
Abstract
Gout nodules (tophi) are formed by a chronic inflammatory reaction in tissues resulting in deposition of urate crystals. They are commonly seen in joints and surrounding tissues, subcutaneous tissues, as well as the pinna and kidney, and are characteristic manifestations of gout. Vocal cord tophi are rarely reported in the literature, and patients often present with hoarseness, progressive dysphagia, and other symptoms. We report a case of a vocal cord mass found by gastroscopy in a patient with a history of gout for more than 20 years. Postoperative pathological findings were vocal cord tophi. Tophi can have serious consequences and should be included in the differential diagnosis of laryngeal masses in patients with a history of gout. Therapy should involve a combination of systemic uric acid-lowering treatment and surgery to improve symptoms and reduce recurrence.
Introduction
The generation and excretion of uric acid in the human body are in a dynamic balance. When either generation or excretion is impaired, excess uric acid can be deposited in any part of the body in the form of monosodium urate, forming gout nodules which are also known as tophi. Vocal cord tophi are atypical symptoms of gout. There are few clinical reports of tophi in rare locations, and the lack of specific symptoms means that clinicians lack understanding of tophi, which leads to the lack of reasonable diagnosis and optimal treatment for the disease. Our case was diagnosed by pathological examination after surgery. The definitive diagnosis of tophi depends on histopathological examination. The typical pathological findings are monosodium urate crystals and basophilic substances in the center of a tophus surrounded by macrophages and epithelioid cells, which may be accompanied by fibrosis. In the human body, tophi appear