
Abstract
Objectives:
To determine whether thyroidectomy improves quality of life in patients with Hashimoto thyroiditis with persistent symptoms despite biochemical euthyroidism.
Methods:
A retrospective cohort study was conducted of patients undergoing thyroidectomy for Hashimoto thyroiditis at our institution between 2014 and 2018. The following variables were collected: age, race, body mass index, preoperative symptoms, preoperative thyroid peroxidase antibody titer, thyroglobulin antibody titer, thyroid-stimulating hormone, free thyroxine, specimen weight, and histologic presence of thyroiditis. Outcomes included general health score on the Short Form 36 (SF-36) Health and responses to a questionnaire addressing postoperative disease management.
Results:
A total of 19 patients were included in the study, 18 of whom were female with a mean age of 48 years. The majority of patients were Caucasian. There were no significant differences between the postoperative general health scores of the patients with Hashimoto thyroiditis and scores from a healthy control population (66.9 vs 74.1; 95% CI: −16.9 to +2.5, P = .16). There were also no differences between groups within the 7 SF-36 subscores. Elevation in preoperative thyroperoxidase antibody correlated with lower reported postoperative energy levels (r = −0.63, P = .016) and emotional well-being (r = −.55, P = .041); 87.5% of respondents reported being moderately or extremely happy with their decision to proceed with surgery.
Conclusions:
Quality of life in patients with Hashimoto thyroiditis who undergo thyroidectomy is equivalent to the general population, and the majority are satisfied with surgery. Thyroidectomy is a consideration for patients with persistent symptoms despite optimization on medical therapy.
Introduction
Hashimoto thyroiditis (HT), a type of chronic lymphocytic thyroiditis, is the most common autoimmune thyroid condition, and its frequency has been increasing in recent decades. 1 Although the pathogenesis is not entirely understood, the development of an immune response against the thyroid has been shown to result from the interaction between genetic susceptibility and environmental factors. 2 Histologically, the disease is characterized by an extensive lymphocytic infiltrate in the thyroid and follicular atrophy with increased fibrosis. Ultimately, replacement and damage of the thyroid parenchyma lead to hypothyroidism and gradual atrophy of the gland. 3 The diagnosis is primarily made on the basis of serum autoantibodies against thyroperoxidase and/or thyroglobulin, which may precede clinical symptoms and biochemical hypothyroidism by several years. 4
The standard approach to disease management and hypothyroidism is the medical optimization of thyroid hormone supplementation. However, a subset of patients continue to report symptoms despite biochemical euthyroid status. 5 It has been surmised that symptoms may result from the inadequacy of levothyroxine in hormone substitution or is related to the intensity of the autoimmune response as measured by elevated thyroid peroxidase antibody (TPO Ab).6,7 To date, there is no algorithm for treatment in these refractory cases. Given the known challenge of thyroidectomy in patients with HT, surgery has typically been reserved for cases of concomitant malignancy or substernal goiter with compressive symptoms.8,9 Recent clinical trial data, however, have shown that thyroidectomy may be a beneficial option in patients with persistent symptoms and extremely elevated TPO Ab levels. 10 In the current study, we present health-related and disease-specific quality of life outcomes in patients with HT undergoing thyroidectomy specifically for persistent symptoms.
Patients and Methods
This retrospective cohort study was approved by Stanford’s Institutional Review Board and Research Compliance Office. Eligible patients were extracted from our institution’s electronic medical record with the help of Stanford Research Repository. Patients were initially identified based on International Classification of Disease (ICD) 9 and Current Procedures Terminology codes for having undergone thyroidectomy at Stanford Hospital between 2014 and 2018. Operations were carried out by the senior author in the Department of Otolaryngology, Head & Neck Surgery. The indication for thyroidectomy in all cases was refractory symptoms. Patients older than 18 years who either had elevated preoperative TPO Ab titers and/or postoperative evidence of lymphocytic thyroiditis on pathology reports were included in the study. Thyroid-stimulating hormone (TSH) levels were between 0.1 and 3.5 mIU/L with hormone supplementation. Patients reported persistent difficulties with fatigue, lack of energy, bodily pain, memory/concentration impairment, or mood fluctuation despite normal or mildly suppressed TSH and normal free thyroxine (T4) while on thyroid hormone supplementation. Those with known malignancy preoperatively, suboptimal medical management with persistent biochemical hypothyroidism, incidental or asymptomatic HT, and surgery within less than 3 months were excluded.
