
Abstract
Objective
To understand the pathogenesis of vestibular dysfunction in children and to provide a reference for the diagnosis and treatment of vestibular dysfunction in children.
Methods
A retrospective analysis was conducted on 80 children who visited our hospital from June 2011 to July 2020, aged between 4 and 17 years, with a duration of 1 day to 3 years. They were admitted to the hospital for treatment upon vestibular function-related examinations confirmed that there was peripheral vestibular function impairment.
Results
Children aged 6–12 years old who are diagnosed are significantly more than other two age groups (4–6) and (12–17) (X2 = 101.738, P < .001). There was a significant statistical difference (X2 = 91.195, P < .001) in comparison of abnormal rates of vestibular function-related examinations. The Mann test had the highest abnormal rate and the lowest Cervical Vestibular Evoked Myogenic Potential (cVEMP) abnormality rate. Comparison of abnormal consistency rates for quantitative and qualitative examination of vestibular function, the abnormal rates (double temperature test and Mann test) were significantly better than other abnormal consistency rates, and there were statistical differences (X2 = 7.485, P = .024 < .05). Among the children with vestibular dysfunction, the etiology was most common in 58 cases (72.50%) of benign paroxysmal vertigo, 4 cases of vestibular migraine (5.00%), 8 cases (10.00%) of vestibular neuronitis, of which 22 cases (27.50%) were combined with other diseases, and the most common was 15 cases (18.75%) of sinusitis.
Conclusion
A limited number of studies were conducted on vestibular dysfunction in children. The current retrospective analysis suggests that age, gender, and side of ear pain have no significant effects, while children aged 6–12 are more likely to suffer from vestibular dysfunction. On children’s vestibular dysfunction, more etiology is unclear, and special attention should be paid to differential diagnosis when giving treatment and the child’s medical history should be examined in detail and appropriate vestibular function tests should be selected in order to provide timely, effective, and accurate treatment for the child.
Introduction
The human body mainly relies on peripheral receptors such as vestibular perception, vision, and proprioception, to feel the position of the body, movement, and external stimuli. The body maintains its own position in the space through the integration and processing of balanced central information and mutual coordination. In the peripheral system above, the vestibular system is a set of precision operating systems for perception and control balance, which performs functions such as motor perception, gaze, and limb balance, and it also participates in cognitive functions such as emotion and memory. Studies have shown that disabilities associated with inner ear dysfunction, especially those with acute inner ear dysfunction, also contribute to a higher incidence of anxiety and depression. 1 Sensory impairments associated with the inner ear not only have an impact on mental health, this illusion of movement brought by it also carries physical risks. When the vestibular is stimulated, it can have a certain impact on other functions of the human body, and patients with vestibular dysfunction manifest imbalance, blurred vision, and vertigo. These symptoms lead to severe social and behavioral disorders, which in turn affects daily activities. 2 children are not able to describe their vestibular symptoms as accurately as adults do. It is commonly observed in children that dizziness with nausea, vomiting, and/or pallor, but without impaired consciousness were self-reported by children and their parents. 2 Vestibular dysfunction can lead to severe delayed motor function development. Inoue et al 3 studies have found that children with vestibular dysfunction typically learn to sit, walk, stand, and hold their heads relatively late compared to their peers without vestibular injury. Therefore, the early detection and diagnosis and treatment of children’s vestibular dysfunction is critically important. The current study is going to preliminarily discuss the clinical pathogenesis characteristics, simple, and reliable diagnosis and treatment methods for children with vestibular dysfunction so as to provide a future reference for the diagnosis and treatment of children’s vestibular dysfunction.
Materials and Methods
Ethical Considerations
This study was approved by the hospital ethics committee.
Clinical Data
Retrospective analysis of children who were hospitalized in our department from June 2011 to July 2020, with dizziness as the first complaint, and after neurology, ophthalmology, and our department vestibular examination, auditory assessment, and if necessary magnetic resonance imaging, to exclude other central balance disorders.
