
Abstract
Objective
In this retrospective case series, we chronicle six patients presenting with acute suppurative thyroiditis (AST) with progression to thyroid abscess in a single institution.
Methods
Patients ranged in age from 16 to 74 years of age. The most common presenting symptoms were progressive unilateral neck pain, swelling, and odynophagia. Other symptoms included hoarseness and systemic signs of infection. Diagnosis of thyroid abscess was made with a CT scan of the neck, fine needle aspiration, and/or incision and drainage (I&D).
Results
Management included antibiotic therapy, I&D, and thyroidectomy. All patients were successfully treated except for one who developed mediastinitis and died.
Conclusion
A complete literature review was performed to determine etiologies, common findings, and management of similar cases.
Introduction
Acute suppurative thyroiditis (AST) is a rare but potentially life-threatening condition. Well-protected from infection, the thyroid gland has a fibrous capsule and fascial planes separating it from other neck structures and shielding it from local spread of pathogens.1,2 The thyroid gland has an extensive vascular supply and lymphatic drainage, which further protects it from infection. The gland’s high iodine content also inhibits microbial growth. Due to these protective factors, AST accounts for <1% of thyroid disease. 2 AST has a mortality rate that is estimated to be 12% or more without adequate treatment.3,4 The disease typically presents as acute onset of painful anterior neck swelling and fever. The etiology of AST is most commonly gram-positive bacteria such as Staphylococcus aureus, although gram-negative associated infections have been documented. 2 Early diagnosis and treatment is vital to prevent complications such as thyroid storm,5,6 airway compromise,5,7 internal jugular vein (IJV) thrombosis,5,8 and sepsis.5,9 Therefore, thyroid abscesses should be considered part of the differential in any patient with anterior neck swelling. Diagnosis can be made with ultrasound, CT imaging, fine needle aspiration (FNA), or incision and drainage (I&D). 10 Surgical drainage and systemic antibiotics are the mainstay of treatment for AST.