The following demographic, medical, and biochemical variables were collected: age, gender, race, body mass index (BMI), length of diagnosis, preoperative TPO Ab and thyroglobulin antibody (Tg Ab), preoperative TSH and free T4, and specimen weight. Pathology reports were reviewed for presence of thyroiditis or occult malignancy. The primary outcome was health score on the Short Form-36 Health Survey (SF-36). The SF-36 is made up of 36 questions and scored from 0 to 100, with higher scores being associated with more well-being, in 8 subcategories: general health, physical functioning, role physical, bodily pain, vitality, social functioning, role emotional, and mental health. Scores from survey data completed a minimum of 3 months postoperatively were compared with normative data from women between 35 and 54 years. This was deemed the most appropriate comparative population as there was only 1 male respondent in this study. All patients had achieved biochemical euthyroid status before embarking on surveys. Secondary outcomes included an additional questionnaire specifically addressing disease management after surgery, which is shown in Figure 1. Surveys were distributed and responses collected electronically. Adverse surgical outcomes were also recorded. Data were analyzed using SAS 9.4 (SAS Institute).
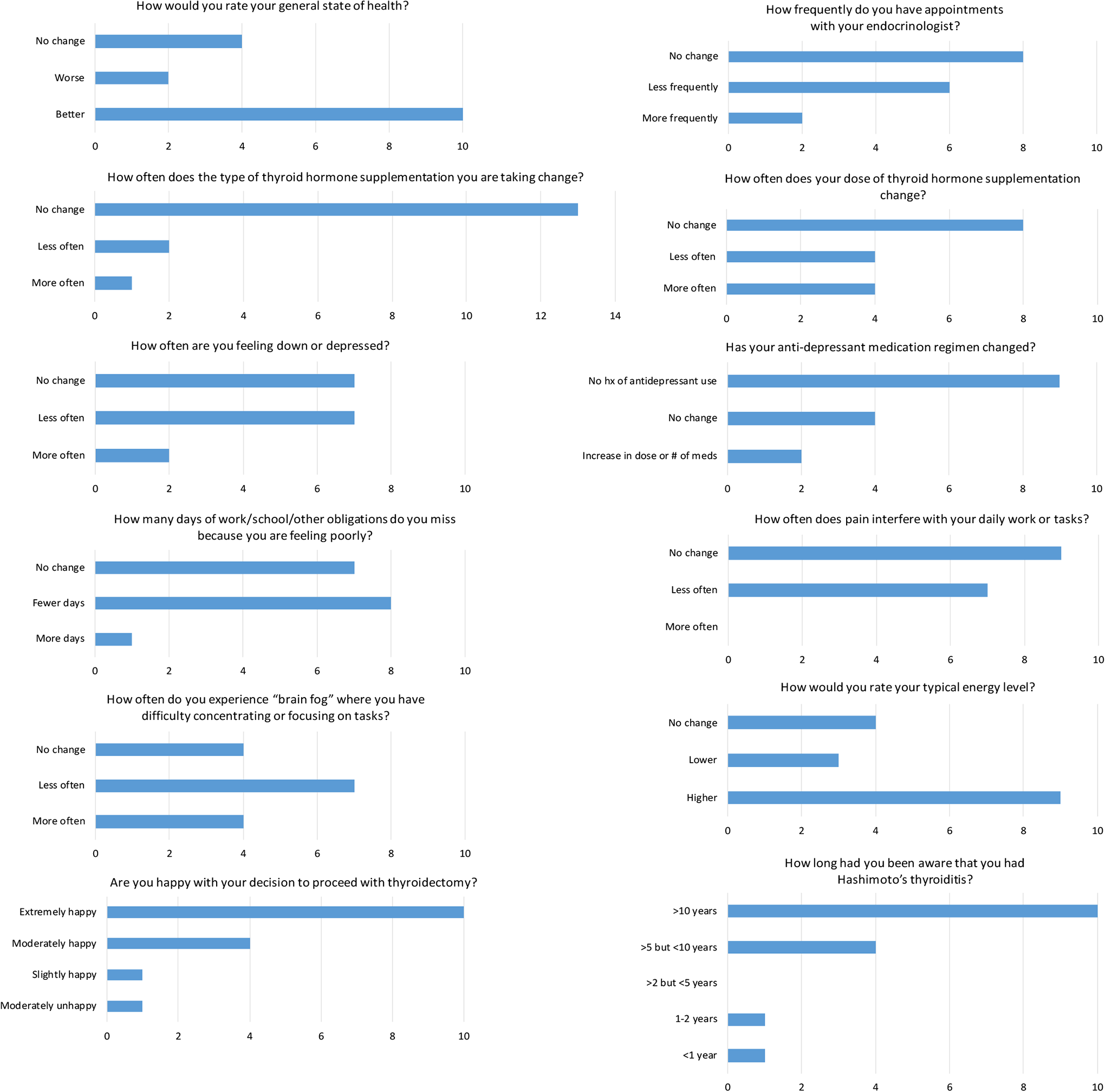
Secondary survey with summary of patient responses.
Results
Patient Characteristics
Chart review yielded 45 patients meeting criteria who had undergone thyroidectomy for management of Hashimoto disease ranging between 3 and 35 months prior. Surveys were distributed to all 45 patients electronically and were completed and returned by 19 (response rate 42%). The remaining patients did not respond to the survey invitations. Of the 19 patients, 18 were female with an average age of 48 years and average preoperative BMI of 27.5. The majority of patients were Caucasian. At the time of surgery, 1 patient had been aware of the diagnosis of HT less than 1 year, 1 patient between 1 and 2 years, 5 patients between 5 and 10 years, and 9 greater than 10 years. Average TSH was 0.23 mIU/L and free T4 was 1.42 ng/dL. Average preoperative TPO Ab was 260 IU/mL and Tg Ab was 207.9 IU/mL. In final pathologic evaluation, 17 specimens showed characteristic changes of Hashimoto disease with lymphocytic infiltration, and 2 specimens harbored clinically occult papillary thyroid carcinoma. Demographic, biochemical, and pathologic data are presented in Tables 1A and 1B.
Demographic Characteristics.
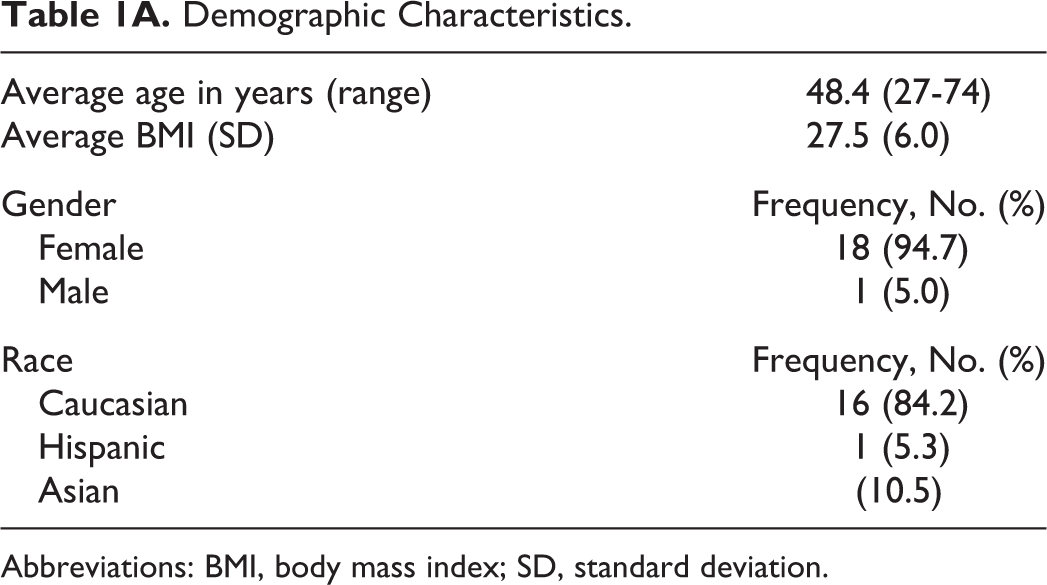
Abbreviations: BMI, body mass index; SD, standard deviation.
