
Abstract
Bone-Anchored Hearing Systems (BAHSs) are commonly offered as a surgical treatment for patients with conductive and mixed sensorineural hearing loss. BAHSs utilize bone conduction to transmit sounds from an external processor to a titanium implant, which is placed surgically into the cranium. This system is indicated in patients with conductive or mixed hearing loss with a bone conduction threshold better or equal to 55 dB HL or those with single-sided deafness who are not candidates for conventional hearing aids. 1
Traditional guidelines for BAHS placement recommend placing the implant approximately 50–60 cm posterosuperior to the tragus and in the horizontal line with the most superior part of the helix. Implantation requires a cranial bone thickness exceeding 3–4 mm.2,3 While these guidelines lead to effective implantation for most patients, patients with a cranial bone thickness of less than 3 mm, such as those with prior craniotomies or cranial malformations, may be at greater risk for complications. Intraoperatively, there is risk of injury to the dura mater and subsequent CSF leakage. 4 Subdural hematomas may also result from damage to the sigmoid sinus, a dangerous complication requiring immediate cranial decompression. 5 Additionally, studies suggest that smaller cranial thickness can limit the length of a fixture placement and may result in osseointegration failure.6,7 Furthermore, BAHS implantation is contraindicated in patients younger than 5 years because these patients do not typically reach a cranial thickness of 2.5 mm until 5–7 years of age. 8