Due to the rarity of this pathology, case reports and case series are frequently used to guide treatment. A total of six patients were identified in this case series, and their unique presentations and clinical courses are described.
Methods
This study is a retrospective review of patients with a thyroid abscess in a multi-centered single institution from January 2005 to November 2021. Exemption from the Institutional Review Board at Geisinger Health System in Danville, PA was obtained.
Results
Case 1
A 50-year-old woman presented 2 weeks after bariatric surgery with left-sided neck pain, otalgia, odynophagia, and hoarseness. She was prescribed clindamycin and referred to otolaryngology. Two days later, she presented to the emergency department with worsening symptoms. White blood cell count (WBC) was 13.47 K/μL and a CT neck with contrast demonstrated a left-sided 4 × 2 cm intrathyroidal abscess without compression of the trachea (Figure 1A). She had no history of thyroid nodules, cancer, or other head and neck pathology. Ultrasound-guided aspiration was the initial treatment recommendation. Ten ml of thick purulent fluid was aspirated, with culture growing Streptococcus anginosus. The patient experienced improvement of symptoms following needle aspiration and was discharged with a 1-week course of Augmentin. (A) CT neck with contrast, axial view, demonstrating left-sided 4 × 2 cm intrathyroidal abscess without external compression or deviation of the trachea. (B) CT neck with contrast, axial view, demonstrating persistent thyroid abscess.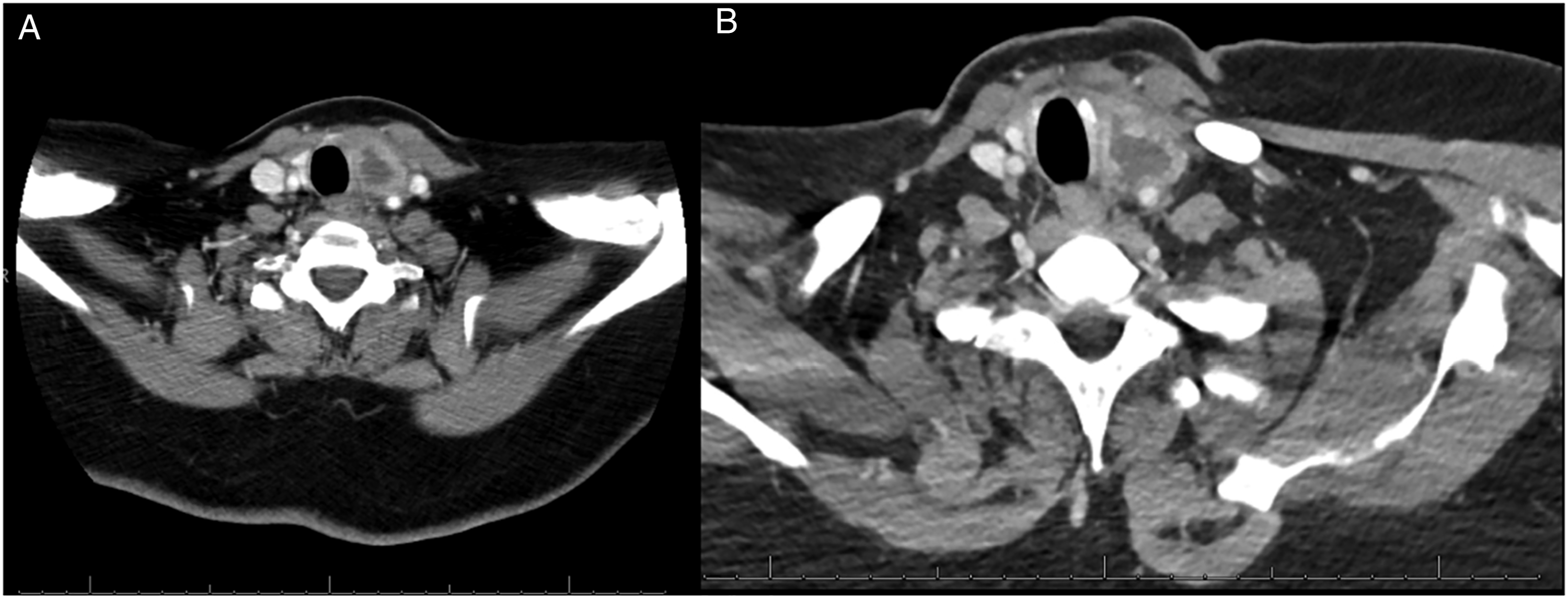