(1) Inclusion criteria for children, 1) The age of the patient < 18 years old; 2) Have the ability to move independently, no intellectual disability; 3) No history of major head trauma, physical deformities, or serious medical diseases; 4) Neurologic examination and brain MRI to exclude intracranial lesions; 5) Diagnostic criteria for vestibular function examination (meet at least two positives below), 4,5 ①Vestibular quantitative test I Double temperature test In the double temperature test, the child lies on his back, the head is raised about 30°, the air is injected into the ear canal, the response is observed after 60 seconds of air perfusion in each ear, the infrared video blindfold is applied to detect eye movement after perfusion, and continue to detect after the perfusion is completed for 60 seconds. The double temperature test, which takes approximately 20 to 25 minutes to complete, evaluates the low-frequency (.003 Hz) function of the horizontal semicircular canal and superior vestibular nerve. Two important results of the double temperature test, temperature reduction, and dominance bias. Temperature attenuation is a comparison of left and right reactions after perfusion (cold and heat). The dominant bias is the comparison of left-right stunt after perfusion. For each comparison, the slow phase angular velocity of the nystagmus after each perfusion is substituted into the formula proposed by Jongkees et al. Most laboratories use 20% to 30% as a criterion for judging temperature attenuation and dominance bias, and this experiment defines greater than 20% as abnormal. II Oculogenic Vestibular Evoked Myogenic Potential (oVEMP) In the oVEMP test, the patient is supine and stares upwards at a fixed target, with the ground electrode placed on the patient’s forehead, the reference electrode on one side of the nose or jaw, and the recording electrode on the middle and middle of the suborbital midline. Pulse stimulation is performed with a pure tone of 500 Hz air conduction at a stimulation intensity of 90 dB SPL with a stimulation duration between 4 and 10 milliseconds, at least 100 to 150 stimuli are given, and two repeat trials are performed. III Cervical Vestibular Evoked Myogenic Potential (cVEMP) In the cVEMP test, the patient is supine and points the tip of the nose towards the ceiling to raise the head, or the head can be turned to the non-stimulating ear side, the ground electrode is placed on the patient’s forehead or jaw, the reference electrode is placed on the sternum, and the recording electrode is placed on the myofibral abdomen of the sternocleidomastoid muscle. The main parameters of cVEMP and oVEMP include incubation period, amplitude, and threshold, which refers to the time when p13/n23 and n10/p16 peaks occur in cVEMP and oVEMP, respectively; Amplitude is the absolute difference between the peak amplitude response of cVEMP at p13 and n23 and the peak amplitude response of oVEMP at n10 and p16, and the asymmetric ratio of the left and right ear amplitudes is calculated, and in most cases, the difference between the left and right ears is greater than 40%, so this experiment will be greater than 40% defined as abnormal. ② Vestibular qualitative test I Romberg test It is a method used to check whether the vestibular balance function is normal. The subject is upright, with his feet together, his upper limbs sagging, his eyes closed and upright for 30 seconds, or he can clasp his hands together in front of his chest and pull them to the sides to observe whether the subject is standing unsteadily or falling. In peri vestibular lesions, the trunk is tipped in the direction of the destruction of the vestibular, consistent with slow nystagmus; In central lesions, the direction of trunk dumping is inconsistent with the slowness of the nystagmus. II Mann test Bipedal station in a straight line on the heel to the toe, closed eye station for 30 seconds, called Mann test. This method is more bipedal and sensitive, and the conclusion is similar to Romberg’s test. All patients have undergone these tests and worked with each other to identify the lesion side.
(2) Exclusion criteria for children, 1) Limb deformities cannot move independently; 2) The vestibular is not developed; 3) Central diseases; and 4) Poor compliance and inability to cooperate with treatment.
(3) Criteria for Withdrawal of Children, 1) Failure to Receive Treatment and Regular Review as Required; 2) No Longer Meet the Selection Criteria; and 3) Auto Quit.
Statistical Methods
IBM SPSS Statistics for Windows, Version19.0 (IBM Corp., Armonk, NY, USA) was used to statistically analyze the age, gender, vestibular function examination, and etiology of the children. The measurement data was represented by (X±SD), and chi-square test is used for data analysis (inspection level P = .05).
Results
Comparison of General Conditions of Children
Of the 80 children with impaired peripheral vestibular function and hospitalization, including 44 males and 36 females, aged 4–17 years (average 9.58 ± 3.19 years), the duration of the disease was from 1 day to 3 years. The ratio of male to female among the children was 44 and 36(X2 = 1.600, P = .206 > .05), no obvious statistical difference. 40 cases (50%) of the left ear, 32 cases of the right ear (40%), 8 cases of both ears (10%), there was no obvious difference in the prevalence of left and right monoaural (X2 = 1.778, P = .182 > .05), single ear accounted for the vast majority, and there was a statistical difference (X2 = 102.400, P < .001). 5 cases (6.25%) in preschool age aged 4–5 years, 61 cases (76.25%) in primary schools aged 6–12 years old, and 14 cases (17.50%) in middle schools aged 13–17 years old. There are significantly more children aged 6–12 years in primary school than children in the other two age groups and there are statistical differences (X2 = 101.738, P < .001).
