinker, & Samii, 1998).
Frequency Following Response
ABR recordings typically involve using transient and simple stimuli. However, brainstem responses can also be evoked using complex stimuli with long durations (e.g., speech sounds, music, and amplitude-modulated sounds). Such brainstem responses are also known as complex auditory brainstem responses (cABRs). A cABR waveform consists of an onset response, a frequency following response (FFR), and an offset response. Given that FFR is a crucial component of cABRs, these terms have been used interchangeably as well (Anderson & Kraus, 2013; Skoe & Kraus, 2010). The neural generators of FFRs change with the modulation frequency. The auditory cortex is the primary generator of FFRs at modulation rates ∼40 Hz. FFRs obtained with 70 to 150 Hz modulation frequency reflects sustained phase-locked activity to the individual cycles of the stimulus waveform or the envelope of periodic stimuli in the brainstem (Holmes & Herrmann, 2017; Moushegian, Rupert, & Stillman, 1973; Smith, Marsh, & Brown, 1975). Recently, FFRs have also been used to elucidate deficits in sound processing with extreme granularity (Banai, Nicol, Zecker, & Kraus, 2005; Kraus et al., 2016).
Kraus et al. (2016) showed that FFRs have the potential to be used as an auditory biological marker of concussion in children. The study included 20 children with a history of concussion and 20 children without concussion history. Inclusion criteria for both groups entailed that participants had no history of hearing problems, neurological diseases, or severe TBI. FFRs were recorded from the right ear using a 40 ms sound/d/ delivered through insert earphones at 80.4 dB SPL. The Post-Concussion Symptom Scale was administered to all participants from the concussion group to assess the symptom load. The concept of symptom load refers to the sum total of the intensity of symptoms subsuming neurocognitive, emotional, and somatic domains. The scale included a total of 19 symptoms, with higher scores indicating greater symptom loads. The FFRs of children with concussion exhibited poorer pitch coding and delayed smaller neural responses than children without a history of concussion. The results of the study suggested that neural processing of the auditory stimuli correctly identifies 90% of the concussion and clears 95% of the control population. Thus, it can be construed that FFRs hold the potential to be a reliable biological marker of concussion. However, further studies are required to confirm the validity of FFR markers in different populations with mTBI.
In summary, we infer that early AEPs show potential diagnostic utility in mTBI. Specifically, ABRs with a higher stimulus repetition rate will further augment AEP recordings by indexing synchronicity of neural firing events at a finer level during cognitive performance. The main challenge will be to attenuate the influence of noise during data acquisition resulting from higher stimulus repetition rates (more than 100 stimuli per second). Algorithm-based novel techniques such as continuous loop averaging deconvolution and maximum length sequencing have been used to suppress noise and recover transient AEPs from the data (Peng, Yuan, Chen, Wang, & Ding, 2017). Lastly, investigating the potential influence of different types of auditory stimuli like clicks and tone bursts (frequency specific stimuli) at various presentation rates and levels will offer new insights into understanding deficits in central and peripheral auditory pathways of people with mTBI.
Middle AEPs
AMLR is a middle AEP mainly used for evaluating auditory cortical functions. It is engendered from the medial geniculate body of the thalamus, inferior colliculus, primary auditory cortex, thalamocortical tracts, and lateral supratemporal gyrus (Kraus & McGee, 1990; Musiek, Geurkink, Weider, & Donnelly, 1984). Typically, an AMLR waveform comprises a total of four constituent waveforms: Two negative waveforms labeled Na and Nb and two positive waveforms labeled Pa and Pb/P50. The Pb/P50 waveform of AMLR is the same waveform as P1 of the ALLR. Waveforms of individual AEPs are shown in Figure 1.