Eight days after discharge, the patient presented with worsening neck swelling and evidence of recollection on CT (Figure 1B). A repeat US-guided aspiration was performed, and she was admitted for IV antibiotic therapy. Barium swallow showed no evidence of a fistula but showed effacement of the left piriform sinus. She then underwent direct laryngoscopy (DL) and neck exploration, with I&D of the abscess. DL did not reveal signs of a sinus tract or fistula; however, significant inflammation was encountered during exploration of the neck. Surgery was limited to an I&D as thyroidectomy was felt to be unsafe. She was discharged on Augmentin for 10 days, with reported improvement of dysphagia and resolution of odynophagia at the 2-week follow-up.
Case 2
A 46-year-old woman presented with dysphagia and right-sided neck pain and swelling 4 weeks after FNA of a 4.8 cm benign right thyroid nodule. The patient had a WBC of 11.2 K/μL, and the right thyroid lobe was enlarged and tender to palpation on physical exam (Figure 2A). CT neck demonstrated a 7.6 cm, partially cystic right thyroid mass, with associated mass effect on surrounding structures (Figure 2B-D). The patient elected for surgical treatment rather than aspiration of fluid. (A) Gross appearance of right-sided anterior neck swelling. (B) Ultrasound of neck demonstrating enlargement of the right thyroid nodule to 7.6 cm. (C) CT Neck with contrast, axial view, demonstrating large, complex, partially cystic mass arising from the right thyroid lobe, measuring approximately 5.8 × 6.5 × 7.1 cm, with mass effect on the surrounding structures causing leftward deviation of the trachea without obstruction. (D) CT Neck with contrast, coronal view, demonstrating same.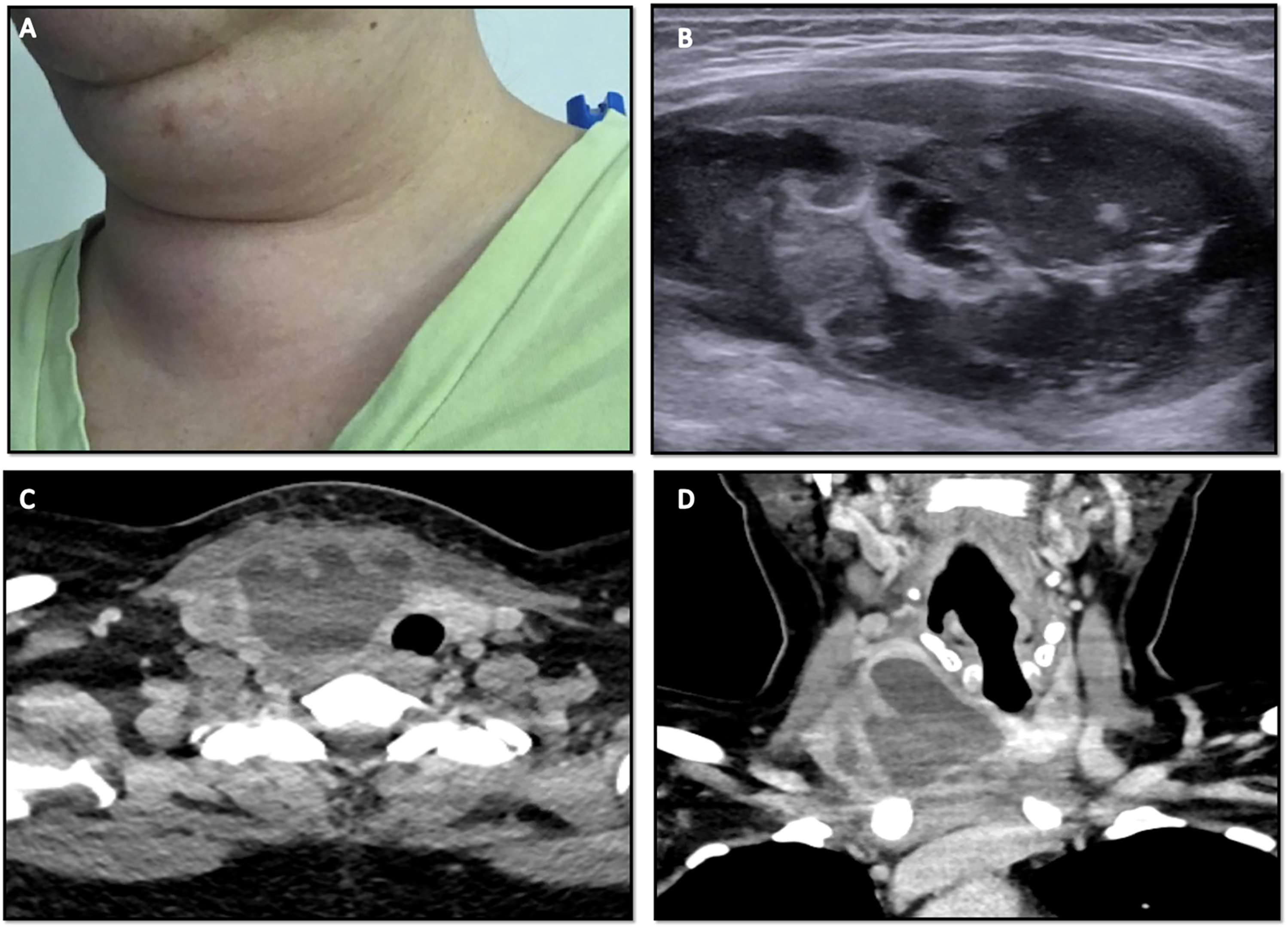
Right subtotal thyroidectomy was completed with extensive perithyroidal inflammatory changes noted. Multiple Staphylococcus species and Propionibacterium acnes grew in the culture. Surgical pathology was consistent with an acute infectious process, without signs of a branchial cleft anomaly. The patient reported immediate improvement in symptoms of neck fullness, pain, and dysphagia. She was discharged home on postoperative day one with a 2-week course of Augmentin and had no further symptoms.
