
Abstract
Fibrovascular polyps (FVPs) are rare benign submucosal tumor-like lesions originating in the cervical esophagus and sporadically in the hypopharynx. In this article, we report a rare case of FVPs of the hypopharynx (hFVPs) with a mass measuring 16.0 × 4.0 × 1.8 cm in size, discussed its surgical strategy, and additionally reviewed relevant literature on important factors, such as age, sex, symptoms, size, treatments, and recurrence, associated with hFVPs.
Introduction
Fibrovascular polyps (FVPs) are rare benign submucosal tumor-like lesions arising from the cervical esophagus and sporadically from the hypopharynx.1,2 In this study, we described a rare case of a giant FVP of the hypopharynx (hFVPs) and reviewed its corresponding literature from PubMed Central to discuss the accompanying characteristics and treatments of hFVPs.
This project’s protocol was approved by the Ethics Committee in Gongli Hospital, Second Military Medical University.
Method
Case Description
A 53-year-old man was presented at the Otorhinolaryngology Outpatient Department of our hospital with the chief complain of a 1-year history of progressive hoarseness and sensation of a foreign body in his pharynx.
He was given an endoscopic examination, which showed that the left piriform fossa was shallower than the right-side one, and a neoplasm prolapsing from the left piriform fossa was identified (Figure 1). Fibrolaryngoscopy (A) and esophagoscopy (B) show a mass from the hypopharyngeal inlet.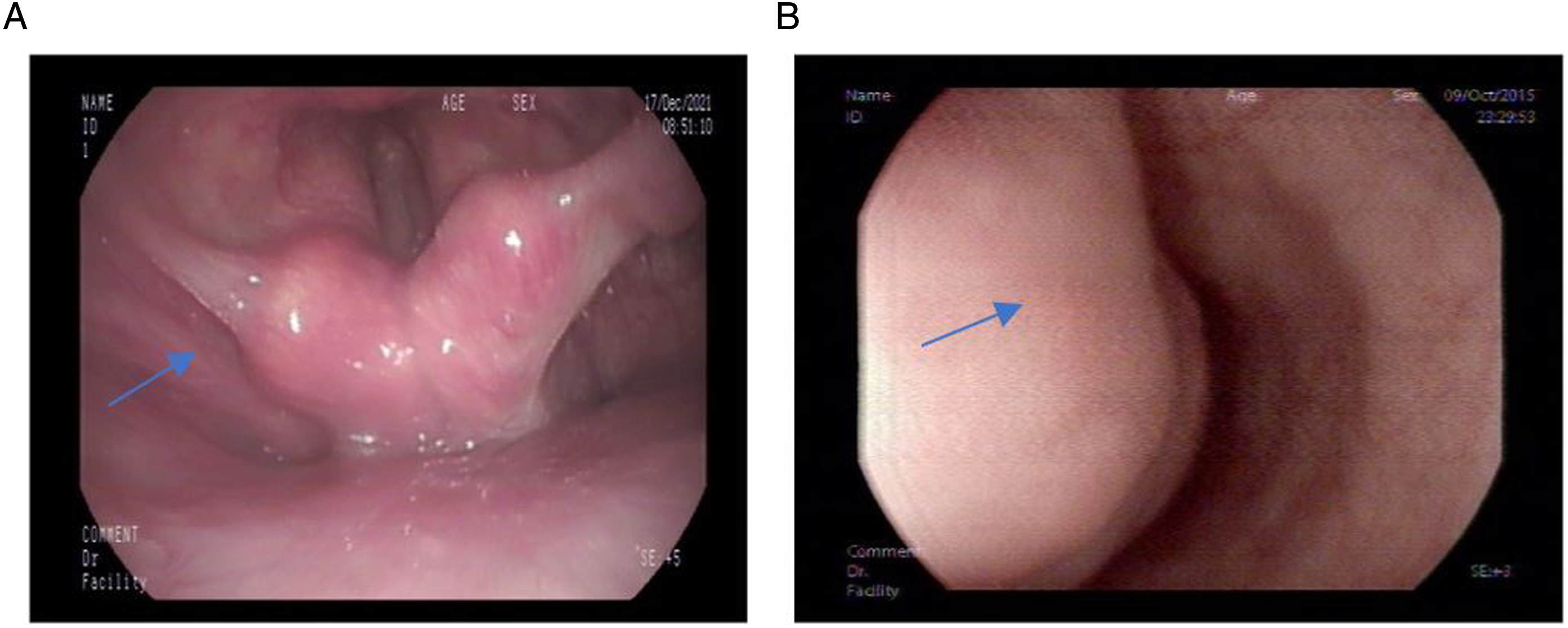
Computed tomography (CT) scanning showed that the neoplasm extended from the oral cavity to the esophagus, expanding the esophagus (Figure 2A). CT (A) and enhanced CT (B) showed space-occupying lesions of the throat and esophagus.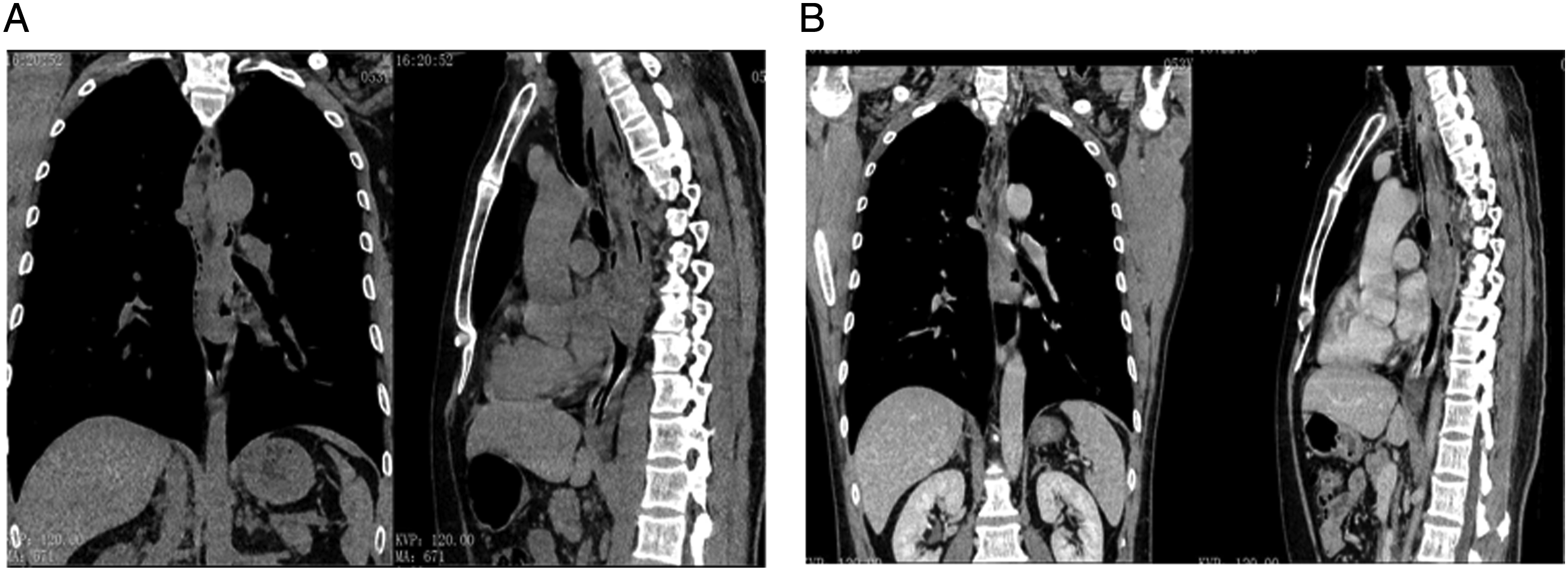
Enhanced CT scan showed complete dilatation of the esophagus, as well as soft tissues and fat density shadows at the affected region. Additionally, the outer wall of the esophagus was smooth, the soft tissues and surrounding vasculature were markedly enhanced, and there was no lymph node enlargement (Figure 2B).
