
Abstract
Papillary thyroid carcinoma (PTC) is prone to regional lymph node metastasis, which is more common in central lymph nodes and lateral cervical lymph nodes, and retropharyngeal lymph node metastasis (RLNM) is extremely rare. A male with PTC presented with extensive cervical lymph node metastasis and the initial RLNM. After full evaluation by preoperative imaging examination, the patient underwent total thyroidectomy + left central lymph node dissection + left neck lymph node dissection (II III IV V) + left retropharyngeal tumor resection, and the postoperative recovery was good without recurrence long-term complications, and no local recurrence and metastasis were found during one-year follow-up.
Introduction
Papillary thyroid carcinoma (PTC) is a common endocrine carcinoma of the head and neck. PTC is prone to local lymph node metastasis, rates from 30 to 80%. 1 The first station of preference for lymph node metastasis in PTC is the central lymph node, followed by the lateral cervical lymph node (level II, III, IV, and V). According to reports, the incidence of retropharyngeal lymph node metastasis (RLNM) in differentiated thyroid carcinoma is 0.43–0.5%.2-6 However, RLNM associated with differentiated thyroid carcinoma often present as recurrent or persistent disease, and the initial RLNM is rare. 4 So this article present a case of PTC with initial RLNM, and a literature review, in order to get a better clinical guidance.
Case Presentation
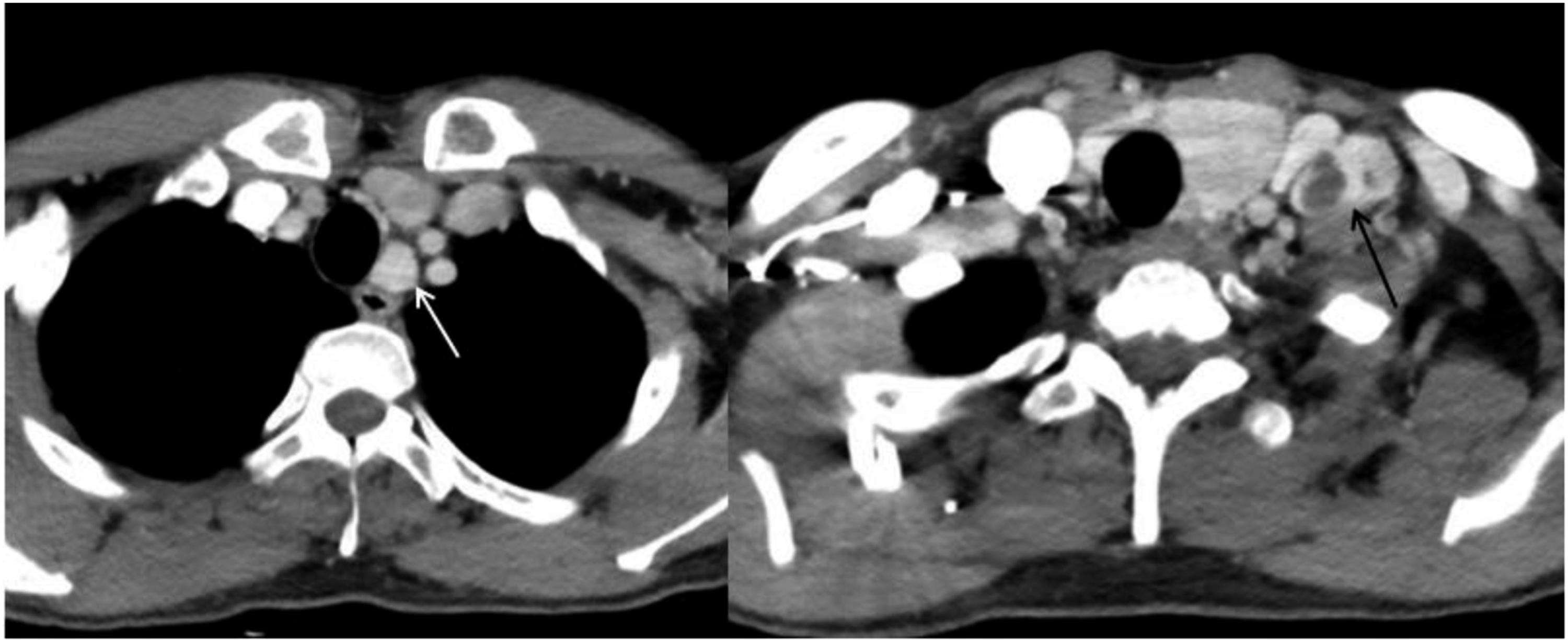
A middle-aged male came with “neck mass,” which was found unintentionally 11 days ago, without redness, swelling, heat, pain, hoarseness, dysphagia, dyspnea, and other symptoms. Physical examination showed that the neck was soft, the trachea was in the center, and the left lobe of the thyroid gland could be palpated with a mass of about 3.5×3.0 cm in size, which is hard, with unclear borders, and moves up and down with swallowing. Multiple enlarged lymph nodes were touched in the left neck, with a large diameter of about 3 centimeters, hard texture, and unclear boundary. The doppler ultrasound was performed, showing an approximately 6 cm diameter mass in the left lobe of the thyroid (Ti-RADS was grade 5), and enlarged lymph nodes in level II, III, IV, and VI with calcification and structural abnormalities. Ultrasound-guided fine needle aspiration biopsy pointed an atypical follicular epithelial cell