
Abstract
Malignant melanotic nerve sheath tumor (MMNST) is a rare and aggressive peripheral nerve sheath tumor of Schwann cell origin that produces differentiated melanin and is clinically misdiagnosed as malignant melanoma. MMNST is most commonly observed in middle-aged adults and is often found in the midline of the spinal nerve or in the peripheral nerve area. It often manifests itself as a localized mass and/or nervous system involvement. To date, no standard guidelines are available for the treatment of MMNST. Herein, we reported a new case of MMNST that occurred in the parotid gland and reviewed the literature for pathological reports on its association with the oral cavity.
Introduction
Malignant melanotic nerve sheath tumor (MMNST) is often referred to as melanotic schwannoma. It was classified as MMNST based on its malignant clinical manifestations in a review published by the World Health Organization (WHO) in 2021. 1 MMNST is composed of various melanin-producing Schwann cells and is a rare invasive peripheral neurinoma. 2 Its pathogenesis is unclear. The mean age of the patients with this disease was 38.4 years with a male-to-female incidence ratio of 1.1:1. 3 It often occurs clinically in the paravertebral spinal nerve or peripheral nerve regions, such as the cerebellum, orbit, heart, trachea, bronchi, bone, soft tissue, and skin. The clinical presentation is a painless or painful mass growing locally with or without neurological symptoms; a proportion of MMNST is accompanied by Carney’s syndrome. Immunohistochemical staining shows positive for markers S100, SOX10, HMB-45, Melan-A, and P16, especially diffuse strong positive for S100 and SOX10.1,2 To date, only 8 related cases have been reported in the oral area. Due to the small number of reported cases, it is difficult to define a standard treatment and predict the prognosis systematically. Herein, we reported a rare case of MMNST that occurs in the parotid gland and a review of the relevant literature to provide clinicians with more ideas for treatment and diagnosis.
Case Presentation
A 52-year-old male had a history of more than 1 month of a painless mass under his right earlobe. The patient was admitted to the oral and maxillofacial surgery ward of Taihe Hospital, Shiyan, Hubei Province. The patient had a history of hypertension for 15 years without a specific personal or family history.
Physical examination showed a 1.5 × 1.5 × 1 cm tender swell with a clear edge of the basilar part of the skin and 25 residual roots in the mouth. The remaining teeth were straight without facial paralysis symptoms, as well as abnormalities of the oral mucosa and parotid gland duct. No lump was observed in both the ipsilateral