Case 3
A 67-year-old woman presented to the emergency department with a 3-month history of an enlarging anterior neck mass, progressively worsening dysphagia, hoarseness, and twenty pounds of unintentional weight loss. She had a history of thyroid goiter. On presentation, the patient had a WBC of 9.8 K/μL and was found to have a urinary tract infection, with urine cultures growing E coli (>100 000 cfu/mL). On exam, there was a large mildly tender and indurated anterior neck swelling with substernal extension. Flexible nasopharyngolaryngoscopy revealed immobility of the left vocal fold. CT neck demonstrated an 8.7 × 6.9 × 8.4 cm heterogeneously enhancing cystic thyroid mass that extended substernally with significant rightward tracheal deviation (Figure 3A and B). (A) CT neck with contrast, axial view, demonstrating large left heterogeneous enhancing cystic thyroid mass with foci of air, compatible with an abscess. (B) CT neck with contrast, coronal view, large left thyroid abscess with substernal extension and significant deviation of trachea. (C) Large nodular thyroid goiter with intrathyroidal necrotic abscess cavity. (D) Cross-section of intrathyroidal abscess cavity.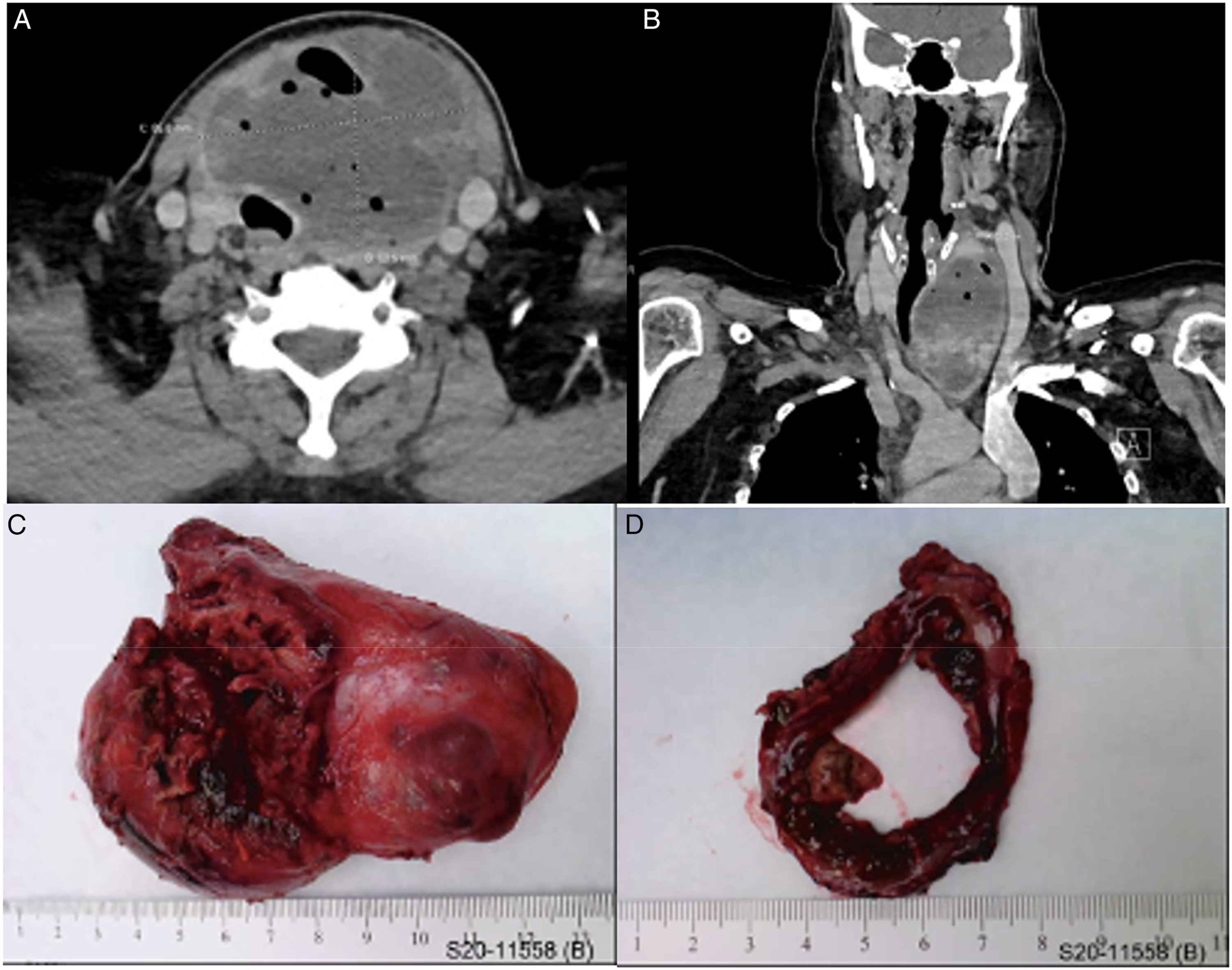
FNA was consistent with an abscess, with cultures growing E coli. The patient subsequently underwent a total thyroidectomy (Figure 3C and D). Final pathology was consistent with an abscess, with necrotic tissue and nodular goiter, but no evidence of malignancy or branchial cleft anomaly. She was treated with ceftriaxone initially and transitioned to Bactrim at discharge. The patient reported significant improvement in her swallowing and voice function during hospitalization. On postoperative day five, repeat flexible nasopharyngolaryngoscopy demonstrated return of left vocal fold mobility. The patient remained asymptomatic at one month, with no recurrent neck infections.