Schematic representation of early, middle, and late auditory evoked potentials.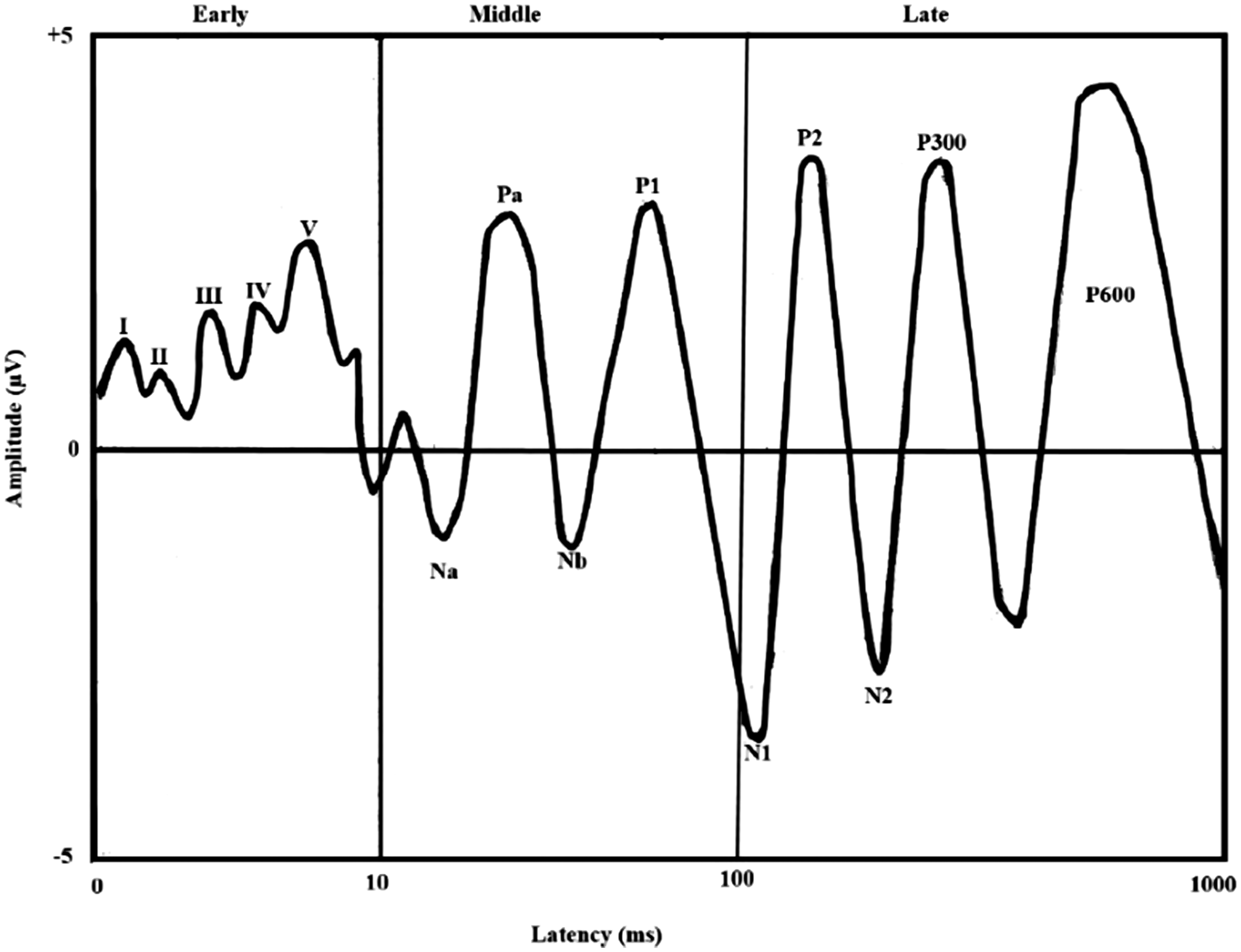
There is evidence to show that AMLR generator regions in the brain may be affected in mTBI, highlighting the diagnostic value of using AMLRs in the evaluation of people with mTBI (Drake, Weate, & Newell, 1996; Soustiel, Hafner, Chistyakov, Barzilai, & Feinsod, 1995). Soustiel et al. (1995) tested 40 participants with mTBI using brainstem AEPs and AMLR. Participants were examined in two sessions: first, 2 days following hospital admission and second, at 3 months following injury. Results showed significantly prolonged Na and Pa waveforms of AMLRs in 15 out of 40 participants. The authors suggested the involvement of diencephalic and paraventricular structures (indexed by abnormal AMLR waveforms) as a plausible pathological basis for some of the postconcussion symptoms, such as memory problems observed in people with mTBI. Drake et al. (1996) studied AMLRs in 20 people with a history of concussion and 20 people without any history of brain trauma. AMLR recordings in people with concussion showed reduced amplitudes of Na and Pa AMLR waveforms and significantly longer Pa latency compared with participants without brain injuries. The authors suggested that amplitude reduction of Na and Pa waveforms may indicate posttraumatic disturbances in subcortical AMLR generators or in frontotemporal cortical structures that modulate them. Further, there is evidence to show that the phenomenon of amplitude reduction of Na and Pa waveforms of AMLRs may be associated with increasing severity of TBI, thus underlining the potential role of AMLRs as one of the main evaluation systems in establishing both the severity of TBI and the associated auditory dysfunction in mTBI assessments (Munjal et al., 2010).
