
Abstract
While gastric cancer often metastasizes to the liver, lymph nodes, and lungs, skeletal muscle metastasis is a rare event. The most common primary tumor metastasizing to the extraocular structures is breast cancer. Gastric carcinoma metastatic to the extraocular muscles is a rare event announcing a spreading disease with a bad prognosis. Here, we report a case of an asymptomatic gastric carcinoma metastasizing to the superior oblique muscle diagnosed via an endoscopic endonasal biopsy.
Introduction
Gastric cancer is an aggressive disease. While this tumor often metastasizes to the liver, lymph nodes, and lungs, skeletal muscle metastasis is an extremely rare event. 1 Among the skeletal muscle metastasis, extraocular muscle (EOM) invasion is even more unusual. 2 The most common primary tumor metastasizing to the extraocular structures is breast cancer followed by lung cancer, prostate cancer, and cutaneous melanoma. 3
Ocular metastasis from gastrointestinal tract primitive had only been seen in 11% of cases with EOM metastasis. 4 Gastric cancer metastatic to the EOM is even rarer. 2 Few studies have reported the clinical features, characteristic imaging findings, and therapeutic modalities of this rare condition.
We report a case of an asymptomatic gastric carcinoma metastasizing to the superior oblique muscle diagnosed via an endonasal trans-ethmoidal biopsy.
Case presentation
A 53-year-old man was referred to our hospital with a 2-month history of right orbital pain, diplopia, decreased visual acuity, and headaches. He was a heavy smoker and had no particular medical or surgical history.