as raised yellow and white nodules of different sizes which form just below the skin or can sometimes break through the skin. The surface is thin, and a white powder or paste can be discharged if it is broken. Such eruptions do not heal for a long time, but secondary infection rarely occurs.
Case Report
A 56-year-old man was admitted to the hospital with vocal cord nodules found during an endoscopy five months earlier. He had smoked for 40 years and had a history of gout for more than 20 years. He reported that he usually took phenylbutazone dexamethasone and vitamin B1 when he was in pain, but he had not received systematic diagnosis and treatment. Some finger joints were swollen, and he had recently developed pain in the little finger of his left hand with a slight limitation of activity. Fortunately, he experienced no hoarseness, no pharyngeal pain, and no symptoms of dysphagia or dyspnea. For further diagnosis and treatment, he came to our hospital. Electronic laryngoscopy showed a protrusion about the size of a grain of rice at the left posterior union and a pale yellow nodule about the size of a mung bean at the right posterior union (Figure 1). Electronic laryngoscopy showed a protrusion about the size of a grain of rice at the left posterior union and a pale yellow nodule about the size of a mung bean at the right posterior union (arrow).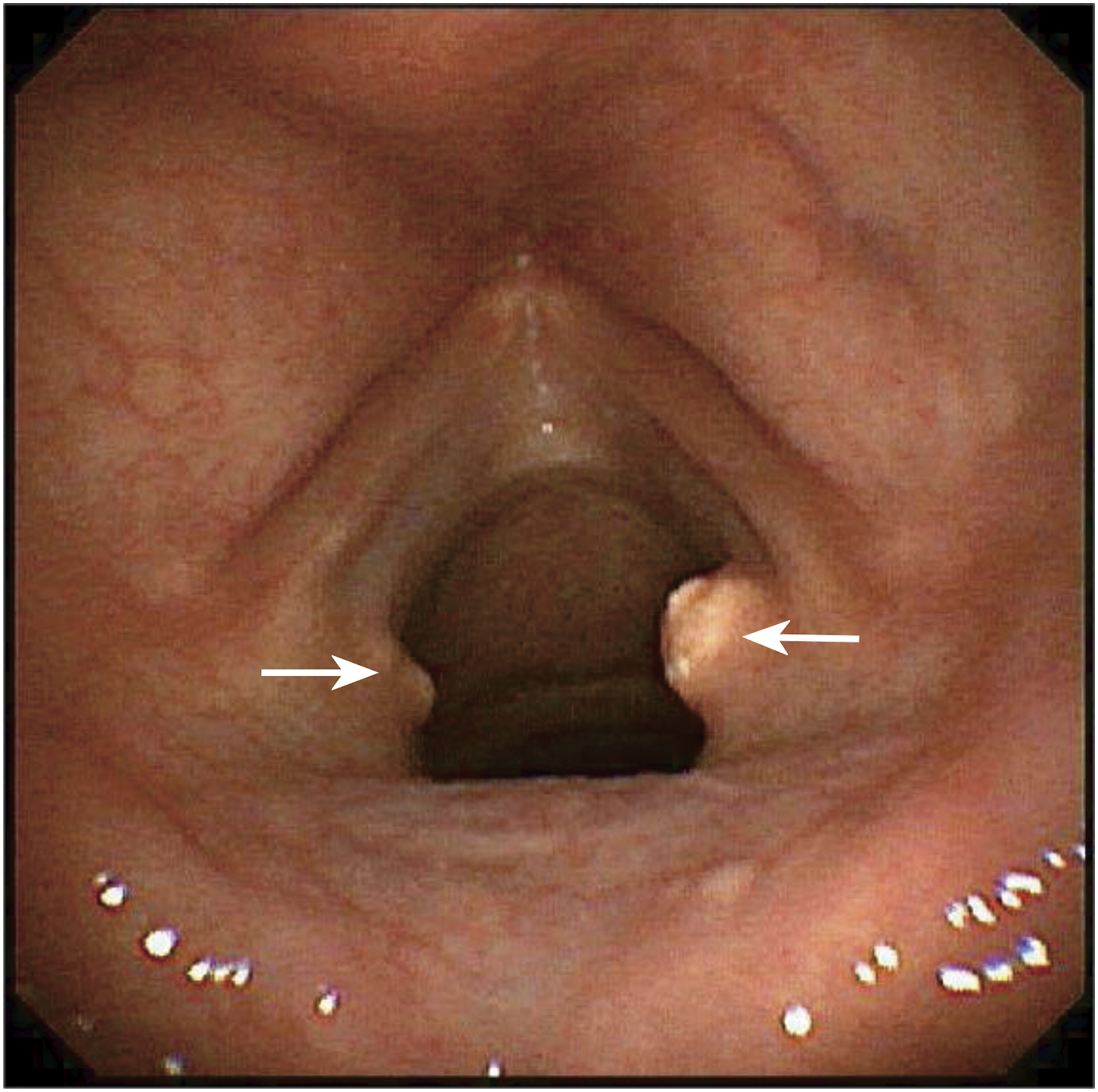
Blood test results were as follows: creatinine 127.4 μmol/L, uric acid 664.5 μmol/L, fasting blood glucose 7.05 mmol/L, total cholesterol 6.5 mmol/L, free cholesterol 2.21 mmol/L, triglyceride 2.85 mmol/L, low-density lipoprotein cholesterol 4.31 mmol/L, serum fructosamine 319.4 mmol/L, and hemoglobin A1c 7.6 mmol/L. Renal ultrasound showed that the shape and size of both kidneys were normal, parenchymal echo was uniform, no