Comparison of Abnormal Rates of Vestibular function-Related Examinations
Comparison of Abnormal Rates of Vestibular Function-Related Examinations.

Comparison of Abnormal Consistency Rates on Quantitative and Qualitative Tests for Vestibular function
Comparison of Abnormal Consistency Rates on Quantitative and Qualitative Tests for Vestibular Function.

Characteristics of the Disease in Children
Proportion of children with confirmed causes (see Figure 1), including 15 cases of sinusitis (18.75%), 3 cases of anxiety (3.75%), and 1 case of asthma (1.25%). Except for 1 case of co-anxiety disorder and refusal of anti-anxiety treatment, the symptoms of the remaining children were gradually and completely alleviated through treatment. Proportion of diagnosed causes among children (n = 80).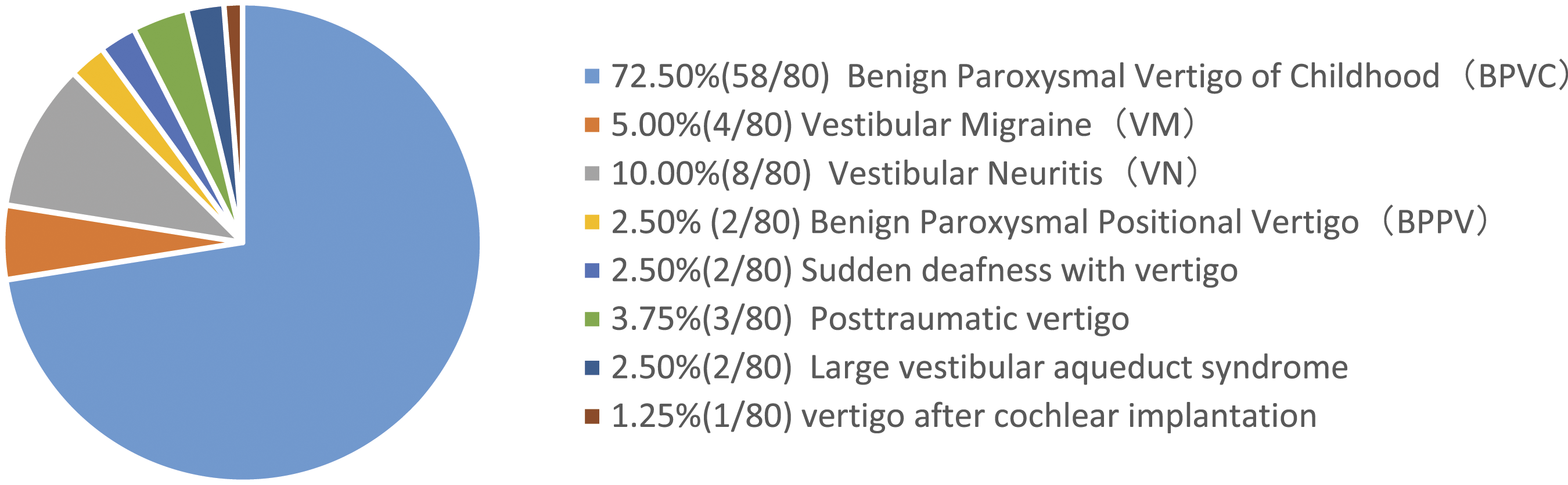
Discussion
Because of the co-existence of auditory and vestibular lesions, extensive neonatal hearing screening programs have raised awareness of vestibular disease in children. In the United States, 2 to 3 out of every 1000 babies born each year have hearing impairments, and 20 to 70% of them have vestibular nerve defects. 6 The prevalence of child balance and vestibular dysfunction is estimated to be between .45 and 5.3%, with a slightly higher prevalence in women than in men and increasing with age. 7 In this study, the prevalence of vestibular dysfunction in children aged 6-12 years in primary school was significantly higher than that in children of the other two age groups, and the difference was statistically significant., This may result from that children aged 6–12 years can clearly describe their symptoms, actively seek medical attention According to Basser’s original description, vestibular symptoms begin before age 4 and resolve spontaneously between the ages of 8 and 10, 8 so the prevalence after age 10 years is on a downward trend, which is consistent with the results of the current study. Some studies have shown greater intellectual and endocrine changes between the ages of 15 and 18 years, with more common incidence in boys than in girls, 9,10 and this study also found that the prevalence of boys was slightly higher than that of girls (55% and 45%), but there was no significant statistical difference, which may be only 17.5% of the children over 13 years of age included in this experiment, and the related vestibular dysfunction is more common in single ear disease (90%), and the cases of both ears affected constitute around 10%, while the prevalence of left and right ears is not statistically significant.