Case 4
A 16-year-old boy presented to the emergency department with right neck swelling, fever of 102 F, and nausea for one day. On exam, a 3 × 3 × 3 cm mass was noted at the base of the right sternocleidomastoid muscle. Laboratory evaluation revealed an elevated WBC count of 13.37 K/μL, and CT neck showed a 3.2 × 2.6 cm cystic mass of the right inferior thyroid (Figure 4). The patient was prescribed a 10-day course of Augmentin and scheduled to follow-up with Otolaryngology. He denied any improvement in symptoms during a follow-up appointment 2 days later. Examination revealed enlarged thyroid gland with tenderness to palpation and no signs of overlying cellulitis. Flexible nasopharyngolaryngoscopy was unremarkable and no lesions within the pyriform sinuses were identified. Aspiration of the suspected abscess was completed, yielding 7 mL of thick, brown fluid from the right thyroid gland. Pathology revealed numerous neutrophils consistent with AST and gram stain showed intracellular gram-positive cocci within the neutrophils. The patient completed the course of oral antibiotics and had complete resolution of symptoms. CT Neck with contrast, axial view, demonstrating a 3.2 × 2.6 cm cystic mass of the right inferior thyroid gland.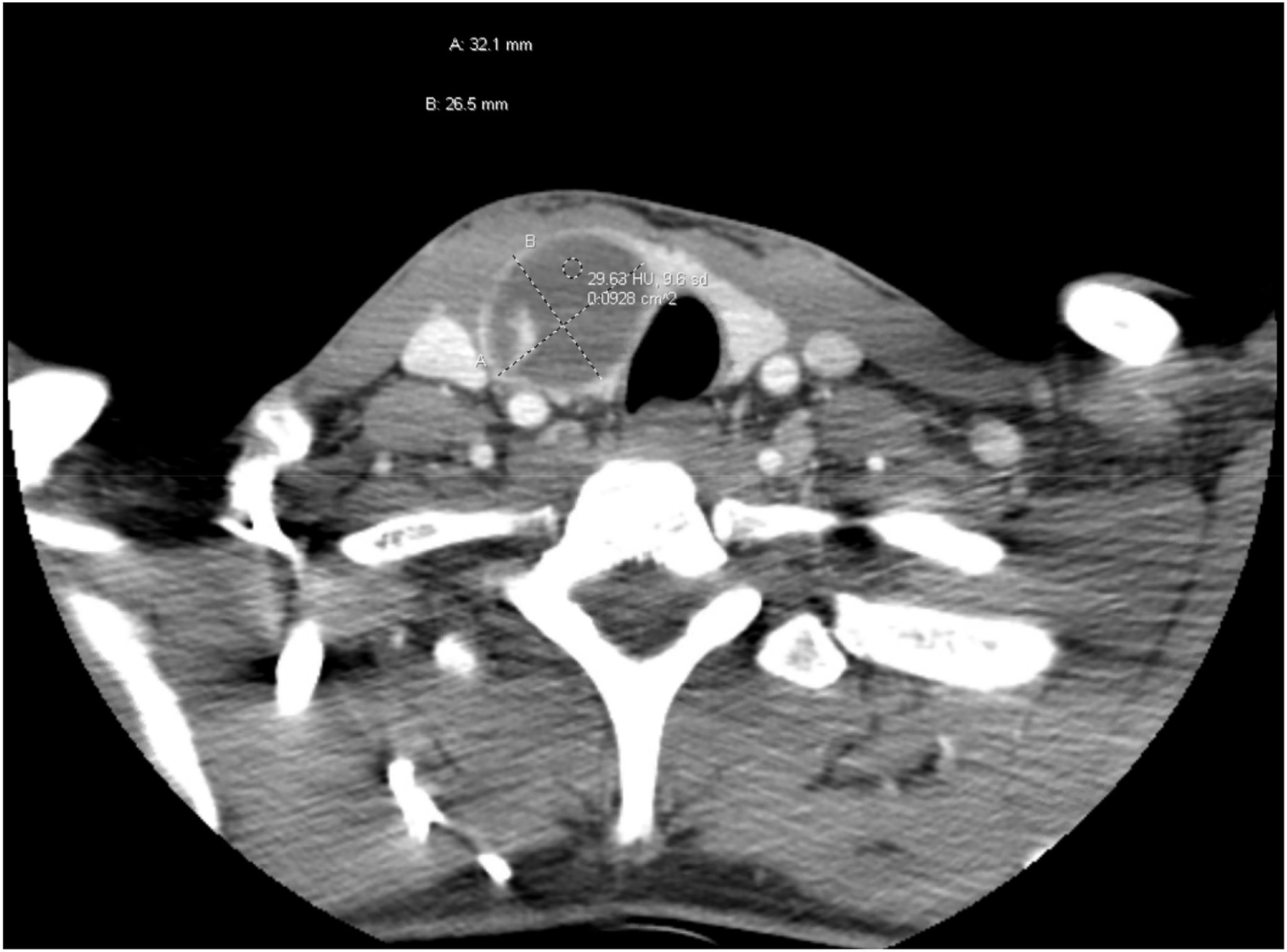
Case 5
A 16-year-old girl presented to the ENT clinic with a 1-week history of sore throat and painful left neck swelling. Because of a known left thyroid nodule, and family history of papillary thyroid carcinoma, a left hemithyroidectomy was recommended. The patient presented on postoperative day 3 with concerns for surgical site infection. Forty ml of purulent material was drained from the neck, confirming a postoperative abscess. She was admitted and treated with intravenous (IV) clindamycin and local wound care. Her symptoms improved and she was discharged on a 10-day course of oral clindamycin with local wound care. After a prolonged course of wound care, the patient’s incision ultimately healed.