Physical exam revealed a restriction of the right eye movements on the down and right medial gaze (Figure 1), a normal eye fundus, and a decreased visual acuity score 20/32 following the Snellen chart. There was no neck lymphadenopathy. The nasal endoscopic examination was normal. Clinical photograph showing a restriction of the right eye movements on down and right medial gaze.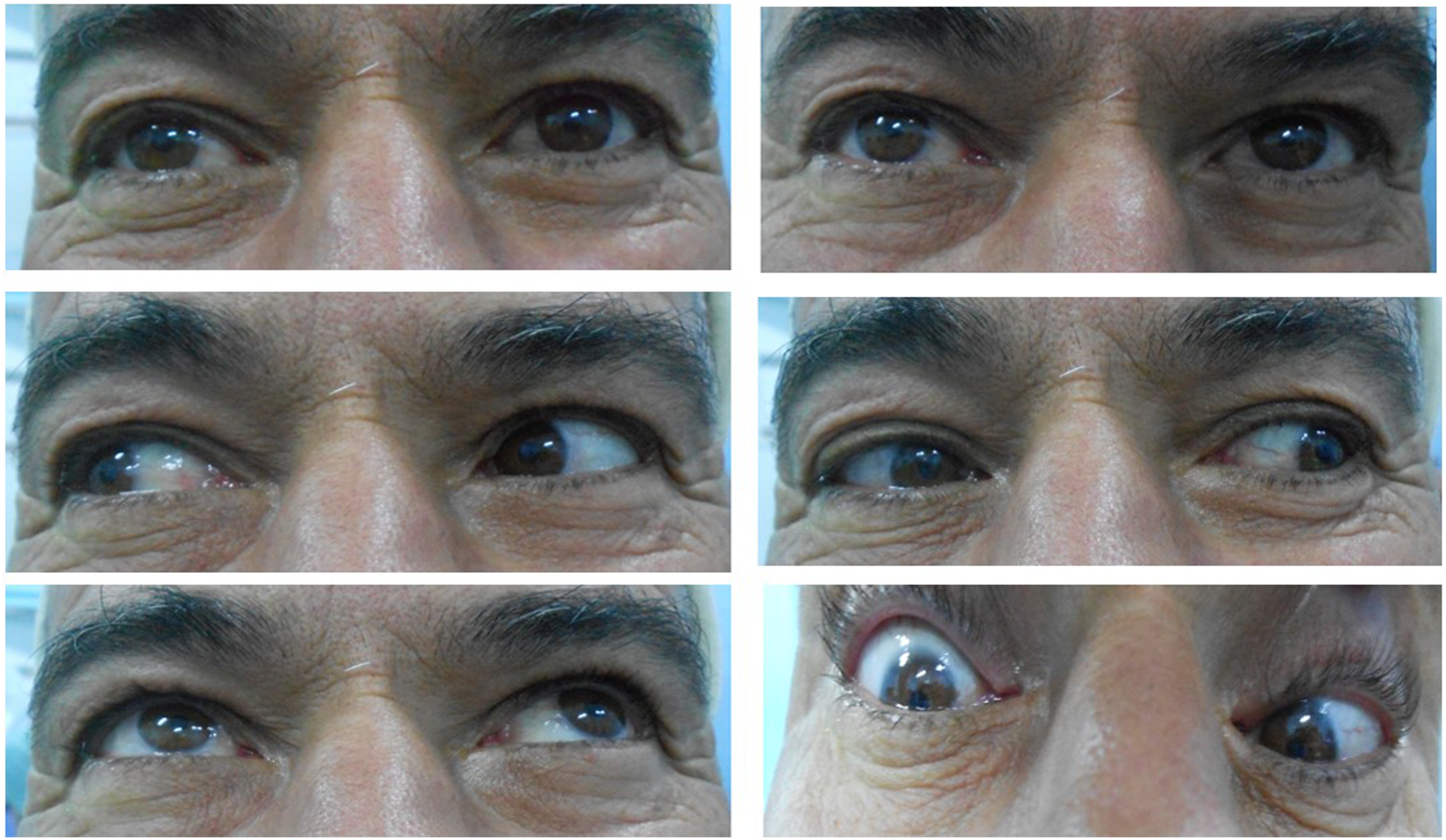
Computed tomography of the orbit showed a nodular enlargement of the right superior oblique muscle, located 1 cm anterior to the orbital apex, measuring 18 × 13 mm with no osteolytic lesion (Figures 2A and 2B). Magnetic resonance imaging (MRI) showed an isointense mass of the right superior oblique muscle on T1-weighted images with an intense enhancement after gadolinium contrast (Figure 2C). Preoperative imaging. A nodular enlargement of the right superior oblique muscle (*) on axial (A) and coronal (B) computed tomography of orbits. Postcontrast T1 MRI (C) showing an enlargement and enhancement of the right superior oblique muscle (*).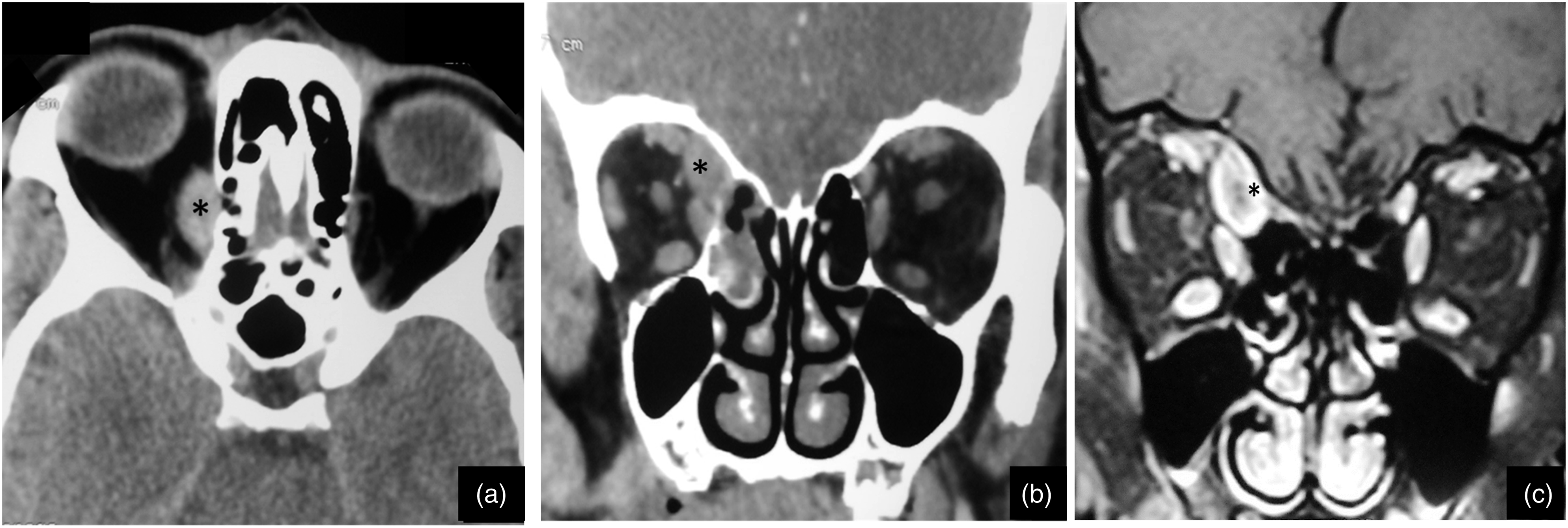
The patient underwent an endonasal procedure consisting of a right ethmoidectomy giving access to the orbital mass through the medial wall of the orbit. Intraoperatively, the mass was infiltrating the superior oblique muscle. A biopsy was performed. Histopathological examination found a metastatic adenocarcinoma that could be secondary either to a gastric or to a pulmonary primitive (Figure 3). Further workup found multiple pulmonary nodules on bilateral lungs. We performed esophagogastroduodenoscopy, which revealed a 4 cm ulceroinfiltrative gastric tumor, and endoscopic biopsies showed moderately differentiated adenocarcinoma from the gastric epithelium. Our patient died before completing his courses of chemotherapy. Hematoxylin and eosin staining of the orbital biopsy specimen revealed adenocarcinoma mainly composed of irregular cords and clusters with occasional ductal structures.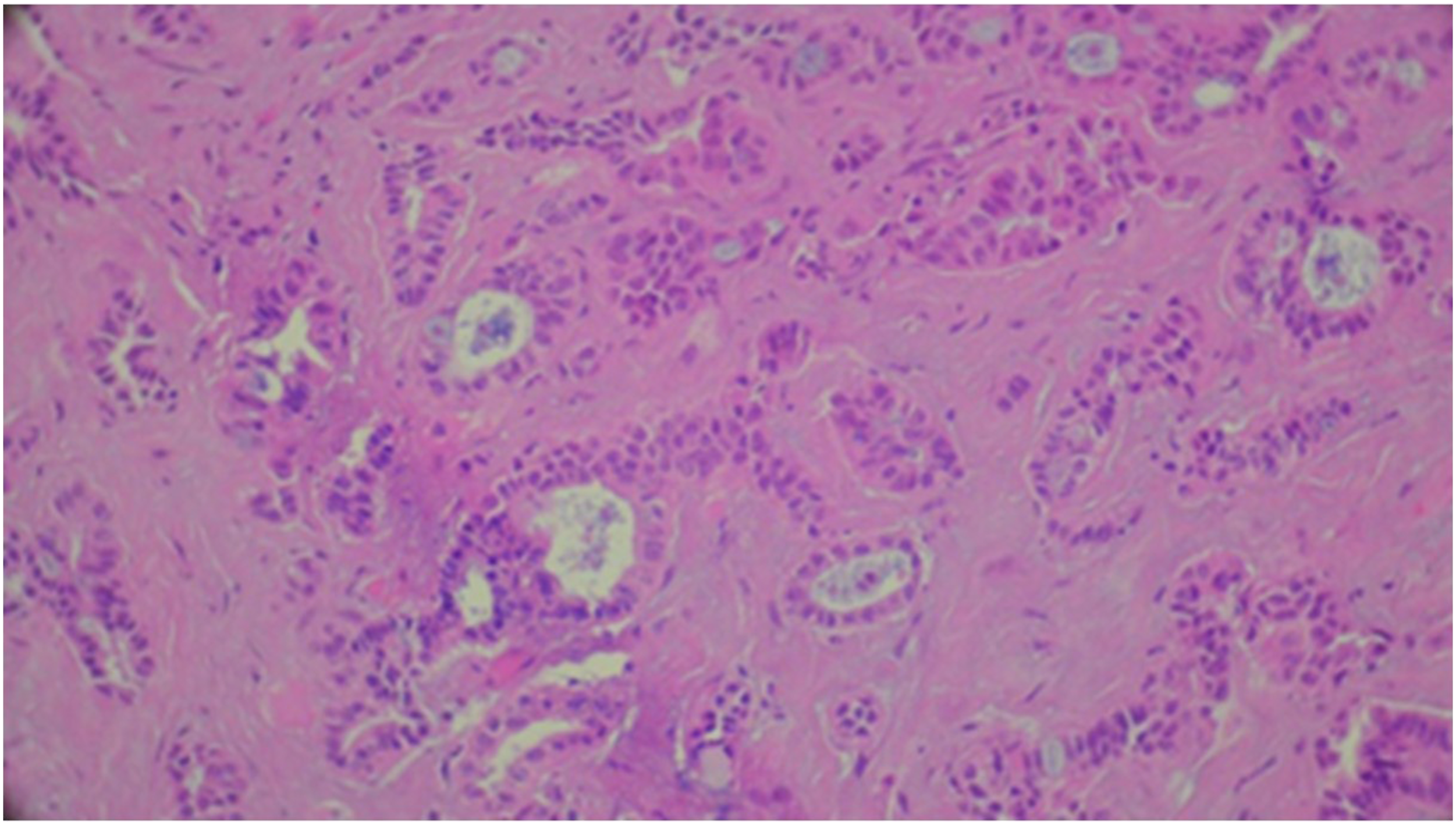