Childhood vertigo disorders are divided into unknown dizziness, peripheral vestibular dysfunction, and central balance dysfunction—three categories the prevalence of vestibular nerve injury in children is difficult to accurately assess due to its symptoms are nonspecific. The differential diagnosis of vertigo in children is different from that in adults because some causes are specific to children and the diagnosis depends on the age range of the test patient and the available vestibular testing techniques, which are often misleading, so most children are diagnosed with unidentified dizziness. It can be seen that the systematic comparison of corresponding vestibular function tests can assist in diagnosis and improving diagnostic accuracy has become a key point in the diagnosis and treatment of children’s vertigo disease. The double temperature test is used to evaluate the function of the horizontal semicircular canal and the superior vestibular nerve, which is considered the gold standard for functional testing of the peripheral vestibular system. This study found that in the children’s vestibular examination, the abnormal rate of the Romberg test was only 53.75%, while the abnormal rate of the Mann test was 83.75%, so the child’s examination should be mainly based on the Mann test, and the child’s vestibular balance disorder could not be simply excluded because the Romberg test was normal. And the abnormal rate of the Mann test is basically equivalent to the double temperature test, which is better than other vestibular examination items, and the most important goal of the vestibular nerve assessment may be to have the child cooperate with the entire test, rather than trying to do as many different tests as possible. 6 Therefore, the Mann test, which is convenient and flexible, is not limited by examination equipment and is more suitable for application in clinical clinics, bedside and grass-roots units that lack corresponding examination equipment.
According to the characteristics of vestibular nerve anatomy and vestibular function examination, one or two abnormalities of the double temperature test or oVEMP are presumed to be supra vestibular nerve abnormalities, only cVEMP abnormalities are speculated to be vestibular nerve abnormalities, and cVEMP abnormalities and cold and heat tests or oVEMP one or both abnormalities are speculated to be vestibular total nerve abnormalities. Our study found that the abnormal consistency rate of the double temperature test and the Mann test was significantly higher than the abnormal consistency rate of the vestibular induced myoelectric potential and the Mann test. The possible reasons are as following. 1) age, difference, inability to maintain sufficient muscle contraction, electrode intolerance, restless sound stimulation, and other factors may affect the application of veMP test in children, while the double temperature test is simple to operate and can provide specific low-frequency information about the vestibular nerve and horizontal semicircular canal, so the abnormal rate of double temperature test is better than vestibular induced myosteriostatic examination abnormalities; 2) The probability of lesions affecting the vestibular nerve is higher than that of the inferior vestibular nerve and the vestibular pansen nerve. 11,12 The assessment and management of vestibular neurological disorders in children has received increasing attention. Age-appropriate vestibular function tests improve differential diagnosis and thus guide medical care and rehabilitation. However, there is no single area of specialization that alone can provide the best treatment, and clear communication across multidisciplinary teams can improve the management efficiency of children with vestibular disorders.
Vertigo and dizziness can present in children as migraine, neurological, intestinal, ophthalmic, or vestibular lesions. 13 The causes of vertigo and dizziness in children are multidisciplinary, and the most common causes are suggested to be benign paroxysmal vertigo (BPVC) and vestibular migraine (VM) in children. 14 BPVC is considered an early manifestation of VM and is recognized by the International Headache Classification (ICD-2). 15 In a study of 2726 children with vertigo, VM, BPVC, and labyrinthitis, vestibular neuritis accounted for the majority of children with vertigo, 16 and this group of studies also found that BPVC was the most proportion. Its characteristics are as following. 1) without any precipitating and aura of sudden dizziness, with or without visual rotation, there may be a feeling of head swelling, lasting for several minutes or hours, can heal gradually after self-healing or taking medication, repeated seizures, intermittent period of several days, months, and may have a continuous feeling of dizziness. 2) During the attack period, there may be autonomic symptoms such as nystagmus, nausea, vomiting, sweating, and pallor. 3) A small number is accompanied by tinnitus, and most of them have no hearing loss. 4) Vestibular function is damaged to a certain extent, walking has feet floating, unstable, running and jumping is easy to fall. Children with inferior vestibular function suggest organic changes in the inner ear, and the disappearance of vertigo symptoms is mainly dependent on the compensatory capacity of the vestibular system, and the recurrence rate after decompensation increases. The main purpose of our study is to compare the causes of dizziness in children under 18 years of age admitted to the Department of OTOL in our hospital, and to describe the clinical overview, investigation, and diagnosis of these children so as to provide certain reference value for clinical work diagnosis and treatment.