separation was observed in the double renal sinus area, multiple patchy regions of strong echo were detected in the double renal papilla area, the maximum was 0.3 cm, color Doppler flow imaging and color Doppler energy showed clear blood flow of both kidneys, and pulsed-wave Doppler showed no abnormal spectrum.
The right vocal cord nodule was removed by endoscopic resection under general anesthesia. The nodule was yellowish-white and silty. The postoperative mass was sent for pathological examination, and the histopathological result (Figure 2) was tophi on the right vocal cord. After surgery, the patient was transferred to the endocrinology department for treatment of gout, and laryngoscopy showed no recurrence six months later. Histopathological result was tophi on the right vocal cord (arrow).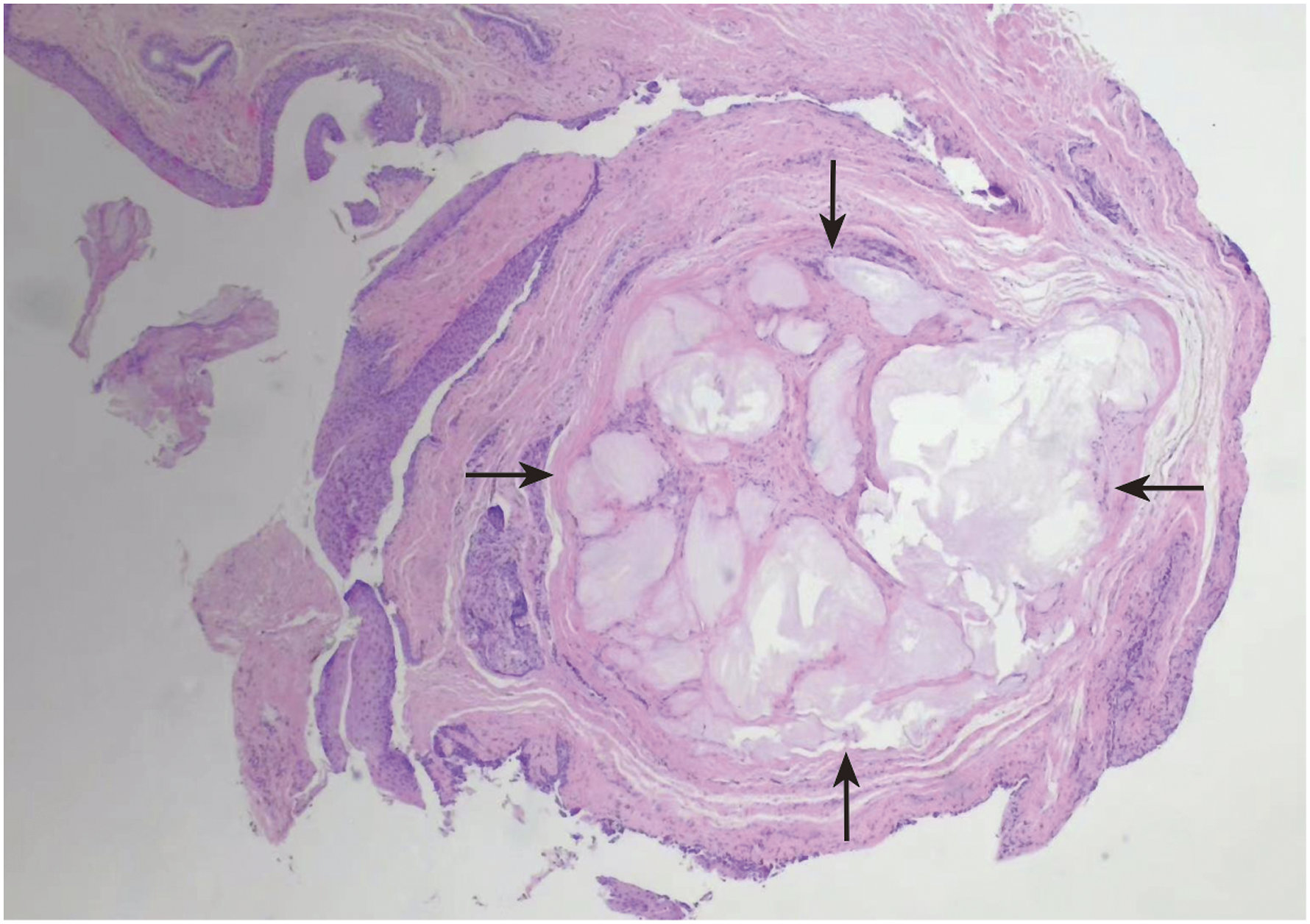
Discussion
Gout is a common chronic disease caused by chronically disordered purine metabolism and reduced uric acid excretion. Hyperuricemia is a leading cause of gout and an important biochemical basis for the occurrence of gout. Under normal circumstances, the production and excretion of uric acid in the human body are in dynamic balance. Once the production and/or excretion of uric acid is obstructed, blood levels of uric acid will increase, resulting in the development of hyperuricemia. 1
The clinical characteristics of gout are hyperuricemia, urate deposition, and gout arthritis, which can be combined with kidney damage. At the terminal stage, gout can manifest as joint malformation, urinary tract stones, and kidney stones. Tophi often appear in the chronic stage of gout and are a characteristic manifestation of gout, caused by the inflammatory response of tissues to urate crystals. 1 Our patient had a history of gout for more than 20 years without systematic treatment.