changes in the left thyroid nodules, the lymph nodes in level II of the left neck showed a small number of lymph node cells and a very small number of stained and enlarged bare nuclear cells. Enhanced computed tomography(CT) of the neck showed a mass in the left lobe of thyroid and extensive lymphadenopathy with partial fusion in level II, III, IV, and V of the left neck, and isolated enlarged lymph node was seen in the retropharyngeal space near the subhyoid level(Figures 1 and 2). Enhanced CT showing retropharyngeal lymph node enlargement. Enhanced CT showing extensive lymph node enlargement in the central region and lateral neck.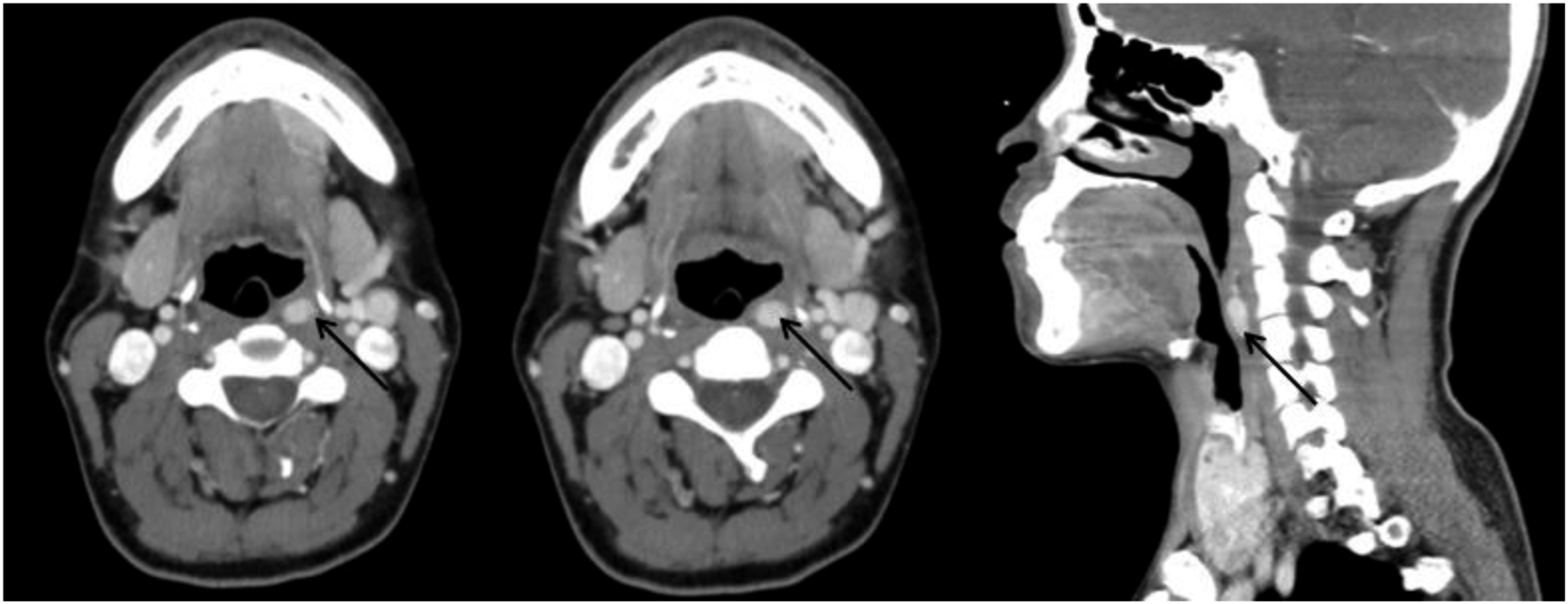
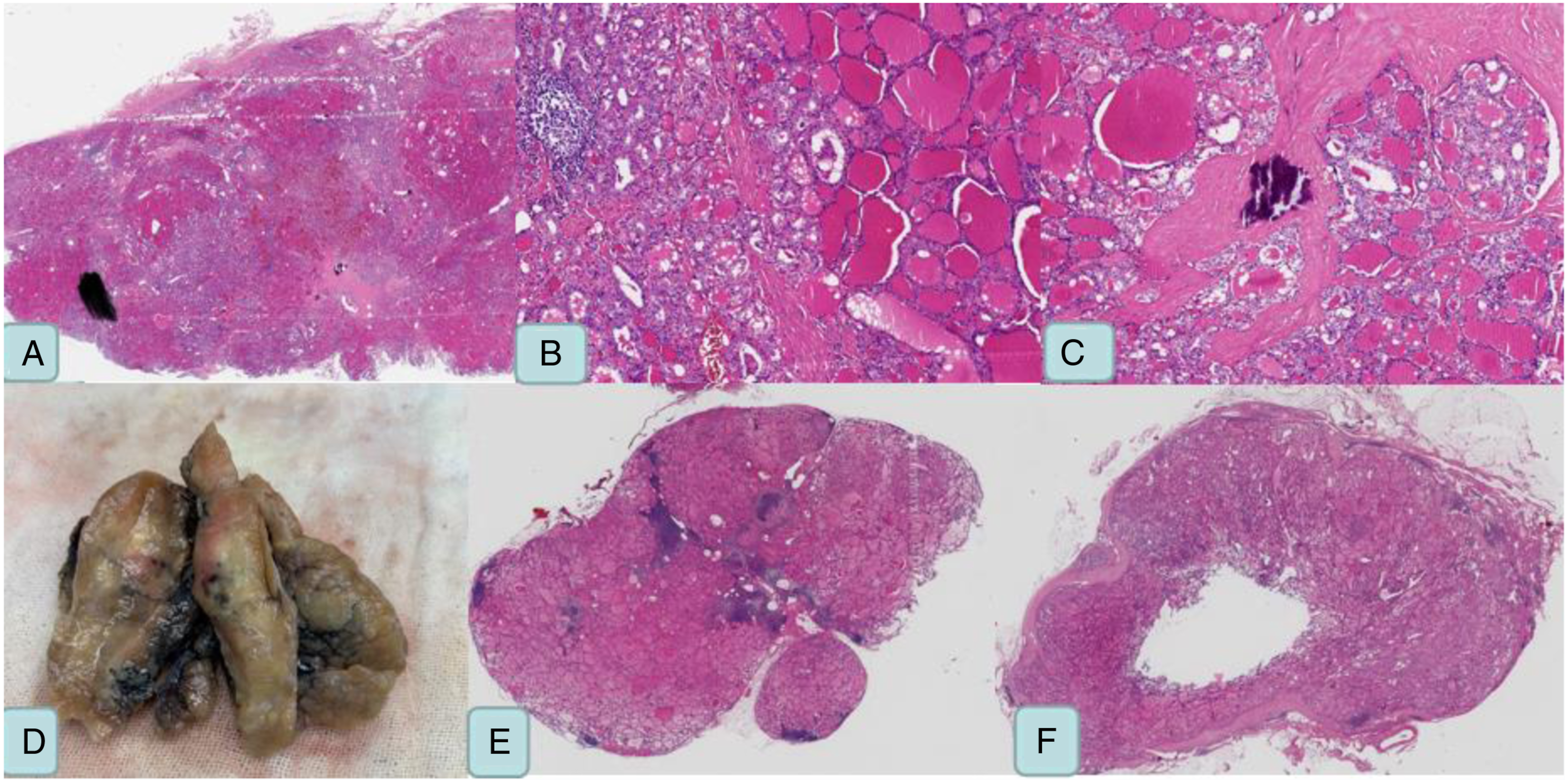
After completing the examination and exclusion of contraindications, the surgery with total thyroidectomy + left central lymph node dissection + left neck lymph node dissection (II III IV V) + left retropharyngeal mass resection was performed under general anesthesia (Figure 3). Postoperative pathology indicated PTC (Figure 4ABC) with lateral cervical lymph node metastasis (Figure 4E) and RLNM (Figure 4F). The patient developed swallowing discomfort after surgery, which disappeared 3 