
Abstract
Background
To assess whether specific selective neck dissection (SND) with involved levels is a feasible treatment for isolated regional failure in nasopharyngeal carcinoma (NPC) after radiation.
Material and Methods
Between January 2011 and December 2019, a total of 46 patients were assigned to undergo SND in the Department of Head and Neck Surgery at our center. The dissection extent of specific SND usually only involved levels of lymph node sites for isolated regional failure; in addition, lesions of level II or III involved removing both level II and III lymph nodes. The patients’ clinical, MRI and pathological characteristics, overall survival (OS), disease-free survival (DFS) and regional-free survival (RFS) were evaluated and analyzed.
Results
Level II was the most commonly involved cervical nodal region in 28 neck dissection specimens (54.9%), followed by level III with positive nodes in 11 specimens (21.6%). Eleven patients (34.8%) had post-SND locoregional recurrence without distant metastasis. Of the patients, 7 patients (30.4%) had regional recurrence, and only one patient (2.8%) had lymph node recurrence on the side of SND. In addition, 8 patients (17.4%) had post-SND distant metastasis. The OS, DFS, and RFS of the patients were 76.1%, 58.7%, and 69.6%, respectively, at 3 years. The OS, DFS, and RFS values of patients who underwent SND were similar to those of patients who underwent comprehensive neck dissection (CND) and/or SND in published articles.
Conclusion
Specific SND was shown to be an effective and feasible treatment for isolated regional failure in NPC.
Introduction
Nasopharyngeal carcinoma (NPC) is a common malignant tumor in Southeast Asia and Southern China, 1 with an incidence of 30–50 per 100,000 persons, 2 while there are fewer than 1 case per 100,000 persons in the US and Europe. 3 NPC has a high propensity to metastasize to cervical lymph nodes, with 49–85% of patients with metastasis at presentation. 4 Radiation therapy with or without chemotherapy has been the standard treatment for NPC, with the local control rate and overall survival at 5 years exceeding 90% and 80%, respectively. However, the incidence of isolated regional failure is 3.7% to 18%. 5 Reirradiation for regional failure is unfavorable due to its association with high morbidity. Regional failure of NPC requires surgery for neck dissection.
The standard treatment for regional failure of NPC is comprehensive neck dissection (CND), including radical neck dissection (RND) or modified radical neck dissection (MRND), with 5-year survival node control rates of 65–70%. 6 However, compared with CND, selective neck dissection (SND) has a smaller extent of dissection, which might result in less injury or fewer complications and a higher quality of life for patients. 7 In recent years, some authors have suggested that SND is not inferior to CND for patients with isolated regional failure. 8 However, few published studies have focused on a specific range of SND in NPC patients with isolated regional failure.
Therefore, we retrospectively analyzed 46 patients to summarize whether a specific range of SND with involved levels is a proper choice for isolated regional failure NPC patients.
Materials and Methods
This study was approved by the ethical committee of our hospital, and the requirement for informed consent was waived. This study was performed in accordance with relevant guidelines and regulations.
Patient Characteristics
We retrospectively reviewed the records of patients who were diagnosed with isolated regional failure NPC and underwent SND between January 2011 and December 2019 at our hospital. In total, 46 patients were recruited for this study, including patients with recurrent and residual disease. The data that were reviewed included demographics, clinical pathological characteristics, radiological characteristics, treatment information, and follow-up data. All patients were staged according to the American Joint Committee on Cancer TNM Staging System 8th edition.
All of the patients diagnosed with NPC were primarily treated with a standard course of conventional radiotherapy (RT) or intensity-modulated radiotherapy (IMRT) with or without chemotherapy. Among the 46 patients, 28 patients were treated with RT, and 18 were treated with IMRT as their first therapy. The principles of treatment consisted of 66–72 grays (Gy) to the primary tumor, 60–70 Gy to the involved lymph nodes and 50 Gy to the uninvolved neck administered as single daily fractions of 1.8–2.0 Gy for 5 days a week over 6–7 weeks.