To secure a clear airway, we surgically removed the lesion. Briefly, when a transoral gastroscope was inserted to explore the esophagus, a long strip of mass that protracted approximately 35 cm from the incisor was observed at the esophageal entrance. The neoplasm was soft and smooth and occupied 2/3 of the esophageal cavity. The entrapment was placed at the bottom of the tumor, and the mass was pulled out via the mouth (Figure 3A). (A). The tumor was dragged out of the mouth. The longitude of the tumor was nearly 14.0 cm. (B). The tumor was completely resected, and the tumor size was 16.0 × 4.0 × 1.8 cm.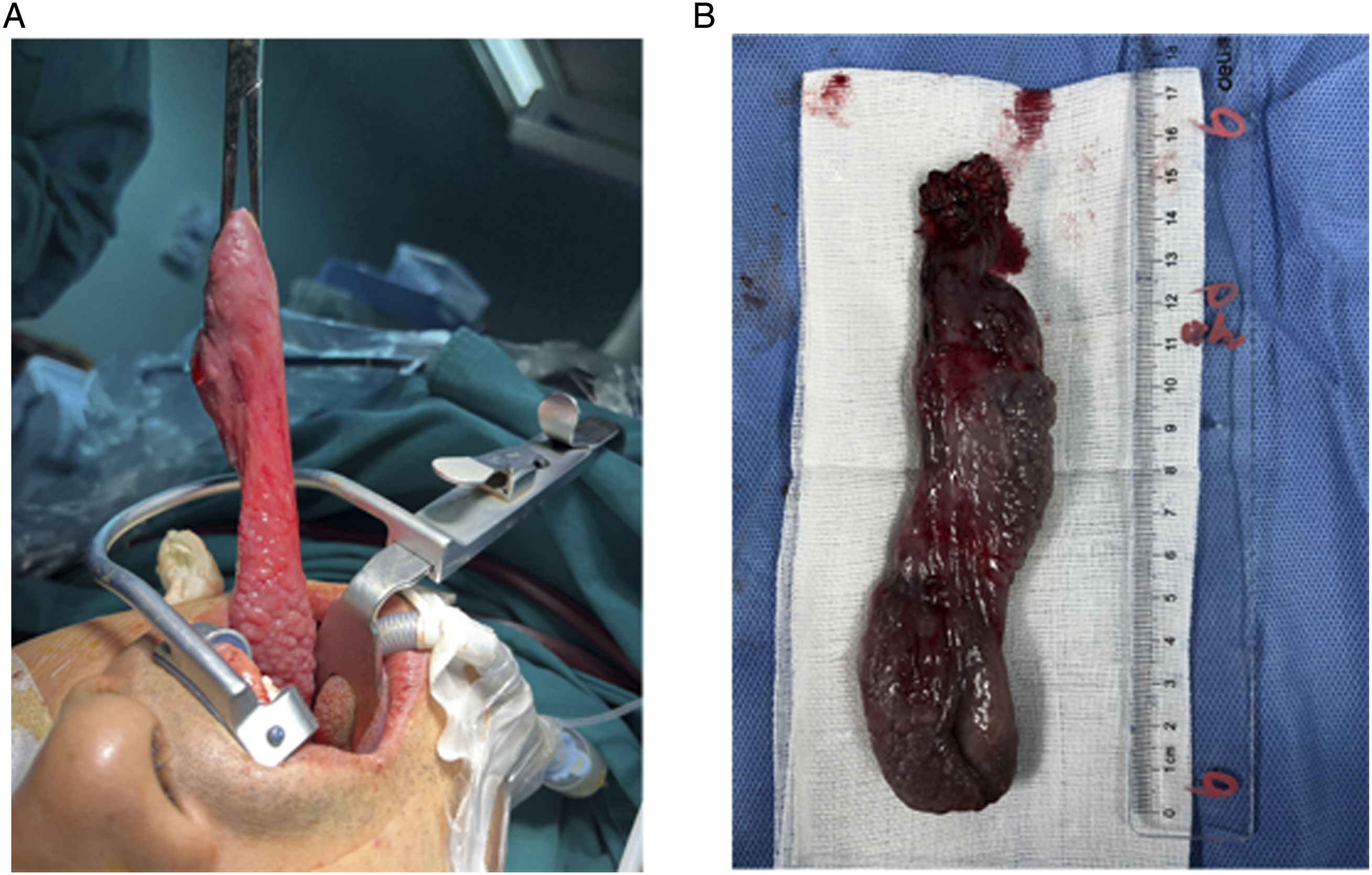
Low-temperature plasma was used to completely resect along the root of the neoplasm. On gross examination, the size of the neoplasm was 16.0×*4.0×*1.8 cm (Figure 3B).