months later. There was no tumor recurrence or metastasis observed during one-year follow-up. (A) The central lymph nodes are closely adherent to the recurrent laryngeal nerve. (B) Resection of retropharyngeal lymph nodes and sublingual nerve. (A, B, C) papillary carcinoma. (D) pathological specimen of primary thyroid carcinoma. (E) lateral cervical lymph node metastasis of papillary carcinoma. (F) papillary carcinoma with retropharyngeal lymph node metastasis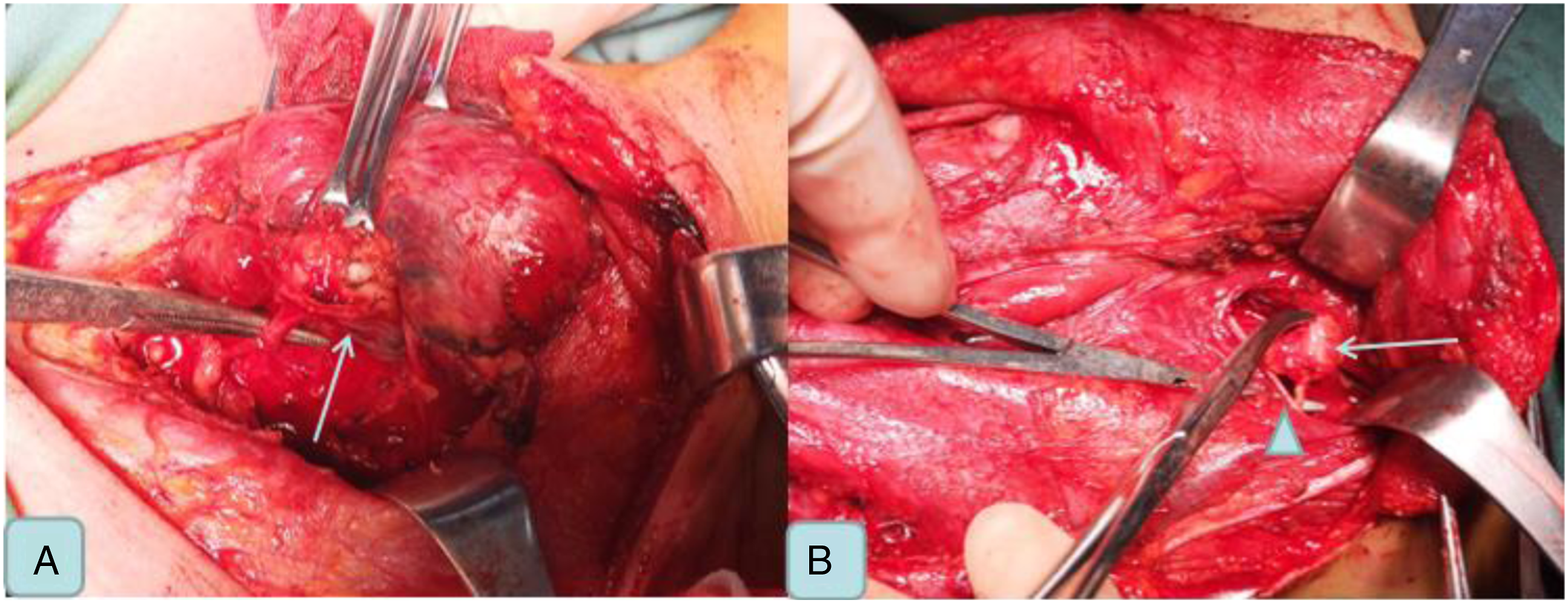
Discussion
The retropharyngeal space was first described by Grodinsky M. 5 The posterior upper part of the deep cervical fascia covers the buccal muscle and pharyngeal constrictor, which is called the pharyngeal buccal fascia. The posterior part of the deep cervical fascia and pharyngeal buccal fascia forms the retropharyngeal space. 8 RLNM of PTC is rare, 9 mostly manifested as recurrent or persistent diseases, and the initial RLNM was quite rare. 8 And this case belongs to the latter (Figure 1).
It has been widely accepted that retropharyngeal lymph nodes are collateral pathways of lateral cervical lymph nodes in thyroid cancer.10-12 This explains why RLNM is common in patients with extensive lateral cervical node metastasis or with a history of neck dissection. Robbins.et al 13 reported that the lymphatic vessels of the superior thyroid pole were directly identical to the lymphatic vessels of the retropharynx, and lymph nodes near the superior thyroid pole could directly diffuse to the retropharynx lymph nodes, which was anatomic variation, accounting for about 20%. 14 Our case followed the first theory (Figure 2).
Imaging diagnosis of RLNM of thyroid cancer mainly relies on PET-CT, enhanced CT and enhanced MR, while Doppler ultrasound is rarely used for its diagnosis.8,15 Sometimes laryngoscopy can also reveal retropharyngeal masses. 9 There is no literature report on doppler ultrasound-guided fine needle aspiration and thyroglobulin eluate examination to assist in the diagnosis of RLNM. Mostly, patients with recurrent PTC with RLNM have no clinical symptoms, while the initial metastasis can be manifested as tonsillar enlargement, snoring, or pharyngeal discomfort. 9 Retropharyngeal lymph nodes were detected by enhanced CT in our patient, which was pathologically confirmed as RLNM of PTC after surgical resection. However, no clinical symptoms of retropharyngeal lymph nodes were observed.