Tumor Characteristics
The patients were diagnosed as having isolated regional failure on the basis of histology and/or radiology. All the patients had WHO type 3 carcinomas histopathologically, which are the most common in southern China. Recurrent nodal disease was defined as the reappearance of lymphadenopathy after initial complete regression of nodal disease. 9 For patients with NPC, when their neck nodes had not regressed completely by 3 months after the completion of therapy, this was defined as residual nodal disease. 10
Treatment
Before receiving salvage treatment for regional failure, the patients also underwent a complete physical examination (including nasopharyngoscopy and biopsy for suspicious nasopharyngeal lesions), magnetic resonance imaging (MRI), and positron emission tomography/computed tomography (PET-CT) to exclude local disease and distant metastases. Some patients also underwent ultrasound-guided fine-needle aspiration cytology (FNAC) to confirm the status of regionally recurrent or residual disease. All patients underwent SND. Unilateral or bilateral neck dissections depended on the assessment of suspicious disease. The extent of SND depended on the extent of clinical or radiological disease and the patterns of lymph node metastases. In our hospital, the dissection extent of SND usually only involved levels of lymph node sites for isolated regional failure; in addition, lesions of level II or III involved removing both level II and III lymph nodes. The extranodal extension of lymph nodes requires adequate surgical margins. Usually, for cases with extranodal extension or positive surgical margins, postoperative chemotherapy may also be applied. The patients were regularly followed up to assess their disease status. Follow-up included physical examinations, nasopharyngoscopy, chest CT, abdominal ultrasonography, MRI of the head and neck, bone scanning, and/or PET-CT every 3 months in the first 3 years after surgery, every 6 months in years 3 to 5, and annually thereafter.
Statistical Analysis
Overall survival (OS) was defined as the time from diagnosis to death from any cause. Disease-free survival (DFS) was defined as the time from diagnosis to local, nodal, or systemic recurrence or death from any cause, whichever occurred first. Regional-free survival (RFS) was defined as the time from diagnosis to nodal recurrence. The study was a single-cohort study comparing results with the values of OS, DFS, and RFS reported in the literature.
Results
General Characteristics
Baseline characteristics and specifics of neck dissection of all subjects.
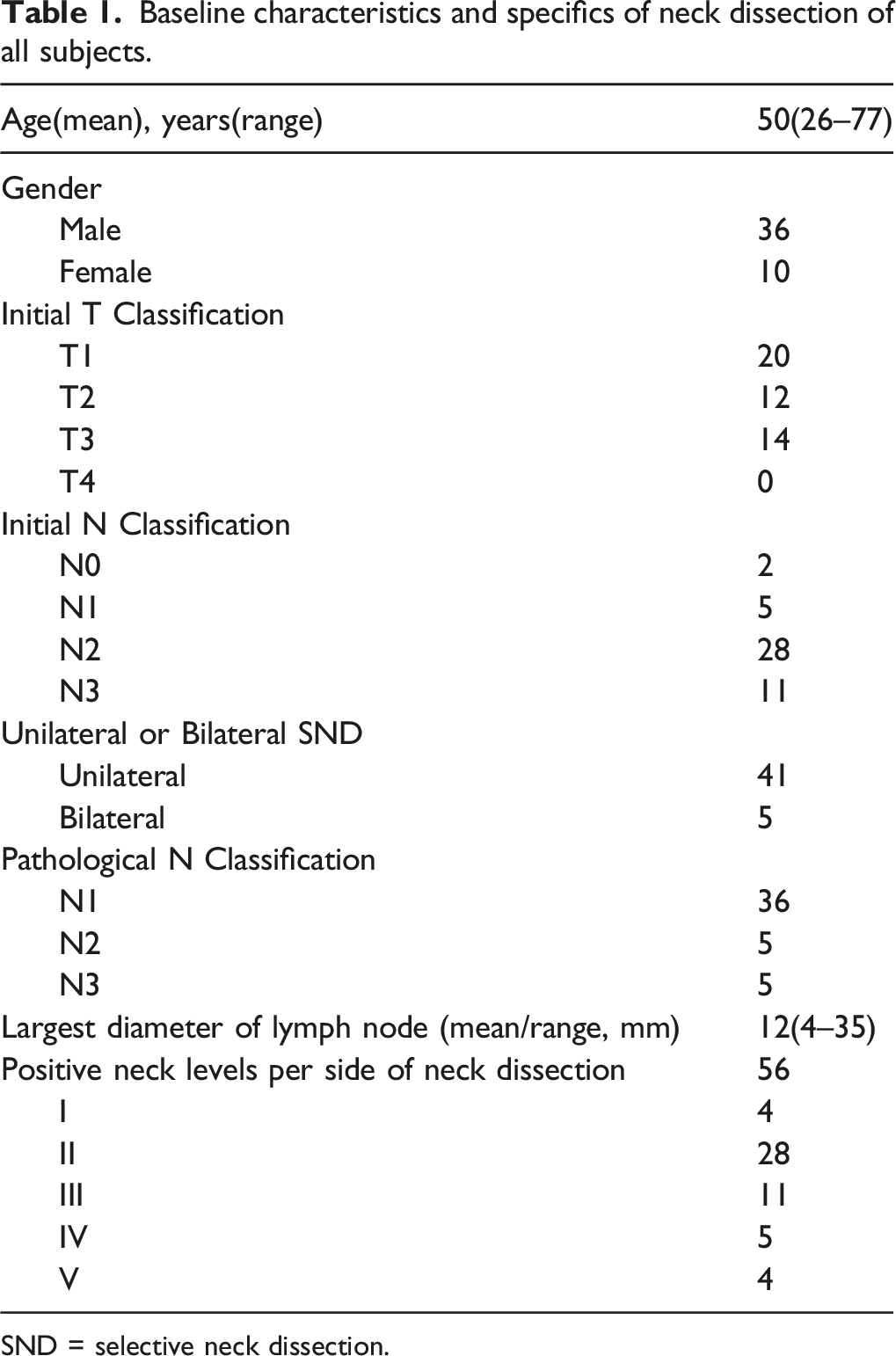
SND = selective neck dissection.
Level II was the most commonly involved cervical nodal region in 28 neck dissection specimens (54.9%), followed by level III with positive nodes in 11 specimens (21.6%). Our patients had no recurrent or residual level VI lymph nodes (Table 1).
Characteristics of post-SND locoregional recurrence and distant metastasis.
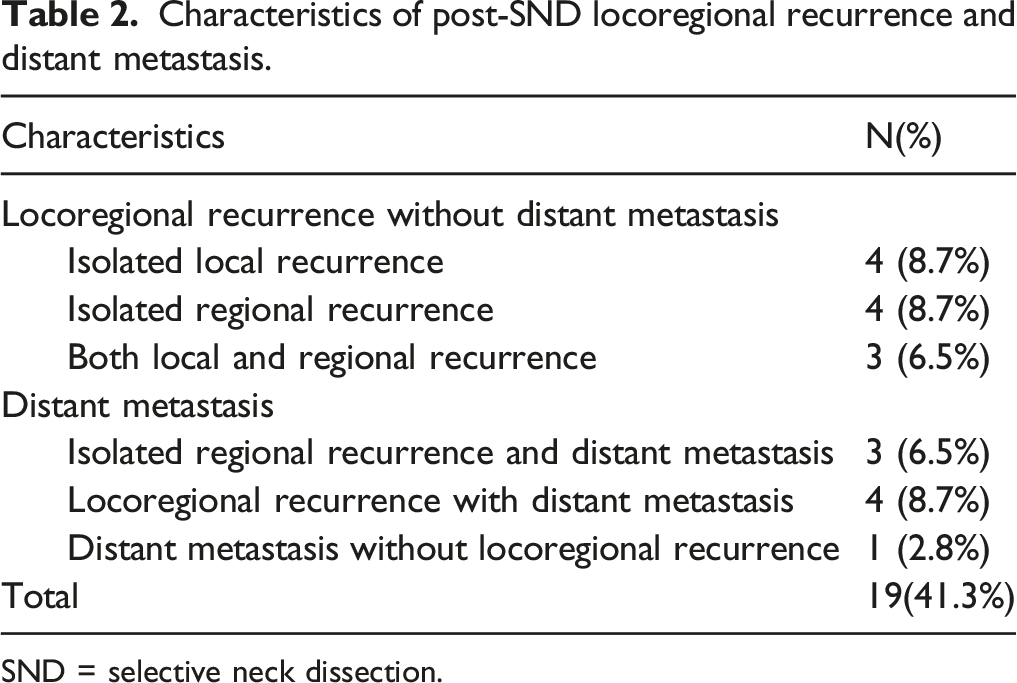
SND = selective neck dissection.