Approximately 18 months after the thyroidectomy, the patient re-presented with anterior neck tenderness, and a deep neck abscess was identified (Figure 5). The patient underwent I&D of the abscess, utilizing the prior thyroidectomy incision. At this point, there was high suspicion for a fourth branchial cleft anomaly. Direct laryngoscopy and esophagoscopy was performed, which revealed a dehiscence in the piriform recess. At the same time, the patient underwent pharyngoplasty and obliteration of a fourth branchial cleft cyst. Unfortunately, the patient continued to develop recurrent neck abscesses requiring multiple I&D’s. Ultimately, a limited pharyngectomy was performed due to inability to close the pharyngeal fistula. Following this, the patient has not had any further neck abscesses. CT Neck with contrast, axial view, demonstrating 5.4 × 5.3 × 5.0 cm fluid and air containing rim-enhancing collection in the left anterior soft tissues, extending from the residual left thyroid lobe to the sternoclavicular notch with a tract extending to the skin anteriorly.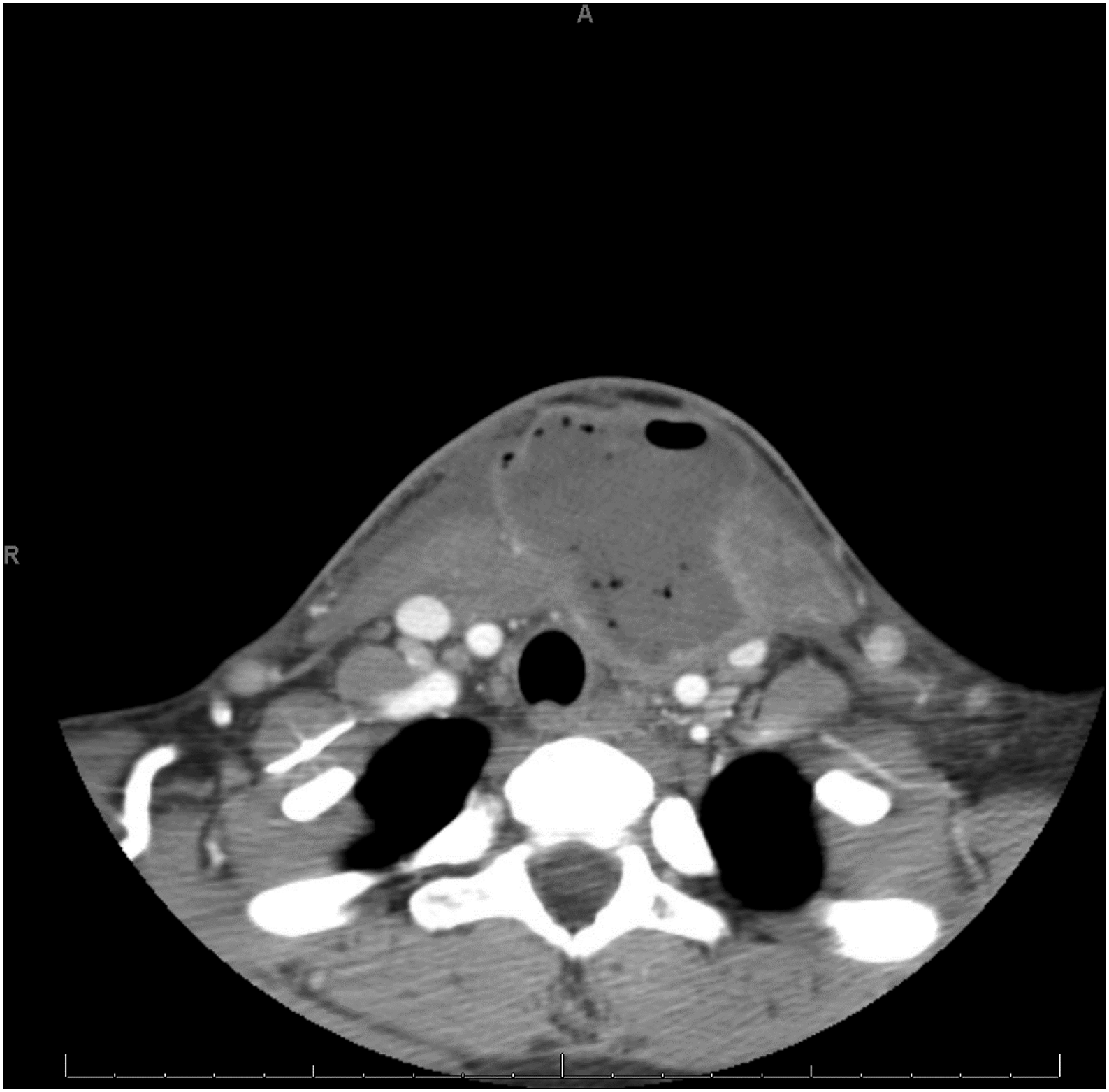
Case 6
A 74-year-old man presented to the emergency room with a 2-day history of progressive odynophagia and throat pain. Thorough examination revealed a temperature of 100.7 F, WBC 24.19 K/μL, thyroid tenderness on palpation, and asymmetric tonsils. CT neck was consistent with an abscess that appeared to originate in the thyroid and extend into the parapharyngeal space and downward into the mediastinum. The patient underwent I&D of the parapharyngeal component of the collection and was admitted to the hospital for IV antibiotics. He initially had improvement in his symptoms. However, after 2 days of conservative management, the patient began to deteriorate clinically. Repeat CT neck revealed progression of the underlying infection with pericardial involvement. I&D of the neck was performed with an isthmectomy, revealing necrosis with abscess. Despite source control, the neck infection continued to progress in the chest, leading to empyema. The patient underwent right thoracotomy with pulmonary decortication and mediastinotomy. Unfortunately, the mediastinal and chest disease were unable to be controlled and the patient expired on hospital day 29.