Clinicopathologic Characteristics.
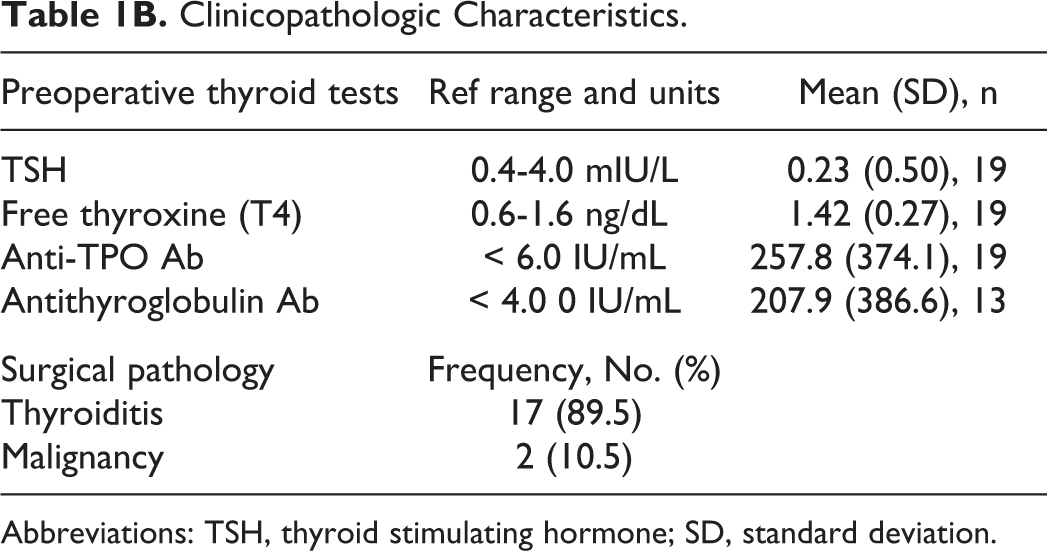
Abbreviations: TSH, thyroid stimulating hormone; SD, standard deviation.
Control Population
Published normative data for the SF-36 were used to represent scores of a healthy, control population with similar demographic characteristics to the patient group; namely, women aged 35 to 54 years (n: 1180-1211). 11 Normative data are shown in Table 2.
Comparison of Short-Form 36 Health Survey Scores.