In addition, eight patients (17.4%) had post-SND distant metastasis (Table 2). Of the patients, three patients (6.5%) had both isolated regional recurrence and distant metastasis, four patients (8.7%) had locoregional recurrence with distant metastasis, and one patient (2.8%) had distant metastasis without locoregional recurrence (Table 2). Among the 7 patients (30.4%) with locoregional or/and regional recurrence with distant metastasis, only one patient (2.8%) had lymph node recurrence on the side of SND.
In our study, none of the patients died from complications of SND. One patient experienced an incision infection, and four patients reported numbness in the neck. None of the patients reported hematoma, chylous leaks, or shoulder pain.
Comparison of Our Study and the Literature for Survival Analysis at 3 Years
OS, DFS, and RFS for 3-year survival in our study and published articles.
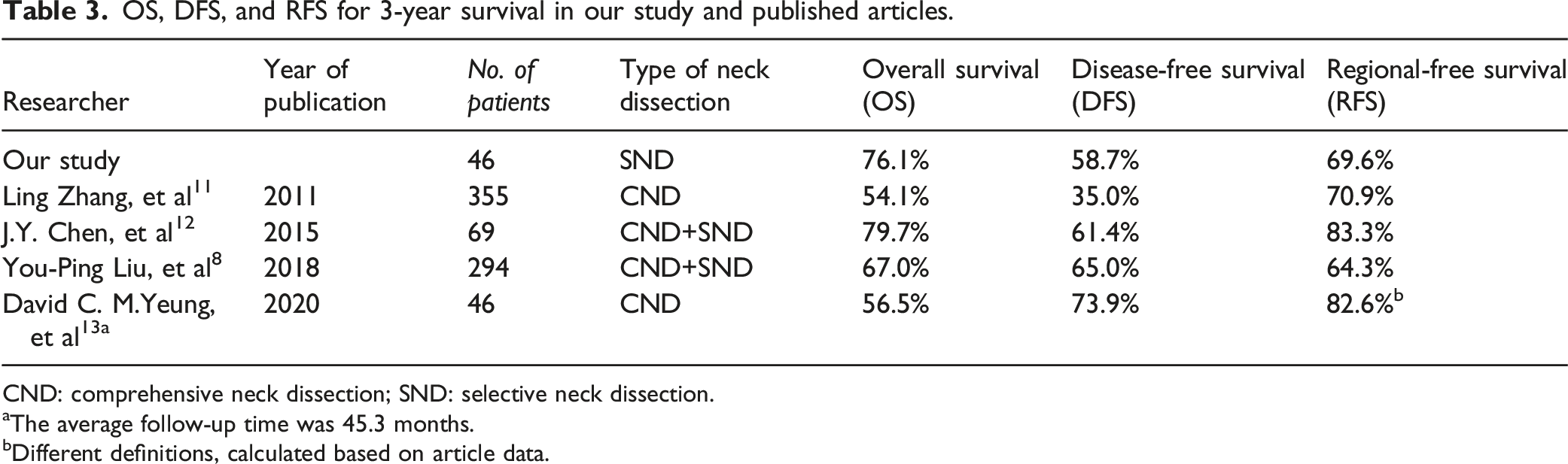
CND: comprehensive neck dissection; SND: selective neck dissection.
aThe average follow-up time was 45.3 months.
bDifferent definitions, calculated based on article data.
In 2015, J.Y. Chen et al. 12 reported that 69 patients diagnosed with neck residual disease or recurrence of NPC were assigned to undergo either RND or SND, including 51 patients in the RND group and 18 patients in the SND group. The OS, DFS, and RFS were 79.70%, 61.43%, and 83.30%, respectively, at 3 years (Table 3).
In 2018, You-Ping Liu et al. 8 reported 294 recurrent or residual NPC patients with only regional failure who underwent neck dissection, including 121 patients in the RND group and 173 patients in the SND group. The OS, DFS, and RFS were 67.0%, 65.0%, and 64.3%, respectively, at 3 years (Table 3).
In 2020, David C. M.Yeung et al. 13 reviewed 46 isolated regional nodal recurrence or residual NPC patients who underwent RND. The OS, DFS, and RFS were 56.5%, 73.9%, and 82.6%, respectively, at 45.3 months (Table 3).
In our study, the OS, DFS, and RFS of the patients were 76.1%, 58.7%, and 69.6%, respectively, at 3 years. These OS, DFS, and RFS values fell between the reported data in published articles and were most similar to the You-Ping Liu et al. 8 data (Table 3).