In addition to the Na and Pa waveforms, the AMLR P50 waveform, which is generated from Heschl's gyrus of the temporal lobe, may be crucial in recording neurophysiological events accompanying mTBI (Korzyukov et al., 2007). The P50 waveform has been used as a sensitive measure to evaluate auditory sensory gating—a phenomenon that refers to the inherent ability of the auditory system in preventing incoming irrelevant auditory information from reaching the auditory cortex, thus ensuring relevant auditory processing. It is suspected that persistent attention and memory impairments accompanying TBI may lead to an impaired auditory sensory gating regardless of severity. Therefore, the P50 waveform can be used in obtaining objective and relative measures of auditory sensory gating and record deficits in attention and memory accompanying mTBI (Adler et al., 1998; Boutros, Overall, & Zouridakis, 1991; Judd, McAdams, Budnick, & Braff, 1992). Arciniegas et al. (2000) assessed auditory sensory gating using AMLR on a group of 20 participants with TBI: five with mTBI, six with moderate TBI, and nine with severe TBI. The severity of TBI among participants was defined using the duration of PTA. The AMLR findings of this group were compared with the findings of the nonbrain-injured control group (n = 20). The findings of this study revealed reduced sensory gating in the TBI group when compared with the control group. Interestingly, the mild, moderate, and severe subgroups of this study revealed similar degrees of impaired auditory gating.
In contrast to the earlier findings, two studies have shown no evidence of significant AMLR changes in people with head trauma (Gaetz & Weinberg, 2000; Musiek et al., 2004). We argue that such inconsistencies with respect to AMLR findings among individuals with and without mTBI may be attributed to the differences in the site of lesion (e.g., peripheral vs. central), test protocols, and the time interval between the brain injury and AMLR assessments (Hall et al., 1982; Musiek et al., 2004). Future studies in this line of research will need to address the above confounds when considering AMLRs as a potential tool for assessment of individuals with TBI. At present, the Pb waveform of AMLR holds promise in capturing auditory sensory gating data, which may have imminent application in the assessment and rehabilitation of people with mTBI.
Late AEPs
Generators of Auditory Late Latency Response.

ALLRs are most commonly elicited by auditory two-tone and three-tone oddball tasks. In terms of P3 waveforms, the auditory two-tone oddball task evokes either P3a or P3b, and the auditory three-tone oddball task simultaneously elicits both P3a and P3b waveforms. While P3a is typically elicited by an infrequent and uninstructed novel stimulus, P3b is indexed by an instructed and infrequently presented target stimulus (Polich, 2004, 2007). There is evidence to show that P3a is associated with the efficient allocation of attentional resources to new auditory stimuli (Kopp, Tabeling, Moschner, & Wessel, 2006). On the other hand, P3b is associated with stimulus evaluation and allocation of attentional resources while updating working memory (Broglio, Moore, & Hillman, 2011).