The differential diagnosis of vertigo in children is different from that in adults because some causes are specific to children, while common pathologies occur very differently in children and adults. In adults, about 70% of BPPV cases are idiopathic BPPV, and the remaining cases are called secondary BPPV. Risk factors for BPPV include chronic otitis media, head trauma, prolonged bed rest, and osteopenia and osteoporosis. 17 In this study, there were 2 cases of primary incidence and 3 cases of secondary disease. Choi et al found that pediatric BPPV is a relatively rare cause of childhood vertigo, with a high incidence and recurrence of related diseases. 18 BPPV is relatively rare in children in this study than in adults, and the main causes are related to inner ear disease and recent head trauma.
Diagnosing vertigo in children is an art that requires experience, knowledge, and accurate clinical sensitivity to determine the neurological, cardiological, or psychiatric cause of a child’s dizziness. 19 Because affected children are unable to properly characterize the symptoms they experience, clinicians may not be able to make an accurate diagnosis, especially in very young children. In addition, the differential diagnosis of pediatric dizziness is extensive, so correct diagnosis requires comprehensive otological examination as well as neurological and general examination. Also, clinical and neurophysiological vestibular tests are not necessarily reliable in young patients. 20 As a result, clinicians often find it difficult to establish an appropriate diagnosis in these cases and delays or misdiagnoses are common. 21
Children with sinusitis and dizziness should be conducted vestibular function tests. Children with vestibular disorder are mostly dizzy in the morning and the symptoms are more relieved after exercise, and in the afternoon, the dizziness is aggravated after improper exercise, after a long period of quiet lying, and after watching animations. In addition to nasal congestion and purulent discharge, patients with sinusitis are mostly based on headaches and head weight, with a certain time pattern, the symptoms are alleviated significantly after medication, and there is no abnormality in exercise. It is suggested that attention should be paid on differential diagnosis. Among the children in this study, there were 6 cases of dizziness. Three cases suffering from dizziness are complicated by anxiety disorders and were treated with psychiatric intervention at the same time with treated vestibular disease. One patient recovered vestibular balance after treatment, but the anxiety disorder improved poorly and he dropped out of school. A child with vestibular dysfunction caused by trauma in one patient developed severe walking difficulties, and the vestibular training for 3 months gradually resumed normal walking. It is worth noting that in this study, there was 1 case of a child with dizziness after electronic cochlear implantation. However, the sample size was small. With the popularity of electronic cochlear implantation, cases of dizziness in children should be given higher priority and early intervention.
A single vestibular function test cannot determine the lateral differentiation of the child’s vestibular dysfunction, and vestibular nerve damage can lead to a series of cognitive, psychological, and somatic symptoms, and can be derived from a wide range of medical reasons, and the diagnosis of another child needs to be confirmed by combining his or her detailed medical history, clinical manifestations, and qualitative and quantitative examination of the vestibular and cannot be concluded based on the results of a single examination item alone. Therefore, medical staff dealing with pediatric vertigo cases should ask in detail about the patient’s medical history, select the appropriate and accurate examination, the necessary vestibular function examination, as well as assessment to determine the lateral differentiation to make a correct diagnosis. If necessary, multidisciplinary cooperation to diagnose are suggested to treat related concomitant diseases. Generally, children who undergo standardized treatment can basically get a cure.
In this study, the standard was less than 18 years old, and the age span of the children is large, and there are many factors involved in the composition and distribution of the etiology, which may lead to biased research results. Vestibular function examination technology is much less accepted in children than in adults, and the influencing factors are parents' concerns and children’s non-cooperation, so it is necessary to give priority to the simple operation and high accuracy of the test method. Another limitation of the study is that all children with vertigo were not subjected to an additional objective vestibular test—the Video Head Impulse Test (vHIT). As noted by Okumura et al, 22 it is very difficult to detect nystagmus on examination for a limited time, as only 2 of the 68 children they evaluated successfully detected pathological nystagmus in paroxysmal vertigo. As this study is retrospective, the method was introduced by MacDougall et al (2016), and so far, there has been no indication of whether they are suitable for children and how much normal value might be. 23 The above are to be carried out for multi-center, large sample case data, subdivided and accurate research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Foundation: Health Science and Technology Project of Hangzhou city (A20200381).