The management of differentiated thyroid cancer is unclear and the 2015 American Thyroid Association guidelines do not address the management of retropharyngeal lymph nodes. 16 There are 3 treatment options for PTC with RLNM: observation, non-surgical treatment, and surgical treatment. PTC usually exhibits a chronic and inert biological behavior. Therefore, Victoria Harries MBBS.et al 8 suggested that RLNM associated with small-diameter, non-progressive differentiated thyroid cancer was appropriate to observe. In their study, 25 patients were selected for observation with a median follow-up of 28 months (range from 2 to 182 months). Finally, 19 patients (76%) had a local recurrent disease and 6 patients (24%) had the distant disease, and no disease-specific deaths. Non-surgical treatment mainly includes radioiodine therapy, external irradiation therapy and systemic therapy. Non-surgical treatment is an option for patients with distant metastases. In the study of Victoria Harries MBBS, 13 patients were opted for non-surgical treatment, of whom 10 had been co-existing local recurrence disease at diagnosis time, 6 had been co-existing distant metastasis at diagnosis time, 3 had tumor disappearance after treatment, and 7 had significantly the shrink of the tumor diameter after treatment. 8 And, retropharyngeal lymph nodes dissection is the most recommended treatment for RLNM of PTC.17,18 Surgical treatment of retropharyngeal lymph nodes was first proposed by Ballantyne. 19 The methods of retropharyngeal lymph node dissection mainly include cervical approach and transoral approach. The transcervical approach also includes direct transoral approach, transoral approach assisted by endoscopy, and robotic transoral approach. Victoria Harries MBBS et al. reported 27 patients underwent surgical treatments, including 19 patients underwent cervical resection and 8 patients underwent oral resection and including 6 patients underwent robotic transoral approach. Among the different approaches, the most common complication was swallowing discomfort, accounting for about 25%. In one case, the hypoglossal nerve was damaged. 8 Our patient only experienced swallowing discomfort, which disappeared after about 3 months. Thomas Shellenberger et al. reported 3 cases of RLNM through an oral approach, confirming that the method is feasible, minimally invasive, and safe. 20 For isolated PTC with RLNM, lymph node resection is limited and regional control can be achieved. Endoscopic resection of retropharyngeal lymph nodes is rarely recommended due to the small operation space and inconvenient operation, and robotic resection is preferred. Goepfert et al. proposed that robot-assisted methods provide a safe and effective dissection in tight Spaces with their visibility and flexibility, but the disadvantages are high cost and poor popularity. 20 Retropharyngeal lymph nodes are classified according to location into nasopharyngeal or oropharyngeal level (above the hyoid level) and laryngeal level (below the hyoid level). For patients above the hyoid bone level, especially those at the nasopharyngeal level, the difficulty of surgery lies in its deep and upper location, located in the inside of the carotid artery and deep surface of the mandible, which results in high surgical risk and large trauma. The reported approaches for this type of surgery include transparotid gland-neck approach, oral approach, and neck-mandible approach. 21 Chen et al. reported 6 cases of retronasopharyngeal lymph node dissection for PTC through cervical approach, and no complications occurred in all patients, confirming the safety and effectiveness of this protocol. 21 For retropharyngeal lymph nodes at laryngeal and pharyngeal levels, the difficulty lies in the evaluation and treatment of laryngeal mucosa. Our case follows this type, but fortunately, the tumor is not close to the pharyngeal mucosa (Figure 1). In conclusion, the author believes that retropharyngeal lymph nodes dissection for PTC should be the first choice. Safely, effectively and economically individualized surgical approaches should be selected based on the characteristics of the disease and the advantages and disadvantages of various surgical approaches.
Differentiated thyroid carcinoma with RLNM may be associated with distant metastasis. Wang et al. reported distant metastasis in 9 of 25 patients at follow-up. 22 Moritani et al. showed that 10 of 22 cases of differentiated thyroid carcinoma with RLNM had distant metastasis at the time of diagnosis, and 6 patients died of distant metastasis during follow-up. 4 Togashi et al. reported 12 patients, 5 of whom developed distal disease during the follow-up. 5 The study of Victoria Harries MBBS et al showed that RLNM was a risk factor for tumor progression, as none of the 8 patients undergoing initial surgical treatment relapsed, and 19 patients had concurrent distant metastasis or progression to distant metastasis, with distant metastasis rates of 28.3% and 38.1% at 5 and 10 years, respectively. 8 However, due to the low incidence rate, there is no reliable evidence of disease-related mortality.
The initial RLNM of PTC is relatively rare. For PTC with extensive cervical lymph node metastasis or multiple recurrence, it is necessary to be vigilant about RLNM. Careful reading of imaging examination is the key and surgical treatment is the preferred treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
We have obtained the patient’s consent and signed the patient consent.