Discussion
NPC is a highly radiosensitive disease. IMRT has been employed to deliver an effective therapeutic radiation dose to the primary tumor and the upper neck nodes while reducing the radiation to nearby structures. 14 However, residual or recurrent disease of neck failure has been estimated to occur in 5–18% of cases. Reirradiation for neck nodes results in a high fatality rate and low treatment morbidity. Reirradiation cure rates have been reported to be only 14% to 28%. 15 Neck dissection has been recommended, but there is still a problem with how to approach the extent of surgical resection, including the choice of CND or SND and how to balance the dissection extent and minimal complications of SND.
For the monitoring of isolated regional failure after primary treatment for NPC, neck CT or MRI has been applied effectively in the detection of regional metastasis. MRI is recommended by guidelines rather than CT. However, PET-CT and, recently, whole-body MRI, which have superior sensitivities (87.3–95% and 90.9%, respectively) compared to CT (76%) or conventional MRI (78%) alone, have been applied to detect distant metastasis in NPC with good effects. 16,17 Meanwhile, some authors have reported applying ultrasound-guided FNAC. However, it is not routinely applied due to its low sensitivity of 25–70% and negative predictive value of 42.9%. 17
New lymph node metastasis of NPC progresses from the upper neck to the lower neck and from level II to level III, IV, and V, and the rate of skip metastasis is only approximately 4%. 18 Previous articles 8 and our study showed that regional metastasis also had similar transfer characteristics to new lymph node metastasis of NPC. The selection of SND is also based on the transfer characteristics of lymph nodes. Previous articles reported that SND patients experienced lower hospitalization and complication rates than CND patients. 12 Meanwhile, in our study, the OS, DFS, and RFS of the patients with SND were between the values in reported data from published articles. These articles were all retrospective studies. The number, staging, and treatment methods of the selected patients were different, so the results were different. Our study data were similar to the You-Ping Liu et al. 8 data. This might be explained by at least two considerations. First, with only regional failure NPC patients, the selected patients were similar to recurrent or residual NPC patients. Second, the dissection extent of SND was similar to the involved levels of lymph node sites and those adjacent to one or two high-risk levels. Based on the literature and our study, the results indicated that SND may be a feasible treatment procedure and that it is not inferior to CND for patients with isolated regional failure in NPC. 8,12
All the previous articles showed that the isolated regional failure of NPC was not as extensive as the primary lymph node metastasis. This phenomenon might be explained by at least two factors. First, patients with isolated regional failure were more frequently re-examined after the primary tumor was surgically removed. Second, radiation therapy weakens lymph node metastasis or invasiveness. In our study, the largest lymph node diameter was 12 mm on average. The incidence of extranodal extension was very high and was previously reported to be 67.5%∼72.5%. 8,19 Therefore, we should pay attention to not only the breadth (level) but also the depth (safe margins at the level) of neck dissection. In our center, SND is the common choice for isolated regional failure of NPC. The dissection extent of SND usually involves the levels of lymph node sites for isolated regional failure according to MRI; in addition, regarding the level II or III lymph nodes, we recommend simultaneous dissection of level II and III lymph nodes, which may not increase surgical trauma and complications. Only one patient (2.8%) had lymph node recurrence on the side of SND for locoregional recurrence without distant metastasis. Therefore, specific SND is a sufficient and effective treatment for isolated regional failure in NPC.
Regarding the limitations of this retrospective cohort study, the results may need to be validated by previous data. Second, distant metastasis is a problem that cannot be ignored and needs continuous exploration. Third, as this was a single-center study with only 46 patients, its results might have selection bias. Last, we only included patients who underwent SND, and we did not perform a comparison with CND, so we were unable to accurately define the indications and contraindications of SND. Therefore, a prospective randomized, controlled and large-sample study is needed to confirm our research findings in the future.
Footnotes
Author Contributions
Jian-Hui Wu wrote the main manuscript text and Jian-Hui Xu prepared data and tables. Fei Ye and Min-Yi Fu have participated in polishing this manuscript. All authors reviewed the manuscript.
Declaration of Conflict of Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Our study was approved by the Ethics Committee of Zhongshan City People’s Hospital (approval no. 2021055).
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.