Studies using ALLRs have been at the forefront of electrophysiological research for almost 30 years. Pratap-Chand et al. (1988) compared P3b between 20 participants with mTBI and 20 matched control participants with no history of brain injury. They observed a significant delay in the P3b latency and reduction in P3b amplitude in the postconcussion period in people with mTBI. However, these delays and reductions in latency and amplitude of waveform P3b diminished completely on repeat testing, indicating that P3b is sensitive to cerebral dysfunction in mTBI and the potential recovery phase that may ensue over time. In a similar study, Solbakk et al. (1999) studied information processing and sustained selective auditory attention in participants with MHI, verified frontal lobe damage, and matched controls. They defined MHI as any blow to the head forcing one to stop whatever one was doing. A dichotic listening task was used to index cortical AEPs. The results of this study revealed significantly reduced N2 and P3 amplitudes in participants with MHI compared with participants with frontal lobe damage and nonbrain-damaged controls, reconfirming the notion that people with mTBI have deficits in focused sustained auditory attention and auditory information processing.
Segalowitz et al. (2001) examined the attentional capacity of university students with a history of mTBI (n = 10) and no self-reported neurocognitive impairment (n = 12). The average time postinjury in the mTBI group was 6.4 years. Experimental protocol included administration of four auditory three-tone oddball tasks and neuropsychological tests, such as Wechler Adult Intelligence Scale-Revised (WAIS-R; Wechsler, 1981) and the Woodcock Johnson Psycho-Educational Battery: Tests of Cognitive Ability (Woodcock & Johnson, 1977). In addition, three self-reported questionnaires assessing memory and attention were administered. It was observed that people with mTBI showed significantly reduced amplitudes of P3a and P3b compared with matched controls, while no significant difference was observed in cognitive performance on neuropsychological tests. The results of the study are important for two reasons. First, cognitive problems, especially related to attentional performance, may continue to persist in people with mTBI several years following injury. Second, ALLRs are a sensitive tool that can index cognitive declines that may be missed during routine neuropsychological tests. Similar results of delayed P3 responses have been observed in military veterans with a history of blast exposure, reconfirming earlier evidence on blast-induced mTBI affecting high level auditory and cognitive processing (Eskridge et al., 2012; Folmer et al., 2014; Gallun et al., 2012; McCrea et al., 2009; Papesh, Billing, Folmer, & Gallun, 2016).
In addition to people with experience serving in the military, a relatively higher prevalence of mTBI is observed among athletes, who are vulnerable to sports-related injuries. A range of postconcussion symptoms is commonly found in this population, including slower information processing, impaired focused attention, problems on tasks involving divided attention, and overall inconsistency in cognitive performance (Gosselin, Thériault, Leclerc, Montplaisir, & Lassonde, 2006; Thériault, De Beaumont, Gosselin, Filipinni, & Lassonde, 2009). In a study conducted by Gosselin et al. (2006), ALLR waveforms were examined in 30 athletes that included 20 symptomatic and asymptomatic athletes with a history of concussion and 10 athletes without concussion (controls). The results of the study revealed significantly reduced the amplitude of N1, P2, and P3 waveforms and delayed latency of P3 in both symptomatic and asymptomatic concussed athletes compared with athletes without a history of concussions. In a similar study, Thériault et al. (2009) compared P3a and P3b waveforms in 30 participants, who were recruited from various college sports teams (athletes from football, basketball, and volleyball teams) and divided into three groups: a nonbrain-damaged control group, a recently concussed group (examined between 5 and 12 months after the last concussion), and a late concussed group (examined between 22 and 60 months after the last concussion). A three-tone auditory oddball paradigm was used to record event-related potentials (i.e., P3a and P3b). A neuropsychological battery was also administered to all three groups, which comprised of a symbol digit modality test, a controlled oral word association test, a verbal learning test, a brief visuospatial memory test, a test for visual search and inhibition, and an orientation test. The findings showed a significant amplitude reduction of the P3a and P3b waveforms in the recently concussed group when compared with the nonbrain-damaged control athletes. On the other hand, P3a and P3b amplitudes in the late concussed group were equivalent to the nonbrain-damaged control group. None of the neuropsychological tests showed a significant difference among the three groups. The results indicate that despite functioning within a normal range on neuropsychological tests and sports activities, concussed athletes may still exhibit subtle deficits in auditory information processing within 12 months of head injury, which is identified by sensitive electrophysiological tests like the ALLR.