lateral pharyngeal wall and the submandibular region. An auxiliary positron emission tomography computed tomography (CT) scan revealed a space-occupying lesion in the lower right parotid gland (Figure 1). The CT scan of the lesion. A 3 cm occupying lesion in the lower right parotid gland (blue arrow).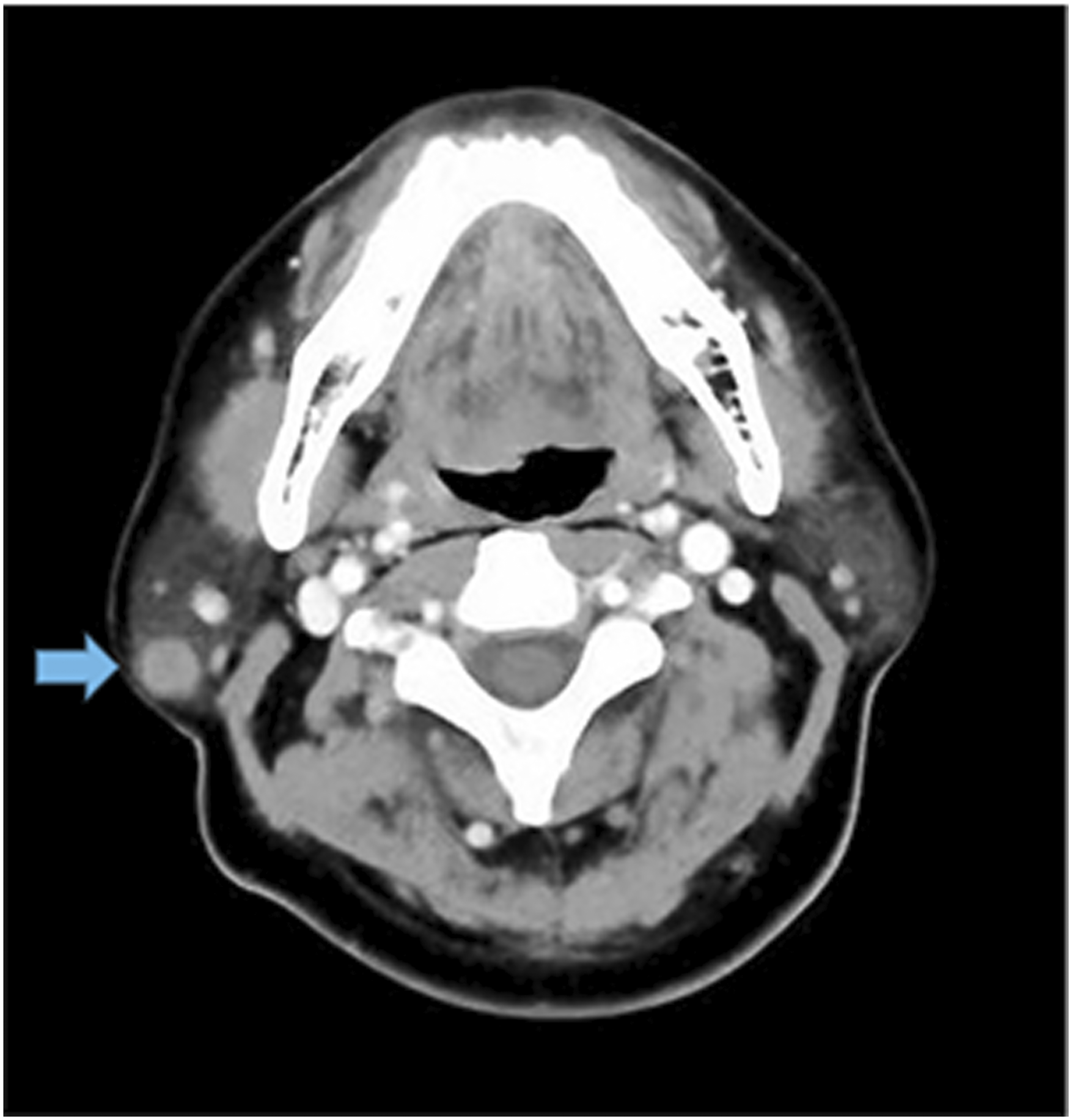
The initial diagnosis was a mixed tumor of the parotid gland or schwannoma. After general anesthesia, an excision of the space-occupying lesion, partial parotidectomy, and simple lymphadenectomy was performed in the right parotid gland.
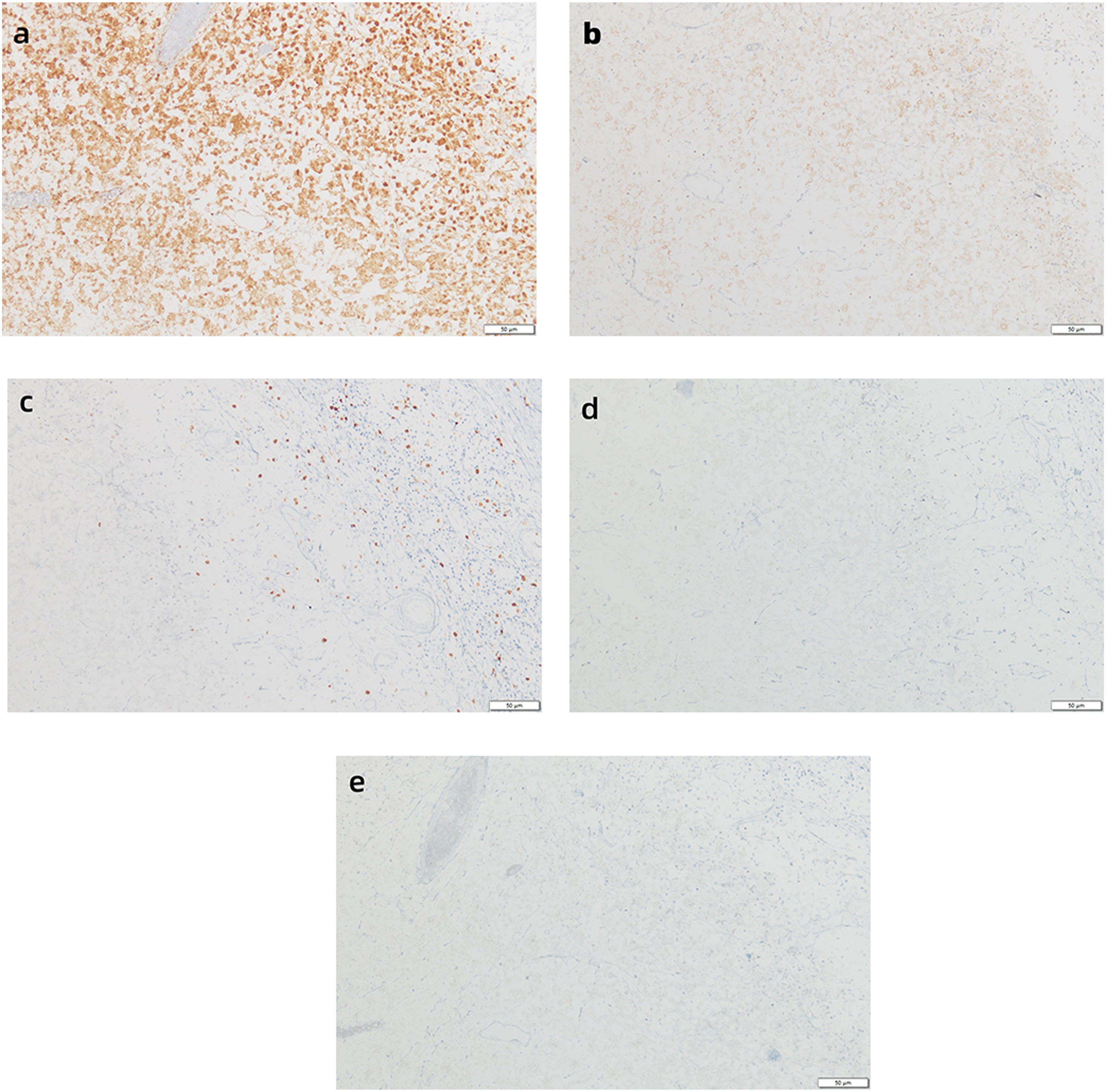
According to the macroscopic observation of the excised tumor, there was a protrusion in the middle of the tumor, which was 0.4 × 0.3 × 0.1 cm with a black, brownish surface, slightly rough and tender. The lesion of the right parotid gland was 5 × 3 × 2 cm. The tumor was cross-sectioned, and its diameter was measured to be 2.5 cm. A solid black nodule was observed on the cut surface, which is soft and well-defined. The remainder of the tissue was solid, gray-yellow, and soft in texture. We stained the tissue with hematoxylin and eosin staining (H&E) and immunohistochemistry (IHC). Optical microscopy showed that the tumor was well circumscribed without an envelope. Spindle cells rich in melanin were arranged in bundles or whirlpools (Figure 2A). The epithelial cells high in melanin were loosely ordered (Figure 2B). The results of IHC staining showed that the S-100 protein was diffusely expressed in the nucleus and cytoplasm of tumor cells (Figure 3A). The IHC stains were positive for the melanoma markers HMB-45 (Figure 3B) and Ki-67 (Figure 3C); however, they did not express the melanin markers Melan-A (Figure 3D) and SOX 10 (Figure 3E) in the tumor cytoplasm. H&E staining showing (A) the spindle cells rich in melanin arranged in bundles or whirlpools, 40× magnification; (B) The epithelial cells high in melanin loosely put in order, 100× magnification. IHC staining showing (A) The S-100 protein reacts positively with the tumor cells, which then express it widely in the cytoplasm and nucleus; (B) The tumor cells positively for melanoma markers HMB-45; (C) The Ki-67 antigen labeling index <1%; (D) The tumor cells do not express melanin markers Melan-A; (E) The tumor cells do not express melanin markers SOX-10, 200× magnification.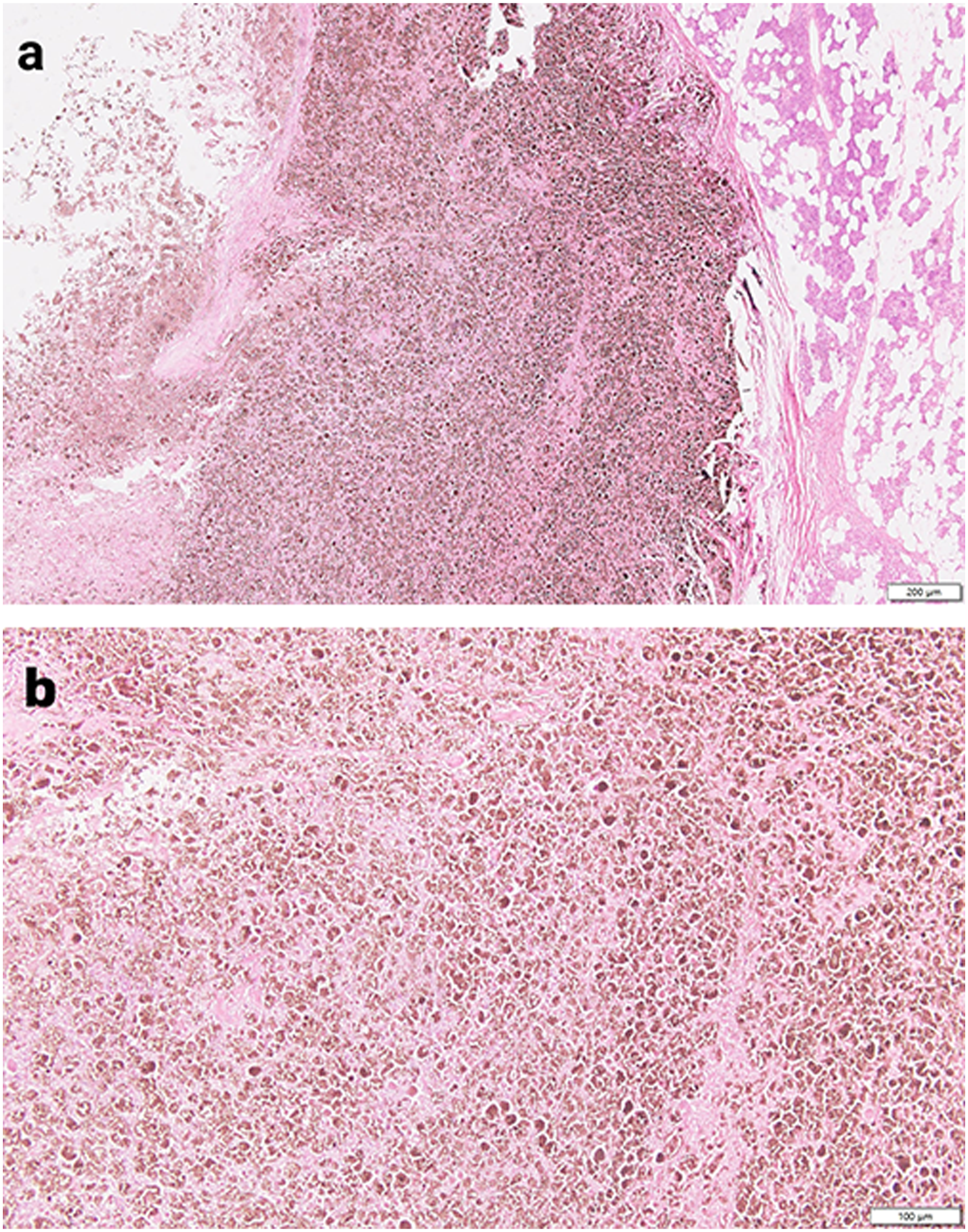
Based on these indications, this tumor was diagnosed as an MMNST that occurs in the right parotid gland. The patient recovered well after the surgery without radiotherapy and chemotherapy and was discharged in good health.
Discussion
The Supplemental Characteristics of MMNST Occur in the Oral Cavity.