Discussion
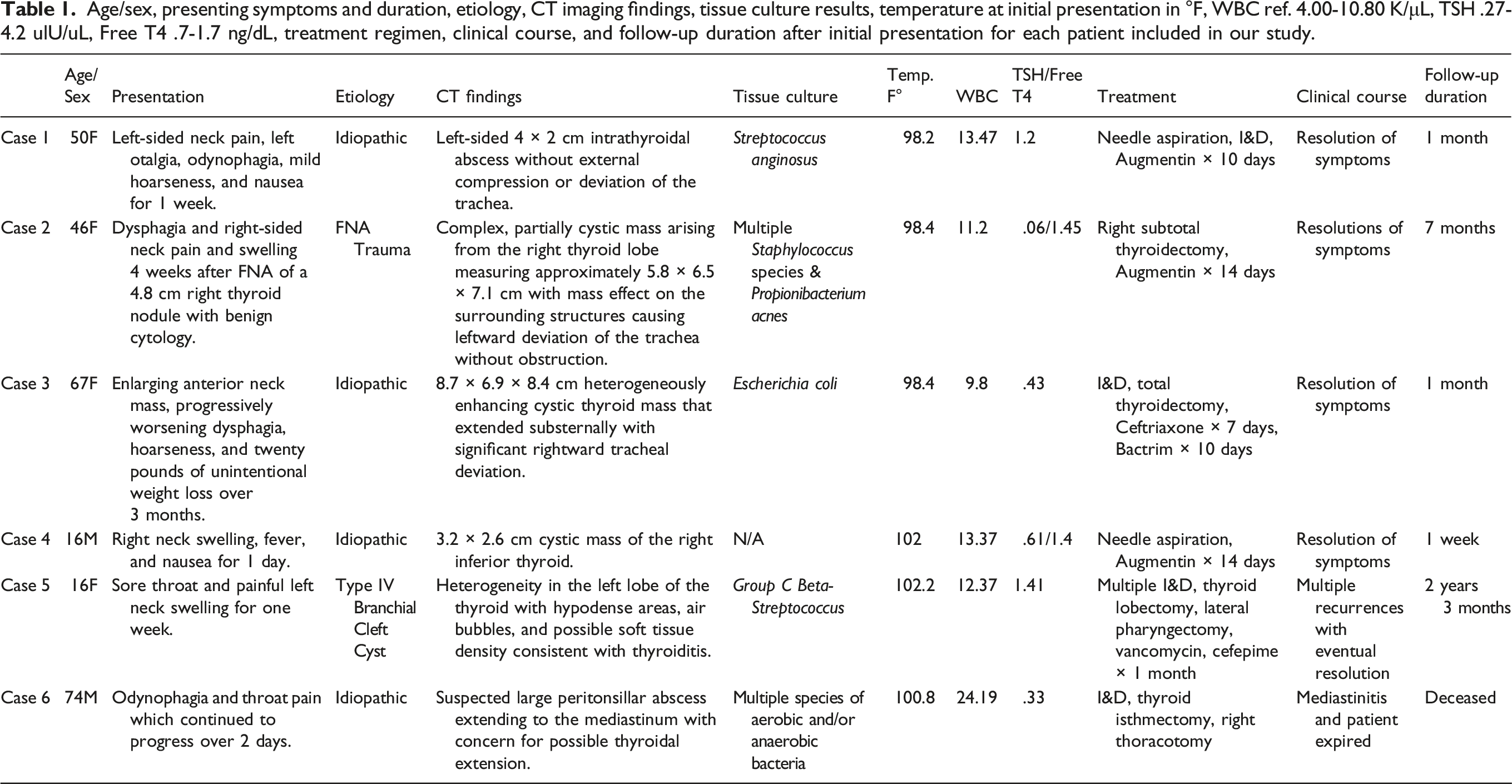
Age/sex, presenting symptoms and duration, etiology, CT imaging findings, tissue culture results, temperature at initial presentation in °F, WBC ref. 4.00-10.80 K/μL, TSH .27-4.2 ulU/uL, Free T4 .7-1.7 ng/dL, treatment regimen, clinical course, and follow-up duration after initial presentation for each patient included in our study.
Staphylococcus and Streptococcus species account for 35–40% of infections; gram-negative species account for 25% of infections; anaerobes account for 9–12% of infections; and the remaining infections have a fungal etiology.1,12 Salmonella, Eikonella, and Tuberculous infections of the thyroid gland have also been reported, with salmonella infections occurring more frequently in immunocompromised patients.13-18 Yu et al 4 performed a review of 191 patients with thyroid abscesses from 1980 to 1997 and reported approximately 50% of patients with AST to be immunocompromised as a result of conditions such as HIV and malignancy. 4 They also report that 70% of their patients had an anatomical anomaly. In contrast, Jeng et al 19 reported that only 1 out of 10 patients with AST presented with an anatomical defect, most commonly pyriform sinus fistula. 19 In this case series, one patient had a history of renal cell carcinoma, classifying them as immunocompromised according to Yu’s classification, and one patient had a branchial cleft cyst.