Tophi not only occur frequently in articular cartilage and around joints but also occasionally in the spine, spinal canal, and other sites. 2 Tophi are visible in the human body as bulges of various sizes of yellowish white nodules, with a thin surface. After rupture, a white powdery substance or paste can be discharged, usually over a long period of time, but secondary infection is rare. Tophi at atypical sites may be missed or misdiagnosed, and in many cases tophi at rare sites are only finally found accidentally by pathology, surgery, or imaging examination. 3 The typical location of a tophus in the head and neck is the auricle, but tophi in other parts of the head and neck have been reported, such as the nose, 4 middle ear, 5 throat, thyroid cartilage plate, 6 temporomandibular joint, 7 sternoclavicular joint, 8 and eye structures.9,10
The occurrence of a tophus in the neck or throat is relatively rare in clinical cases and has rarely been reported in the world. When affecting the vocal cords, subglottic tophi may cause hoarseness of different degrees, progressive dysphagia, and other symptoms. CT can better show the destruction of tophi and adjacent joints. This advantage is further enhanced by dual-energy CT, which can reveal more tophi and smaller tophi. Energy spectrum CT can perform substance separation and concentration imaging and allows qualitative and quantitative analyses of the detected substance. Compared with other examination methods, it can identify more tophi deposits, providing an imaging examination scheme for noninvasive diagnosis, 11 but histopathological analysis is still the gold standard for the diagnosis of tophi. Typical pathologic findings of tophi include a core of urate crystals and basophils, surrounded by macrophages and epithelioid cells, which may be accompanied by fibrosis. 12 It should be noted that monosodium urate crystals are water-soluble, and the use of water during specimen preparation may affect the pathological results. In our case, laryngeal nodules were accidentally found during gastroscopy, and postoperative pathological results confirmed tophi.
The involvement of tophi in the larynx and trachea may lead to respiratory stenosis and severe respiratory failure, which may endanger life. Arlandis 13 et al. reported a case of respiratory failure complicated by the involvement of tophi in the larynx and bronchus. In addition, inflammation in gout arthritis can lead to degeneration of the recurrent laryngeal nerve, which in turn leads to glottis stenosis. 14 Laryngeal gout may be located at the margin of the vocal cords, laryngeal ventricle, subglottic, thyroid cartilage, or cricoarytenoid joint.6,15-20 True vocal cord involvement often presents with mild symptoms such as hoarseness or sore throat.6,15,16 Cricoarytenoid joint involvement is often painful, and in severe cases it can lead to dyspnea.6,13
Although rare, laryngeal gout should be considered as a possible diagnosis in patients with dysphagia, dysphonia, or laryngeal lesions, especially in those with a history of gout. Because the prevalence of laryngeal gout may be higher than previously recognized, clinical awareness of the disease may lead to increased diagnosis rates. 21 Laryngeal tophus may also cause relevant pathological changes of adjacent tissue. Lee et al. 22 reported a case of laryngeal gout concurrent with tendonitis of the longus colli muscle tendons, causing symptoms of severe dysphagia, so the first diagnosis considered was chondrosarcoma; however after imaging using dual-energy computed tomography, evaluation results indicated laryngeal tophus, and postoperative pathological results further confirmed a laryngeal tophus. In view of the nonspecific manifestations of laryngeal gout, it should be differentiated from cancer, chondrosarcoma, tuberculous granuloma, inflammatory granuloma, etc. The exact diagnosis depends on biopsy and pathological examination.
Management of laryngeal gout requires the development of a systematic treatment approach, with lifestyle interventions as the first priority, including weight loss, avoidance of alcohol, and avoidance of high-purine foods. Acute inflammation can be treated with nonsteroidal anti-inflammatory drugs, steroids, or colchicine. Lifestyle interventions should be combined with allopurinol or febuxostat uric acid lowering agents. Laryngeal involvement of gout may require surgical intervention, such as endoscopic resection of tophi or tracheotomy for acute airway injury due to vocal cord immobility.16,21 Tophi may occur almost anywhere in the body and have serious consequences to the patient, even causing difficulty in breathing, suffocation, and other life-threatening problems. We hope that by reporting this case and reviewing the literature we will provide reference data to study, so that clinicians will become more fully aware of the atypical symptoms of gout and its possible abnormal distribution and detailed history, to improve disease diagnosis, and thus provide patients with the best treatment options.
Footnotes
Acknowledgments
We thank Prof. Xiaoyu Tuo and Jian Shen from the Department of Pathology, the First Affiliated Hospital of Kunming Medical University for providing and reviewing the pathological image.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from 2022 Yunnan Science and Technology Department - Kunming Medical University Joint Fund for Applied and Basic Research (No. 202201AY070001-078), Doctoral Scientific Research Fund of the First Affiliated Hospital of Kunming Medical University (No. 2021BS006), 535 Talent Project of First Affiliated Hospital of Kunming Medical University (No. 2022535D08).
Informed Consent
A legally authorized representative of the patient gave written consent for the publication of this case report.