
Abstract
Introduction:
Bamboo nodules are rare and have been shown to present in patients with rheumatologic disease.
Methods:
Three cases of bamboo nodules were investigated retrospectively in patients with previously-established rheumatologic processes. Patient data were analyzed.
Results:
All cases involved women presenting with dysphonia. One patient had elevated erythrocyte sedimentation rate and the presence of perinuclear anti-neutrophil cytoplasmic antibody, another had systemic lupus erythematosus and rheumatoid arthritis (RA), and the third had RA and Sjögren’s syndrome.
Conclusion:
This case series supports an association of bamboo nodules with rheumatologic disease, and voice quality may be improved using voice therapy as a first-line treatment. Intra-lesional corticosteroid injection, as well as addressing aggravating factors such as reflux also benefit voice quality. Areas for further research include the impact of diet eliminations, such as gluten and dairy, and of immunosuppressive therapies on voice function in patients with bamboo nodules.
Keywords
Introduction
Bamboo nodule is a type of benign vocal fold mass that presents primarily in women and is associated with autoimmune disease.1 -6 The most common presenting symptom is hoarseness.7,8 While bamboo nodules may be more common in certain types of autoimmune disease such as rheumatoid arthritis (RA), 2 they may occur in association with other autoimmune disorders; and the presence of a bamboo nodule should increase clinical suspicion for the presence of a systemic autoimmune condition.
Current understanding of “bamboo nodules” has developed since the mid-1900s. In 1959, Scarpelli et al described a case of systemic lupus erythematosus (SLE) presenting with laryngeal edema that ultimately led to the subject’s death. 3 “Inflammatory nodule” was the term used to describe the lesion at that time. In 1972, Webb and Payne described a woman with RA who had lesions on her vocal folds, hence “rheumatoid nodules.” 4 The change from “rheumatoid nodules” to “bamboo nodules” came in 1993, when Hosako, et al reported submucosal laryngeal lesions in the middle third of the vocal fold in a patient with SLE, noticing that it appeared similar to the nodes on a bamboo stem. 5
On laryngoscopic examination, bamboo nodules tend to be located in the subepithelial mid-musculomembranous portion of the vocal folds, unilaterally or bilaterally. They are creamy yellow in color.7,9 A transverse, band-like extension along the vocal folds is what makes them appear like bamboo shoots. 9 Laryngeal rheumatoid nodules are also subepithelial, but they are more ligamentous. 9 Both nodule types share histopathologic characteristics of palisading histiocytes surrounding granuloma formation with fibrinoid necrosis on hematoxylin-eosin staining.7,9
While the morphologic presentation of bamboo nodules has been understood better recently, the pathophysiologic link between bamboo nodules and autoimmune disease remains unclear. Hypotheses posit that immune complexes may be deposited within these lesions. 6 In a case report presented by Li et al, electron microscopy of a bamboo nodule demonstrated immune complex deposition within blood vessel walls. 10 Voice overuse at the higher pitches may lead to microphonotrauma in the mid-portion of the vocal fold where the amplitude of the mucosal wave is largest. 10 Immune complexes with higher molecular weights may become lodged in the exposed vasculature within the vocal fold, triggering an inflammatory response.10,11
The study of voice quality over time in patients with bamboo nodules has not been investigated thoroughly. However, previous case series have elucidated through clinical observation that voice therapy should be used as a first-line, noninvasive treatment to improve voice quality.1,10 -12 Secondary options, although more invasive, may include steroid injection or, rarely, surgical excision.7,13 Treating aggravating factors contributing to hoarseness such as reflux and the underlying autoimmune disease can be effective, also.8,14 Given their association with autoimmune disease, elimination diets, particularly with gluten and cow’s milk dairy, may be considered as a supplemental therapy option in addition to pharmacotherapies. 15
This report retrospectively investigated and compared 3 patients with confirmed bamboo nodules. Patient presentation, physical exam findings with repeated strobovideolaryngoscopy (SVL), treatment, and outcomes are highlighted.
Case 1
Patient Description
A 56 year-old woman with a past medical history of reflux, elevated erythrocyte sedimentation rate (ESR), and the presence of perinuclear anti-neutrophil cytoplasmic antibody (p-ANCA), presented to the laryngologist for hoarseness evaluation.
She had started estrogen-containing hormone replacement therapy (HRT) 1 year prior to her initial visit. Within 1 month of initiating therapy, she had noticed joint pain and voice changes. She denied any previous history of hoarseness. She had been placed on a trial of omeprazole by her primary care provider without improvement in her voice. When a course of oral corticosteroids was prescribed, she recalled mild improvement in voice quality. She denied history of tobacco use, and she had minimal alcohol and caffeine consumption.
Prior otolaryngology evaluation with flexible laryngoscopy diagnosed “vocal nodules,” and she was referred to a speech-language pathologist (SLP) for voice therapy. Voice therapy was pursued with incomplete benefit, and she had persistent voice fatigue.
Initial SVL revealed bilateral, mid-musculomembranous nonspecific fibrous vocal fold masses with nodular characteristics, and a possible cyst on the left vocal fold that was deeply embedded within the vocal fold tissues (Figure 1A). Other findings included stiffness at the base of the masses, glottic insufficiency, mild-moderate right vocal fold paresis, muscle tension dysphonia (MTD), and mild reflux laryngitis. A diagnosis of left bamboo nodule was suggested 1 year later after the patient was followed every 3 months with repeat SVL. Reflux finding score (RFS) was 12 on initial presentation and normalized to 7 on subsequent follow-up examination.