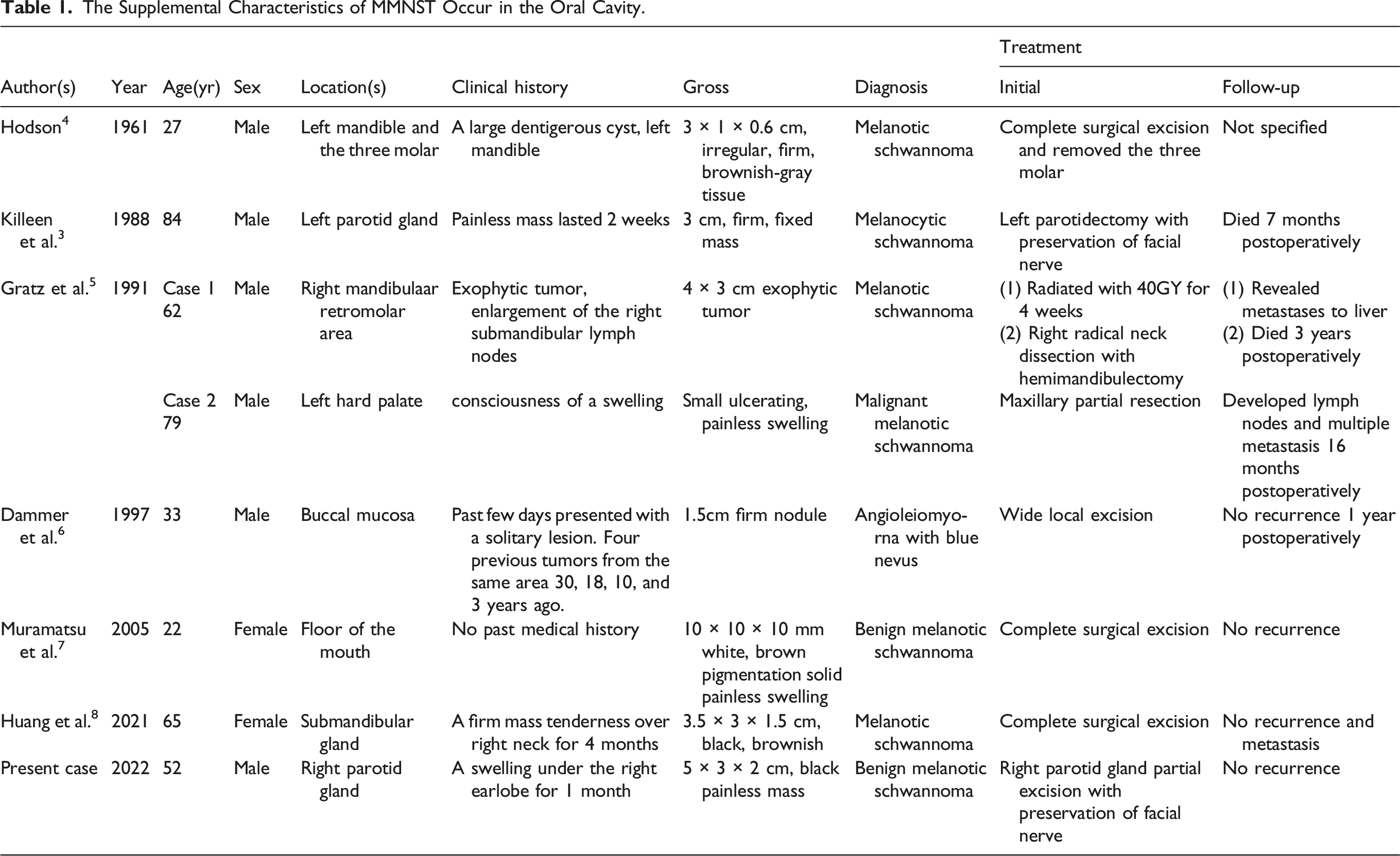
Anatomical sites with oral MMNST were available in 8 cases: mandible (n = 2), parotid gland (n = 2), submandibular gland (n = 1), hard palate (n = 1), buccal mucosa (n = 1), and floor of the mouth (n = 1). The age of the 8 reported cases ranged from 22 to 84 years (mean, 53 years; median, 57 years), of which 6 of the 8 cases were male, and the remaining were female.
The clinical presentation varied according to the site of the tumor. However, based on the descriptions of the lesions related to the 8 cases, we found the tumor was a size of 1–5 cm, with a median of 3 cm (average, 2.88 cm). All patients underwent surgical resection of the tumors. Follow-up was available in 8 cases, which ranged from 7 months to 3 years. During the follow-up period, 2 patients died, one patient developed multiple lymph nodes and distant metastasis, 4 patients had no recurrence and metastases after surgery, and one patient whose follow-up information was not available.