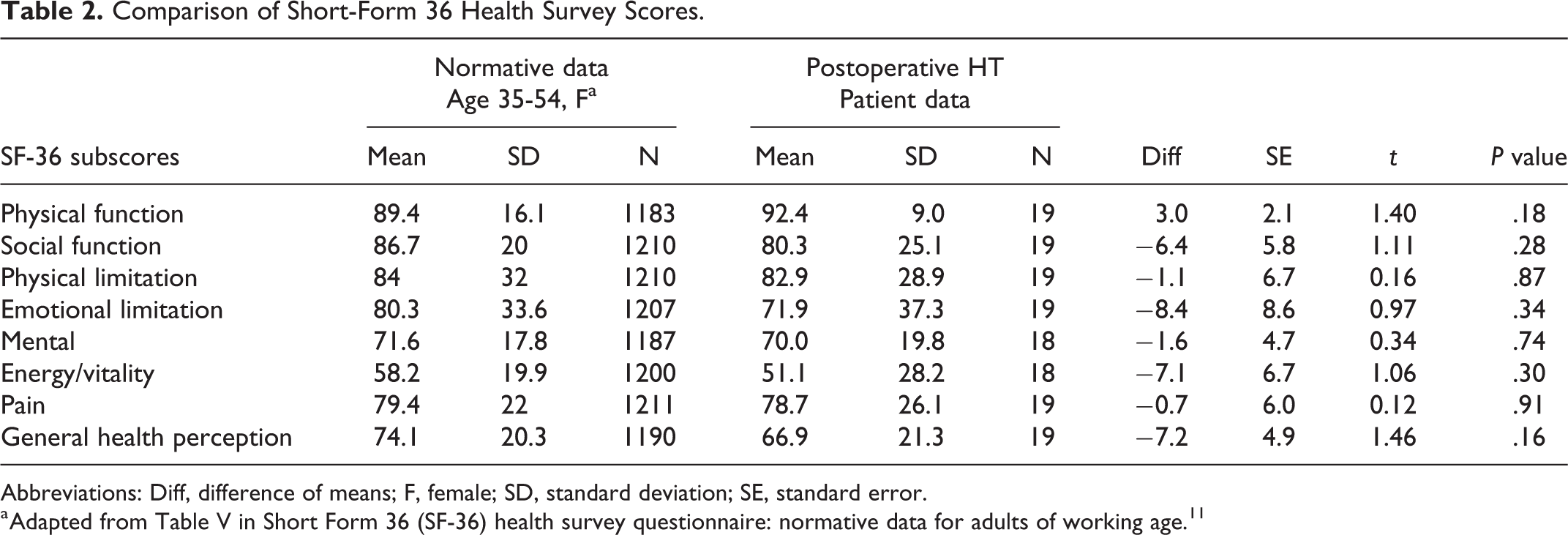
Abbreviations: Diff, difference of means; F, female; SD, standard deviation; SE, standard error.
a Adapted from Table V in Short Form 36 (SF-36) health survey questionnaire: normative data for adults of working age.11
Health-Related Quality of Life
The mean overall SF-36 general health score for the patient group 3 to 35 months (mean 18 months) after surgery was 66.9 (s = 21.3) compared to the mean SF-36 general health score of a control population of healthy women aged 35 to 54 years was 74.1 (s = 20.3). The difference in means between groups was 7.2 points, which was not significant (95% CI: −16.9 to +2.5, P = .16). There was also no significant difference between the post-thyroidectomy and normative groups for all 7 subscores of the SF-36, represented in Table 2. Elevation in preoperative TPO Ab correlated with lower reported postoperative energy levels (r = −0.63, P = .016) and emotional well-being (r = −.55, P = .041).
A secondary survey was developed and distributed by the authors that more specifically addressed changes in management of Hashimoto disease postoperatively as well as satisfaction with surgery and was completed by16 patients; 14 (87.5%) reported they were moderately or extremely happy with their decision to proceed with thyroidectomy. Ten (62.5%) rated their general state of health as being better than before surgery. Frequency of endocrinology visits decreased in 7 (43.8%) respondents after surgery, and frequency of changes in dose or type of thyroid hormone supplementation also decreased in 7 (43.8%). In regard to symptom improvement, higher typical energy levels were reported by 9 (56.3%) patients. Seven (43.8%) patients reported reduction in concentration and memory impairment, pain that interferes with daily tasks, and frequency of low mood. Eight (50%) patients also had fewer missed school/work days than prior to surgery. Survey questions and results are compiled in Figure 1. Regarding adverse events, 9 (56.3%) patients experienced temporary hypoparathyroidism, based on a closing intraoperative parathyroid hormone (IOPTH) level of <15 pg/mL rather than on documentation of hypocalcemia. There were no cases of permanent hypoparathyroidism. One patient had unilateral vocal fold paresis as determined by postoperative flexible laryngoscopy that resolved within 3 months.