Intraoperative frozen biopsy showed benign lesions of hypopharyngeal mass without malignant tumor cells. Postoperative pathology confirmed that the neoplasm was hFVPs, with lymphatic follicles in the subcutaneous fibrous stroma (Figure 4). The patient had a remarkable postoperative recovery without complications, and a follow-up 10 months after surgery showed that the lesion had not recurred. Hematoxylin and eosin staining (HE) of hFVP (Original magnification ×200).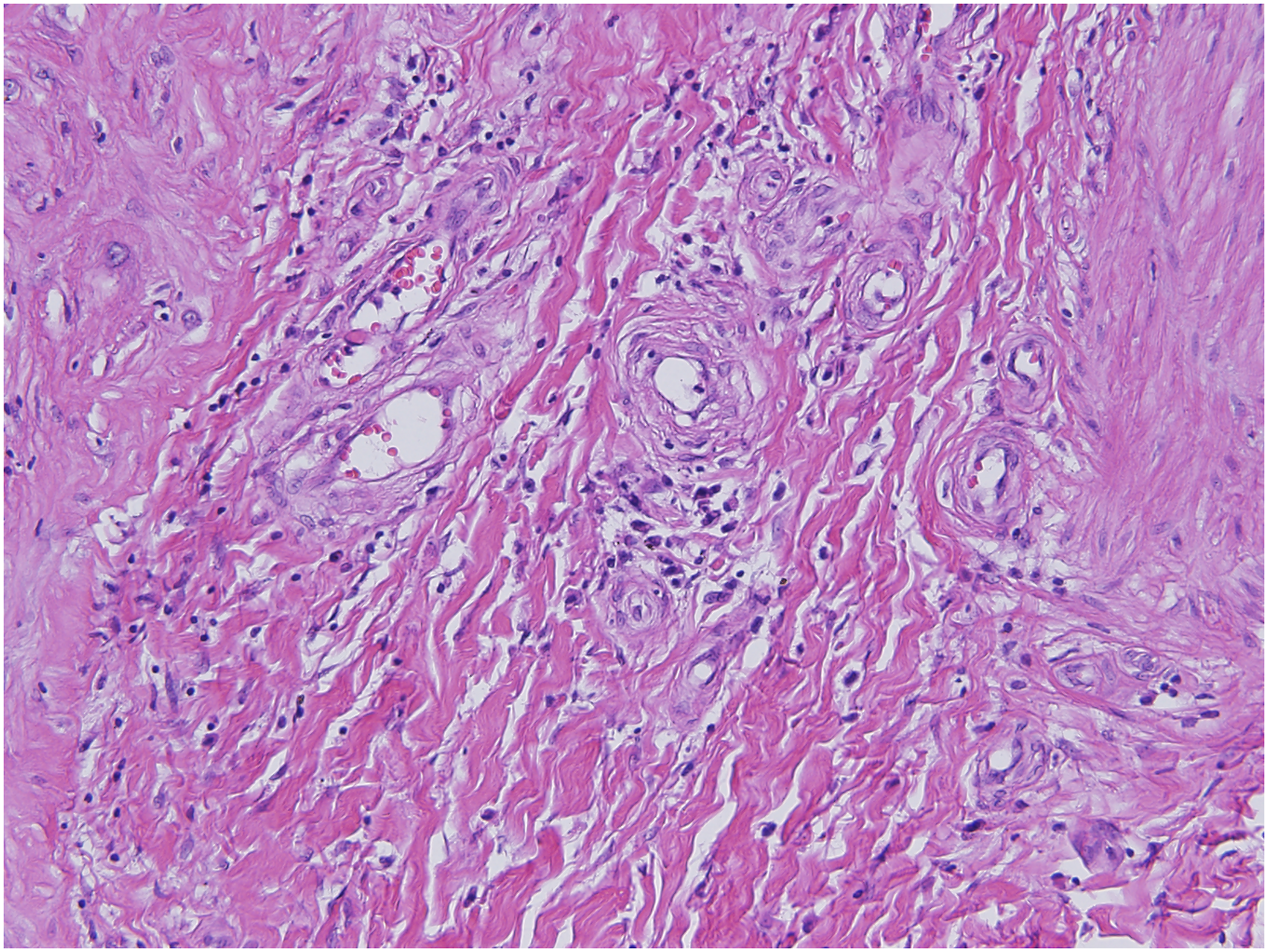
Review of the Relevant Literature
Prior reports of hFVPs.
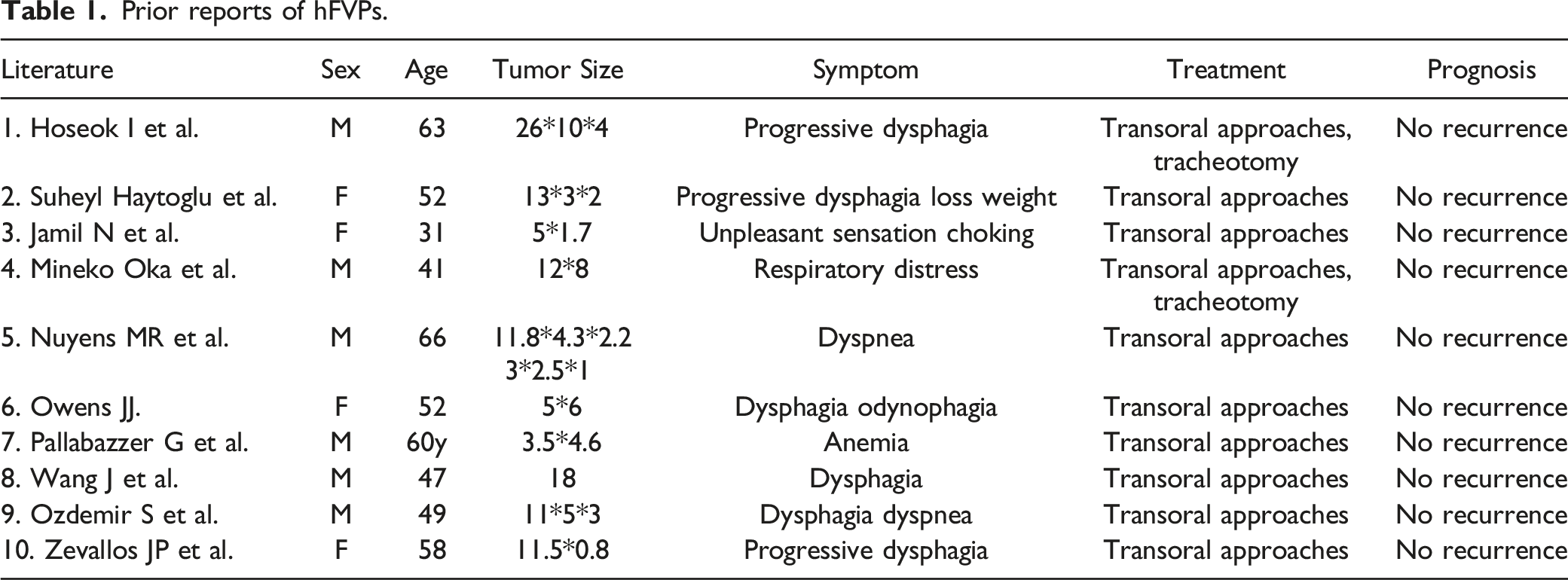
Our results showed that the age at diagnosis ranged from 31 to 66 years old. The hFVPs cases were often accompanied by symptoms such as throat mass sensation, dysphagia, vomiting, laryngeal discomfort, weight loss, anemia, and sore throat. Surgical excision was performed in all cases in which transoral approaches were used in most cases. Tracheotomy was required in 2 cases. The smallest reported polyp size was 3.0 × 2.5 × 1.0 cm, and the biggest was 26.0 × 10.0 × 4.0 cm. However, compared to our present study, none of the previous literature reported lesion recurrence after resection.