Discussion
Orbital metastases may occur in 2% to 3% of patients with systemic cancer. 3 In 19% to 51% of patients, the primary neoplasm was diagnosed from the orbital tumor.3,5 EOM metastasis accounts for 0.07% to 4.7% of patients with malignancy. 2 It is the second most common orbital site after the choroid. 6 EOM invasion usually reflects an extensive hematogenous spread, thus an advanced disease stage. 7 Metastatic orbital tumors most commonly arise from breast cancer in women, lung cancer in men, and neuroblastoma in children. 8 Orbital metastasis of gastric carcinoma is a rare event, and literature about EOM metastasis of gastric cancer is poor so far. 1 In our case report, ocular symptoms revealed an unknown primary gastric adenocarcinoma. The patient was healthy and asymptomatic.
A multitude of clinical presentations of orbital metastasis has been described in the literature. Diplopia and orbital pain are the most commonly reported symptoms at the time of presentation. 7 The most frequently affected extraocular muscle is the medial rectus, followed by the lateral rectus, the superior rectus, and the inferior rectus, respectively. 4 To our knowledge, this is the first report of a gastric carcinoma metastasizing to the superior oblique muscle.
Given the absence of specificity of EOM metastases clinical presentation, other common etiologies of EOM enlargement must be considered, including thyroid-related orbitopathy, bacterial or fungal infections, and infiltrative disease, such as amyloidosis. 7