An Overview of Studies Indexing Auditory Evoked Potentials in Mild Traumatic Brain Injury.

AEP = auditory evoked potential; AMLR = auditory middle latency response; TBI = traumatic brain injury; mTBI = mild traumatic brain injury; ABR = auditory brainstem response; AERPs = auditory event-related potentials; FFR = frequency following response; MHI = mild head injury.
Future Implications
Neurocognitive deficits accompanying mTBI may be transient, subtle, and complex, involving problems with attention, working memory, episodic memory, processing speed, fluid reasoning, and executive functioning (Tulsky et al., 2017). Current limitations of neuropsychological and neuroimaging assessment tools may result in an underdiagnosis of mTBI, leading to challenges in acute management, long-term recovery, and rehabilitation for people with mTBI. These limitations can be addressed to some extent by including AEPs in the standard test battery of assessment tests in mTBI. The inclusion of AEPs in a standard test battery is suggested because AEPs are not an independent diagnostic tool for mTBI and have certain limitations such as targeting only auditory sense modality and providing less spatial or localizing information than neuroimaging tests. In addition, the clinical usefulness of AEPs in the assessment of mTBI is limited by the lack of standardized experimental paradigms. Nevertheless, various waveforms of AEPs offer a promising assessment protocol as a simultaneous or supplemental tool in recording accompanying neural events in conjunction with other neuroimaging tests in mTBI. The range of neurocognitive deficits observed in people with mTBI may also be a result of problems in the processing of auditory information itself (since cognitive and auditory domains are interrelated in tasks of information processing, as in auditory comprehension). However, it is likely that deficits resulting from mTBI may encompass both neurocognitive and auditory domains, depending on the site and the extent of neurotrauma. AEPs offer a highly sensitive index to measure potential auditory deficits in mTBI, thus providing enhanced information for making clinical decisions. The high rate ABR is sensitive to changes in synaptic efficiency, secondary to ischemic changes, and may identify subtle synaptic impairment associated with mTBI (Podoshin et al., 1990). The sensitivity of high rate ABRs could be enhanced by manipulating stimulus parameters and incorporating newer techniques like maximum length sequencing and continuous loop averaging deconvolution. Future studies are warranted to identify the influence of these techniques in the detection of deficits in patients with mTBI. The attention and memory deficits in mTBI patients could be associated with impaired sensory gating. The P50 waveform of the AMLR is a sensitive parameter to identify sensory gating deficits in participants with mTBI (Arciniegas et al., 2000). The clinical potential of P50 needs to be explored in future studies. A recent study examined the processing of fundamental frequency using FFRs in children with concussions and suggested that FFRs could be used as a biological marker for sports-related concussions (Kraus et al., 2016). There is a need to validate FFRs in different types of mTBI populations. The P3 waveform and its subtypes, P3a and P3b, are viable tools for investigating the integrity of sensory pathways, including their efficiency for conducting auditory inputs and the covert aspects of information processing, auditory memory, and auditory attention (Eierud et al., 2014). Despite the efficacy of P3, it is not used widely or routinely in general clinical neurology. One of the major barriers in clinical utility of all these promising AEP waveforms in mTBI assessment is a lack of standard testing paradigms. The development of standard testing paradigms for high rate ABR, FFR, P50, and P3 waveforms is the next step in considering AEPs as a clinical tool in mTBI assessment protocols.
Conclusions
Structural and functional brain changes following mTBI entail both acute and long-term neurocognitive implications, regardless of the etiopathology and the extent of the neuronal injury. Conventional neuropsychological tests and neuroimaging techniques may not be sensitive or specific enough in delineating varied cognitive deficits and neural correlates underlying these deficits. AEPs are cost-effective, easily accessible at most clinical care centers, and sensitive to indexing neural events accompanying performance on cognitive tasks. Including AEPs as part of the standard assessment tools will provide concurrent validity by offering triangulation of data from neuroimaging and neuropsychological tests, resulting in better diagnostic outcomes for people with mTBI. This step will be crucial in performing comprehensive evaluations of neurocognitive profiles of people with mTBI for meeting acute management and rehabilitation goals as well as identifying predictors for mTBI recovery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.