Discussion
FVPs are rare benign submucosal tumor-like lesions originating in the cervical esophagus, and on extremely rare occasions, they may arise from the hypopharynx.1,2,13
The occurrence of hFVPs was found to be unrelated to age and sex. Although most cases could present with varied clinical manifestations, 14 the symptoms could be mild or even asymptomatic. However, as the lesion grows, dysphagia, respiratory symptoms, and unpleasant sensation in the pharynx or oral cavity follow. 15 Related nonspecific symptoms could include hoarseness, anemia, weight loss, swallowing pain, and fever.9,16
Endoscopy, CT, and MRI are important imaging modalities for diagnosing hFVPs. The advantage of endoscopy is its wide availability, rapid examination and results, and non-radioactive nature. However, endoscopy might lead to incomplete/inaccurate FVP diagnosis due to its localized nature. One study reported that 25% of intramural and intraluminal esophageal tumors were overlooked on endoscopy. 17 Moreover, the polyp’s mucosa might often be mistaken as normal esophageal or pharyngeal mucosa.3,11 Thus, for proper and accurate diagnosis of hFVPs, multimodal examination is required, such as CT or MRI.
The differential diagnosis of FVPs includes other lesions of the larynx and esophagus, such as hamartoma, inflammatory polyp, lipoma, hemangioma, lymphangioma, and schwannoma. 3
Surgical resection is the definitive treatment. The indications for excision include possible asphyxiation secondary to the prolapse of the polyp into the airway, severe dysphagia, and potential risk of malignancy. 7
The location and size of hFVPs often determine the choice of surgical method. Researchers have demonstrated that small pedicled polyps < 2 cm could be removed by endoscopic ligation and electrocoagulation of the root pedicle. Open surgery could be performed via an external cervical approach for polyps > 8 cm. In recent years, with an increasing understanding on hFVPs and advancements in CO2 laser therapy, low-temperature plasma technology and advanced endoscopic instruments, it is now possible to safely remove polyps > 8 cm under endoscopy, thereby decreasing the need for more invasive procedures. 11
The recurrence rate of hFVPs is low. Endoscopic low-temperature plasma resection can be performed again for recurrent hFVPs that are still benign. Comparatively, for multiple recurrences with large polyps, securing the airway is essential to surgical management. 3 The malignant transformation of hFVPs is reportedly rare.
In conclusion, hFVPs are clinically rare benign submucosal tumors. Dyspnea and dysphagia are the frequently reported symptoms at presentation. Endoscopy, CT, and MRI can help diagnose hFVPs and should be distinguished from other tumors of the larynx and esophagus. The treatment of choice for FVPs is surgical resection, with endoscopic resection being the preferred operative method. However, a lateral cervical approach for resection could be considered for difficult polypectomy of giant hFVPs. Moreover, airway management should be considered as early as possible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by Young Medical Talents Training Program of Pudong Health Bureau of Shanghai (Grant No. PWRq2021-06), Subject Construction Project of Pudong Health Committee of Shanghai (Grant No. PWZy2020-06), Pudong New Area Clinical Characteristic Discipline (PWYts2021-15).
Data Availability Statements
All data generated or analyzed during this research are included in this published article. Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Informed Consent
This article has obtained written informed consent from patients for their anonymized information to be published in this article.