In craniofacial surgeries, advances in computer-aided design have broadened applications of virtual surgical planning (VSP). In particular, CT imaging has become widely used for 3-D reconstruction and bony and soft tissue modeling. Given soft tissue structures are subject to alteration by equipment such as head stabilizers, bony models are generally preferred by surgeons in virtual planning. 9 Nevertheless, soft-tissue modeling provides utility in surgical planning for procedures which rely on soft tissue landmarks, such as those in orthognathic surgery. 10
Here, we present a novel approach to BAHS implantation, which utilizes CT-guided reconstruction of cranial thickness and bone and soft-tissue models to determine areas of appropriate cranial thickness for abutment placement.
The present perspective is based upon observations from a case of a 37-year-old female with a large encephalocele and low tegmen scheduled for a left-sided Ponto BAHS implantation in March 2022. She also had a significantly anterior and superficial sigmoid sinus. A preoperative CT temporal bone scan was used to determine areas on the cranium with the required thickness for implantation (5 mm).
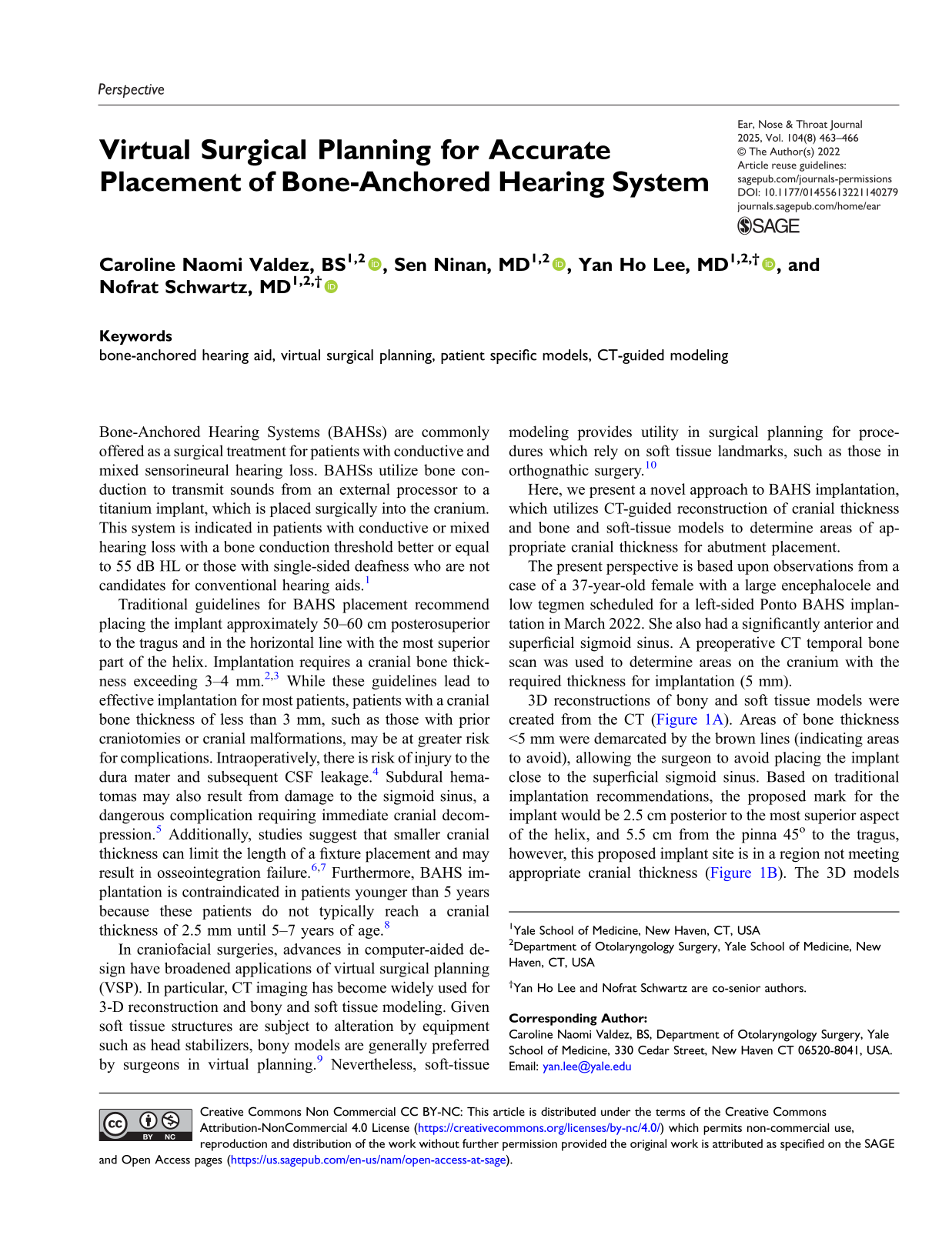
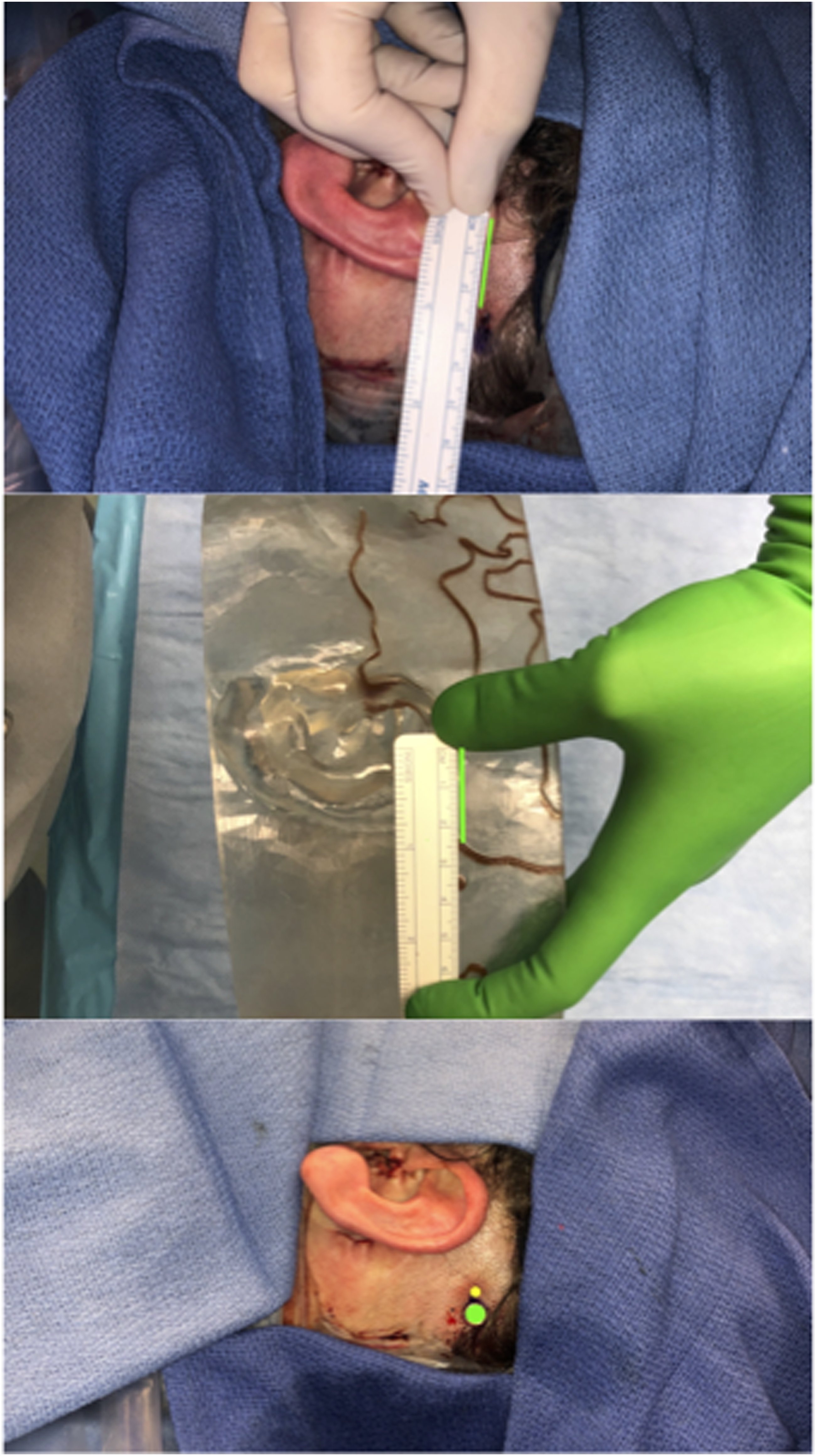