Imaging can differentiate inflammatory lesions and tumors from proliferating lymph infiltrates. Orbital bones, cranial cavity, and EOM invasion should be evaluated by CT scan. 7 However, orbital soft lesions are better explored by MRI than CT. EOM metastasis may result in a well-defined round or fusiform mass involving the EOM with variable signal intensity and contrast enhancement in MRI. While solitary lesions are maybe difficult to differentiate from other masses, multiplicity is an indicator of metastasis. 6
The definitive diagnosis of an extraocular lesion requires a diagnostic tissue. Fine-needle aspiration biopsy has been the most commonly used diagnostic modality. 9 However, this procedure can lead to tumor cell dissemination. It also can cause a globe injury. 10 The endonasal endoscopic route has the advantage of providing a wide field of view and is minimally invasive. 8 Hence, trans-ethmoidal endonasal biopsy, as proceeded in our case, is an effective and safe alternative for medial, infero-medial, and apical orbital tumors since they are not eligible for fine-needle aspiration biopsy. When symptomatic of compression, the endonasal approach can also help in ocular globe decompression.8,11
Given their poor prognosis, palliation of symptoms and survival prolongation are the main goals of orbital metastasis treatment. Radiation therapy is typically offered to such patients, while surgical resection is only advisable when patients present with intractable pain or well-circumscribed tumors.7,12 Orbital decompression surgery may be a useful option for palliative purposes. 8
In summary, gastric adenocarcinoma metastatic to extraocular muscles is a rare event and can precede the detection of the primary tumor. It reflects an advanced stage of the disease with a poor prognosis. Trans-ethmoidal endonasal biopsy is preferred to fine-needle aspiration biopsy allowing a diagnostic tissue.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.