Congenital anatomical anomalies should always be considered in patients with thyroid abscesses regardless of age. 20 In this series, based on imaging and history, only one case was felt to be associated with a congenital abnormality. This was an unusual case of a young woman with recurrent thyroid abscesses secondary to a type IV branchial cleft cyst. The branchial cleft cyst was masquerading as thyroid pathology, and her recurrent infections were only controlled after a lateral partial pharyngectomy was performed. Sinus tracts between the pyriform sinus and thyroid gland were described by Paes et al 12 AST due to pyriform sinus fistula was found in 135/139 cases described in a review by Miyauchi. 21 As seen in our patient, left thyroid lobe involvement is associated with pyriform sinus fistula. 22 Kruijff et al 20 reported five patients, aged 9–41 years old, presenting with a left-sided thyroid abscess due to third or fourth left branchial cleft anomalies. 20 Management of patients in their study included lobectomy as was used in treatment of our patient with branchial cleft anomaly. However, due to recurrent infections in one patient in this series, definitive treatment with a limited pharyngectomy was required.
Iatrogenic and idiopathic cases of AST were identified in this case series. Patient 2 presented with a thyroid abscess following FNA of the thyroid nodule. Other cases of iatrogenic AST have also been described, and self-induced thyroid abscesses have been reported from patients self-injecting heroin into the thyroid gland.23,24 There are reports of idiopathic thyroid abscesses, but an idiopathic thyroid abscess continues to be a rare phenomenon.4,6 Interestingly, four patients in this case series had idiopathic AST. While it is essential to identify risk factors for AST, a high degree of suspicion needs to be maintained in any patient who presents clinically with neck swelling, pain, and associated fever.
Diagnosing patients with AST utilizes laboratory assessment but relies largely on imaging modalities. Ultrasound is the preferred imaging modality for the thyroid gland. When diagnosing thyroid abscesses, however, CT neck with contrast is an invaluable tool to identify the abscess and potential anatomic anomalies. Basic laboratory values include white blood cell count, c-reactive protein, sedimentation rate, complete metabolic panel, thyroid stimulating hormone, and free thyroxine. Of note, thyroid labs have not proven to be useful in the diagnosis or management of these patients. 4 Surgical drainage and concurrent antibiotic therapy were the mainstay of treatment in these patients. This approach is the most utilized treatment paradigm described in the literature on thyroid abscesses.
Other approaches have also been described. Halenka reports success in conservative treatment with US-guided fine needle evacuation and sclerotization with absolute alcohol, in addition to targeted antibiotics.1,25 Paes et al 12 noted a trend towards less invasive treatment during acute inflammation and infection. 12 Incision and drainage may also be repeated if the abscess reaccumulates. Ultimately, hemithyroidectomy or total thyroidectomy may be performed in severe cases, especially if patients are refractory to antibiotics and drainage.26-28 Delaying removal of thyroid tissue until more conservative approaches have been exhausted is recommended due to risk to parathyroid glands and recurrent laryngeal nerves, which can be particularly difficult to identify and protect in the setting of thyroiditis.
Potential complications of a thyroid abscess are numerous and may include death. Cases of thyrotoxicosis associated with thyroid abscess are present in the literature.5,6 These patients presented with symptoms of thyroid storm, which responded to surgical drainage of the abscess and systemic antibiotics. In addition to thyrotoxicosis, the case report by Fonseca et al 5 had extension of the right thyroid lobe abscess into the thorax introitus, causing tracheal deviation and large vessel compression leading to IJV thrombosis and sepsis. 5 Neck abscesses are a known cause of IJV thrombosis. 8 Deshmukh et al 7 reported a stridorous patient who was ultimately found to have tracheal compression due to a thyroid abscess. 7 Sepsis may be a complication of thyroid abscess, as well as the etiology.5,9 Jain et al. report a case of an E coli thyroid abscess following urosepsis in a patient with a history of goiter. Morbidity of thyroid abscess may be significant, and this emphasizes the importance of prompt diagnosis and treatment.
This study is limited by its retrospective nature. Patients were identified and included in the review because they were known to the otolaryngology service. We did not include patients who were not treated by the otolaryngology department, thereby excluding other possible cases within our institution. Strengths of our study include a relatively large number of cases; diversity in age, presentation, and outcomes; and treatment by a single department.
Conclusion
We present six cases of thyroid abscess with varied etiologies and disease courses. The etiology of thyroid abscesses is occasionally iatrogenic or due to congenital anatomic anomalies, but they are frequently idiopathic. A high degree of suspicion should be maintained in patients presenting with anterior neck pain and swelling. Early diagnosis and treatment with abscess drainage and systemic antibiotics are vital to ensuring good outcomes in this potentially fatal, rare condition.
Footnotes
Authors’ note
This published research complies with internationally-accepted standards for research practice and reporting.
Author contributions
Writing/drafting the manuscript, Final approval: Randy Lesh, Ryan Hellums, DO, Priscilla Pichardo, DO, Jeff Wong, MD; Critical revision/editing, Final approval: Phillip Pellitteri, DO, Nicholas Purdy, DO, Kevin Stavrides, MD, Thorsen Haugen, MD.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval is not required for this study in accordance with local or national guidelines.
Informed consent
Written informed consent was obtained from the patient for publication of the details of their medical case and any accompanying images.
Data availability
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.