Discussion
The cornerstone of treatment for HT is the medical correction of hypothyroidism with thyroid hormone supplementation. However, many patients who achieve euthyroid status continue to report physical symptoms, particularly fatigue, pain, insomnia, cognitive impairment, or mood instability. Indications for thyroid surgery have traditionally included malignant, indeterminate, or symptomatic nodules; goiter, where compressive symptoms such as dysphagia and dyspnea are reliably relieved with surgical intervention; and as one of the definitive treatment options for the autoimmune condition of Graves’ disease. In the absence of these conditions, however, thyroidectomy for persistent symptoms remains controversial.
The pathogenesis for these symptoms is not well understood. Study of joint and rheumatic manifestations in thyroid autoimmune disease has shown the presence of antithyroid antibodies in synovial fluid, sometimes preceding the detection of serum antibodies, suggesting a direct role for antibodies outside the thyroid gland. 12 Alternatively, the dynamic between the autoimmune and predisposing genetic factors may influence the production and response of inflammatory cytokines that contribute to systemic symptoms.13,14 Recent literature suggests genetic polymorphisms in enzymes involved in hormone conversion may be responsible for more baseline symptoms in some patients. 15 This subgroup may benefit from combined levothyroxine and liothyronine, but clinical trial data remain mixed. 16 However, it has been shown that major antithyroid antibodies disappeared after the removal or ablation of all antigenic thyroid tissue, and so would suggest that total thyroidectomy may be a reasonable approach in refractory patients. 17 A recent clinical trial conducted in Norway of patients with preoperative TPO Ab levels exceeding 1000 IU/mL (average 2232 IU/mL) did, in fact, report symptom improvement in all domains of the SF-36 following surgery. 10 In contrast, the noninterventional group who maintained euthyroid status with levothyroxine showed no changes in quality of life over the 18-month study period. It was hypothesized that these results were attributable to a normalization of serum TPO Ab levels in the surgical cohort and, thereby, an attenuation of the autoimmune process leading to a systemic inflammatory state.
Prior efforts have sought to determine reliable criteria for when to consider thyroidectomy to relieve symptoms in patients with HT. In a study of 133 patients with HT, Mcmanus et al reported 90% of preoperative symptoms improved following thyroidectomy. Based on this result, the authors recommended surgery in cases of compressive symptoms, cervical pain, hoarseness, and hormonal fluctuations. 18 Another group in Serbia found significant improvements in all but 2 domains of the ThyPRO quality of life instrument in patients with HT undergoing thyroidectomy compared with those with benign goiter. They suggested that surgery be considered in patients having HT not only with goiter or malignancy but also with decreased quality of life. 19 Conversely, Promberger et al did not observe a clear benefit in quality of life in women with elevated TPO Ab levels and concluded that only compressive symptoms should be targeted with surgery. Those with HT confirmed histologically did show improvement in quality of life, but the authors caution against correlating TPO Ab level with disease presence and severity. 20
In the present study, we sought to lend further information regarding the impact of thyroidectomy on persistent symptoms in patients with euthyroid HT. In this cohort, only those who underwent surgery specifically to address refractory, noncompressive symptoms were included. Results from SF-36 responses demonstrated no significant difference in any domain between post-thyroidectomy HT patients and an age and gender-matched population. Higher preoperative TPO Ab levels correlated significantly with lower postoperative energy levels and lower sense of emotional well-being. There was no significant relationship between SF-36 scores and any other patient factors. An additional survey specifically addressing concerns unique to patients with HT was also distributed. This revealed that 10 (62.5%) of 16 patients felt their general health had improved after surgery, and 14 (87.5%) of 16 patients were either moderately or extremely happy with their decision to proceed with thyroidectomy. Improved energy level was also reported by the majority of patients; 43.8% (7 of 16) reported fewer endocrinology visits, thyroid medication changes, and days with poor mood, intrusive pain, or difficulty concentrating. Temporary hypoparathyroidism was present in 47.4% (9/19) and temporary vocal fold paresis in 5.2% (1/19), both of which are higher rates of temporary complications than cited in most thyroidectomy literature. This is, in part, due to a small sample size. In addition, HT has been recognized as a risk factor for these complications. 21 The cited rate of temporary hypoparathyroidism in this study was based on a level of IOPTH < 15 pg/dL at the end of surgery and not on serum calcium levels nor symptoms. However, all patients had documented normal serum calcium levels on follow-up, and there were no instances of permanent hypoparathyroidism or vocal fold paralysis. There was no significant correlation between adverse outcomes and survey responses.