3D reconstructions of bony and soft tissue models were created from the CT (Figure 1A). Areas of bone thickness <5 mm were demarcated by the brown lines (indicating areas to avoid), allowing the surgeon to avoid placing the implant close to the superficial sigmoid sinus. Based on traditional implantation recommendations, the proposed mark for the implant would be 2.5 cm posterior to the most superior aspect of the helix, and 5.5 cm from the pinna 45o to the tragus, however, this proposed implant site is in a region not meeting appropriate cranial thickness (Figure 1B). The 3D models were used to select an alternative implantation site which was triangulated 3.5 cm from the superior auricle and 7.5 cm from the inferior auricle, safely within the area of cranial thickness of 5 mm (Figure 1C). Because the bone is not readily exposed on the surgical field, the soft tissue model allows for site markings triangulated from the superior and inferior auricle and also allows the surgeon to select an appropriate location above the pinna to avoid shadow effect. Figure 2 highlights the difference between the proposed implant site based on traditional landmarks (yellow) and the actual placement of our BAHS implant (green). Intraoperatively, there was no direct injury to the dura or sigmoid sinus during implantation. Postoperatively, there were no signs of infection at the site of abutment and no evidence of osseointegration failure. During a 4-month post-operative visit, good osseointegration and significantly improved self-reported hearing were noted. Heat-maps from preoperative CT scans (A) used to construct soft tissue (B) and bony models (C). In models, brown lines demarcate areas where cranial thickness <5 mm. Proposed implant site according to traditional guidelines using surface landmarks, measured on the patient (top) and CT-constructed soft tissue model (middle). Measurements on the soft tissue model reveal the proposed target site falls within a region where cranial thickness <5 mm. Bottom: Proposed implantation site according to traditional guidelines (yellow) and actual implantation site determined by VSP and CT-guided models (green).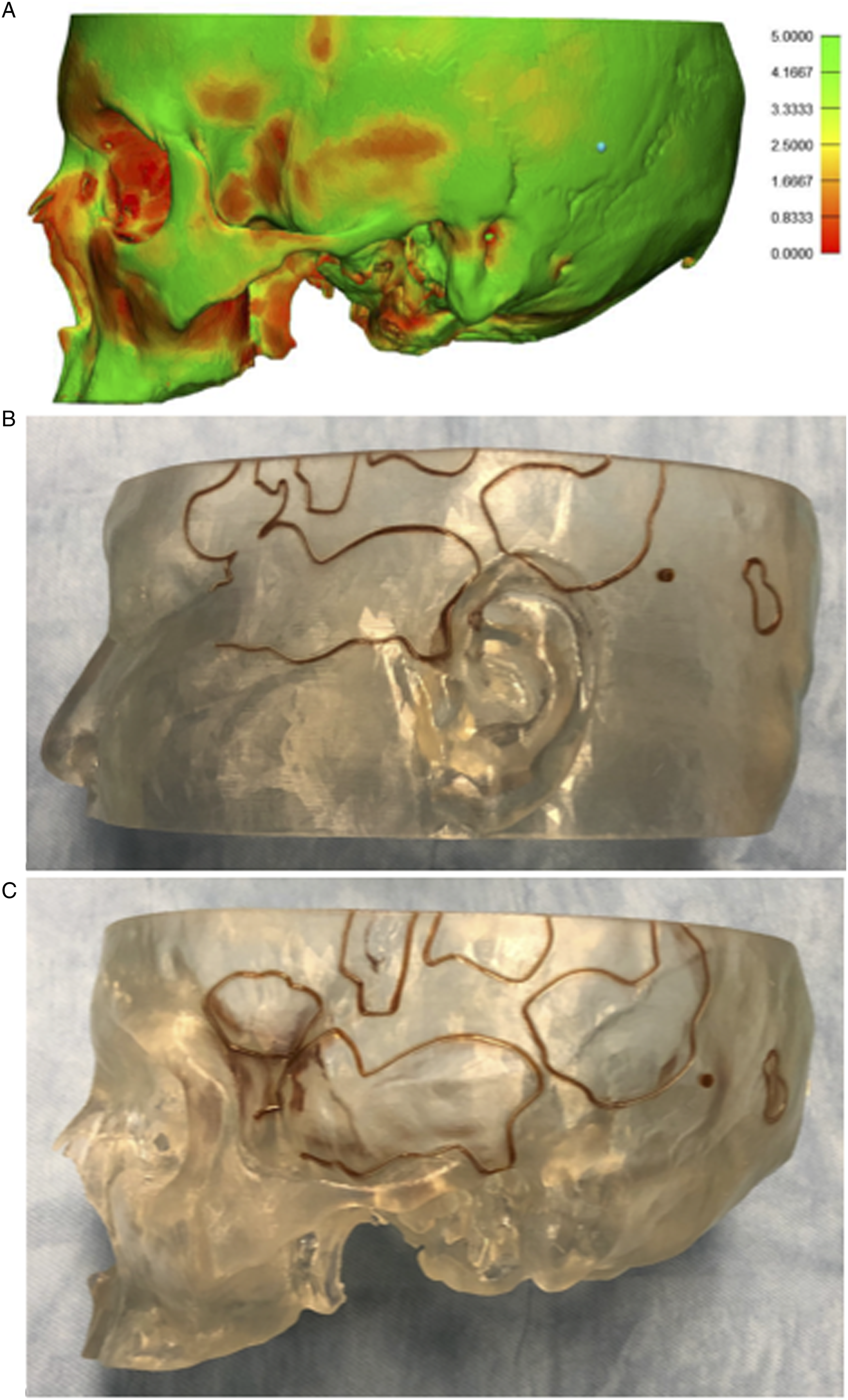
Here, we share our experience with a novel technique for BAHS implantation, using VSP to identify a target implantation abutment site where cranial thickness was greater or equal to 5 mm. This case demonstrated that after surgical site marking with surface anatomy, VSP with soft tissue and bony models led to an adjustment in implant site, resulting in successful implantation in a more suitable location. VSP allows surgeons to target areas of the cranium with appropriate skull thickness and may be used to reduce risk of intraoperative complications and osseointegration failure, particularly in patients with decreased cranial thickness or aberrant craniofacial anatomy.