According to the classification of tumors of the central nervous system published by WHO in 2021, melanotic schwannoma or melanocytic schwannoma is classified and renamed MMNST. 1 MMNST is a rare lesion of the nervous system and rich in melanin, which has the same immunohistochemical characteristics as malignant melanoma. 2 It has not yet been reported to occur in children. 9 The general age of MMNST incidence is 10–49 years, but the peak of incidence is 38–40 years. There are no significant differences in sex, geography, and race in the reported cases. 10 The tumor can occur in any part of the peripheral nervous system but is commonly found in the paravertebral sympathetic ganglia and gastrointestinal tract, rarely in the orbit, cerebellum, heart, trachea, cervix, bone, soft tissue, and skin.2,11 Lesions are often found incidentally. Most patients present with a localized painful mass with some neurological symptoms depending on the location and growth rate of the tumor. 2
Mostly, MMNST is a round or oval mass with expansive growth covered by a thin fibrous membrane, which is delimited from the surrounding normal tissue. The section of the mass is black, brown, or gray, and sometimes it may be rough. The diameter of the phyma is generally more than 5 cm.2,12
Histologically, the tumor is well circumscribed and without encapsulation. It consists of atypical spindle cells and epithelial Schwann cells arranged in fascicles, intertwined, and nested orders. Pigmented granules can be observed in the cytoplasm, which can cover the nucleus when the granules are in large numbers. We can observe vacuoles in the cytoplasm of some tumor cells, which are similar to mature adipocytes and lack Verocay bodies. The nuclei usually present are round or oval with rare mitosis. Sometimes atypical degenerative changes, such as nuclear hyperchromatic staining, chromatin contamination, and pseudoinclusion bodies, can be seen in the nucleus. Stratified calcified globules can be observed in some tumors. The nuclei of tumor cells will enlarge, chromatin will vacillate, and the mitotic figures can be easily observed in the malignant process. Tumor cells can infiltrate peripheral tissue, accelerating the recurrence and metastasis of the tumor. IHC staining shows better positivity for S100 and/or SOX 10 and positivity for HMB-45, Melan-A, P16, and vimentin. The linear, peri-cytoplasmic immunoreactivity of laminitis and collagen can be detected in most cases.12-14
The etiology of MMNST remains unclear. The current theories include the melanomatous transformation of neoplastic Schwann cells, phagocytosis of melanin by Schwann cells, and the presence of 2 different neoplastic populations of proliferating melanocytes and Schwann cells. 14 In addition, there is a high correlation between MMNST and the Carney complex (CNC). CNC is a rare autosomal dominant multiple endocrine neoplasia syndrome (hyperendocrine-pigmentation-myxoma triad) caused by the deficiency of PRKAR1A.15,16
Due to the small number of reported cases, there are no clear criteria for MMNST. To date, gross total excision remains the main method of primary treatment for MMNST. It has been reported that the local metastasis and recurrence rate was 15%–35%, and the metastasis rate was 26%–44% within 5 years.15,16 We recommend adjuvant radiotherapy or chemotherapy when there is a development of malignant clinical features or inadequate resection, but the effectiveness of this method remains to be investigated. In addition, MMNST can still recur or metastasize after 5-year surgery, indicating the need for long-term follow-up. 12
Conclusion
We reported a case of MMNST that occurs in the parotid gland and a literature review on MMNST in the oral cavity. However, this report had several limitations due to the small sample size for the literature review, differentiation of treatments, and partiality of the follow-up. Therefore, we must improve long-term follow-up and clarify the method of remedy.
It is a rare case since the MMNST occurs in the parotid gland. The diagnosis is based mainly on clinical symptoms combined with radiography and histopathology. We should pay attention simultaneously to the differential diagnosis of malignant melanoma, melanoma neurofibroma, and other nervous system tumors. Although the prognosis is grossly good, the biological behavior of MMNST is difficult to predict nowadays and may still relapse and metastasize locally. In the future, we should follow the long-term follow-up record with interest.
Footnotes
Acknowledgments
We express many thanks to the patient for generously authorizing us to share his rare case.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Health Commission of Hubei Province scientific research project (No. WJ2021M049).
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are investigated and resolved. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013). Written informed consent was obtained from the patient for publication of this Case report and any accompanying images.
Data Availability
The data that support the findings of this study are available from the corresponding author (NY), upon reasonable request.