The authors recognize that a primary limitation to drawing conclusions regarding the impact of surgery is a lack of preoperative SF-36 or other standardized quality of life data. However, prior study has established impaired quality of life in patients with HT in all domains of this survey instrument except bodily pain compared with normative values, even in the euthyroid state.7,22 We may, therefore, infer that a normalization of SF-36 scores in our patient population potentially represents improvement from the preoperative state. Additionally, an inherent disadvantage to the SF-36 is its design to reflect a patient’s status within the preceding 4 weeks. There are a number of health, personal, and other factors unrelated to thyroiditis or thyroid surgery that could influence survey responses in a positive or negative manner. For example, 1 respondent reported a recent nonthyroid surgery leading to decreased quality of life at the time of survey completion. The supplemental questions were designed to assess changes that more specifically relate to thyroid disease and subsequent quality of life. We acknowledge the potential for recall bias in this data set as well as the lack of information due to several missing responses. Finally, the sample size in this study is small, due, in part, to stringent inclusion criteria as well as a 42% survey response rate.
Because of the stringent inclusion criteria, however, the information provided herein is potentially of great utility in treating and counseling patients with HT. While multiple studies have addressed relief of local pain/pressure, dysphagia, or voice complaints after thyroidectomy for Hashimoto goiter,23-25 it is frequently the noncompressive symptoms that present the greatest challenge in disease management and persist despite biochemical euthyroidism. 26 This study specifically addresses the patients that fall into this category, and whose surgical indication was refractory symptoms related to energy, mood, discomfort, and general sense of well-being. Furthermore, there was no minimum cutoff value for TPO Ab level. It has been shown that TPO Ab levels decline in over 90% of patients with HT taking levothyroxine, with 16% normalizing antibody levels after 50 months of therapy. 27 As all included patients were on long-term supplementation, a minimum antibody value was not enforced. It may, therefore, be inferred that even those without significantly elevated autoantibody titers may stand to benefit from thyroidectomy. However, as noted above, higher titers may correspond with lesser, or potentially more delayed, gains in energy and emotional well-being postoperatively. Although the SF-36 is a validated measure, it is intended to be used across many conditions and does not entirely capture reasons for decreased quality of life in the population with HT, which can result from factors such as frequency of physician visits, medication changes, and intermittent memory and mood impairments that interfere with daily obligations. The supplemental survey provides valuable information regarding these additional factors and is unique to this study.
The determination of refractory symptoms related to HT can be challenging and certainly subject to the interpretation of the individual provider. The decision to pursue surgery, therefore, must be made with the patient’s understanding that thyroidectomy may fail to address their concerns. At our institution, surgery is typically reserved for those with long-standing hypothyroidism who have required multiple trials of thyroid hormone in differing combinations and doses, yet continue to report unresolved symptoms. Intervention is pursued only after a measured discussion with the patient and agreement upon expectations.
Conclusions
Although medical management is first line in managing HT, a subset of patients will continue to report intrusive symptoms and decreased quality of life despite euthyroid status. In this study, patients who underwent total thyroidectomy in this scenario reported postoperative quality of life scores on par with a matched healthy population. The vast majority also indicated their satisfaction with having undergone surgery. Although further prospective study is required and planned, these data suggest that thyroidectomy may have a role in the treatment algorithm for refractory HT.
Footnotes
Acknowledgments
The authors would like to acknowledge and thank Yifei Ma, BS, MS, for providing statistical analysis and consultation for this manuscript.
Authors’ Note
All data generated or analyzed during this study are included in this published article (and its supplementary information files). This abstract was accepted for poster presentation at the annual ENDO Society Meeting intended to be held in San Francisco, CA, in March, 2020. It was subsequently cancelled due to COVID-19. Priyanka Thatipamala and Julia E. Noel shared first authorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.