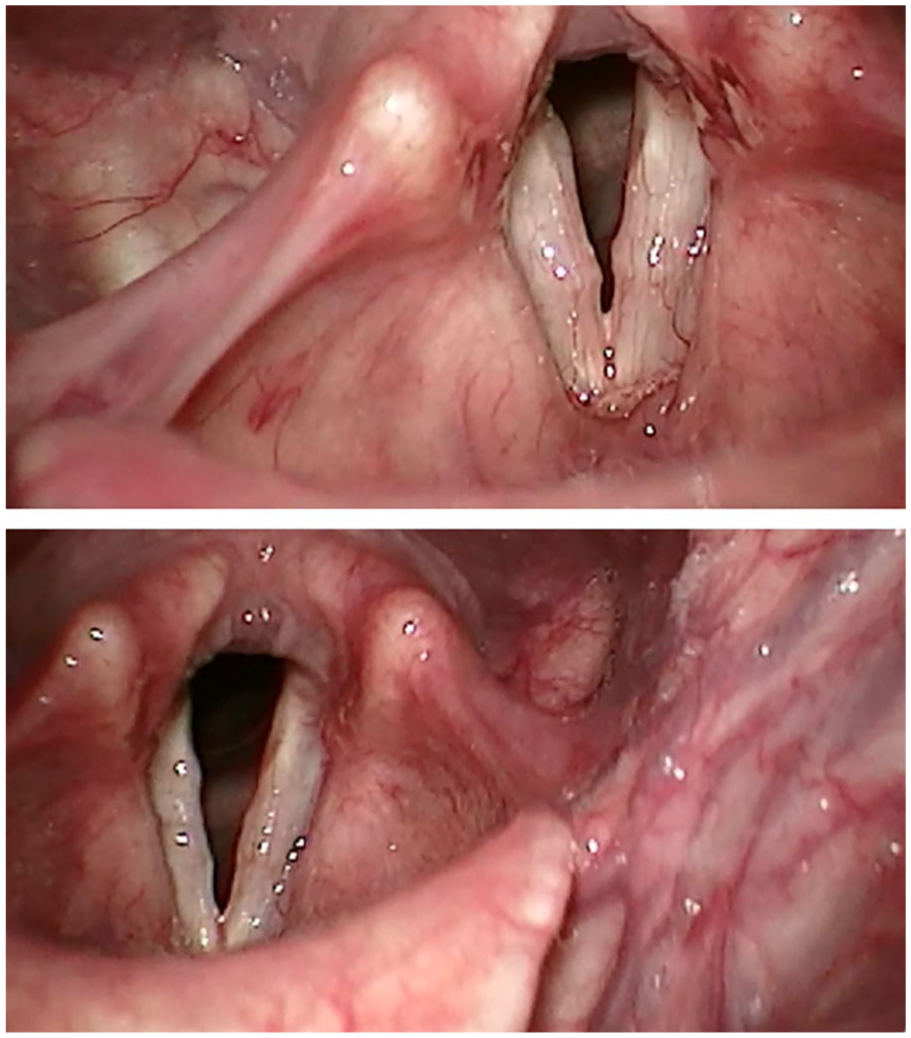
Case 1. (A, top) Pretreatment rigid stroboscopy. (B, bottom) Posttreatment after gluten-free diet, reflux management, and voice therapy.
Treatment Plan
Given elevated ESR and p-ANCA positivity, clinical suspicion for rheumatologic cause of the vocal fold masses (“bamboo nodules”) was raised. Since vocal folds are hormone-responsive, influence of her prior HRT could not be excluded. Follow-up with rheumatology, voice therapy with a SLP addressing MTD, vocal hygiene, and myofascial release were recommended.
At her 6th week follow-up, she noted a 60% to 70% improvement in voice quality with voice therapy. A 2 week gluten-free diet trial was recommended followed by reflux therapy with omeprazole 40 mg twice daily, ranitidine 300 mg at bedtime (switched to famotidine 40 mg nightly after ranitidine was recalled), and reflux diet/lifestyle modifications. At her 4th month follow-up appointment, she reported 99% improvement in voice quality (Figure 1B). Her voice remained stable on routine follow-up over 2 years. Omeprazole was tapered gradually and subsequently discontinued with no change in symptoms or laryngoscopic findings.
Case 2
Patient Description
A 24 year-old woman with a past medical history of SLE and RA presented to the laryngologist for the evaluation of hoarseness.
Since resuming work as a music therapist 6 months prior to her initial visit, her voice became raspy with use. She denied any issues with her voice in the past. When singing, pitches were inconsistent, and her voice cut out, or would not come out at all. She noted dry mouth/throat despite drinking a lot of water daily. She saw rheumatology for SLE and RA and was taking hydroxychloroquine 200 mg twice daily, prednisone 5 mg daily, and methotrexate 0.3 mg weekly. She denied tobacco and alcohol use.
SVL revealed a right vocal fold bamboo nodule, mild right vocal fold paresis, glottic insufficiency, mild reflux laryngitis, and MTD (Figure 2A). On initial evaluation, the RFS was 9.
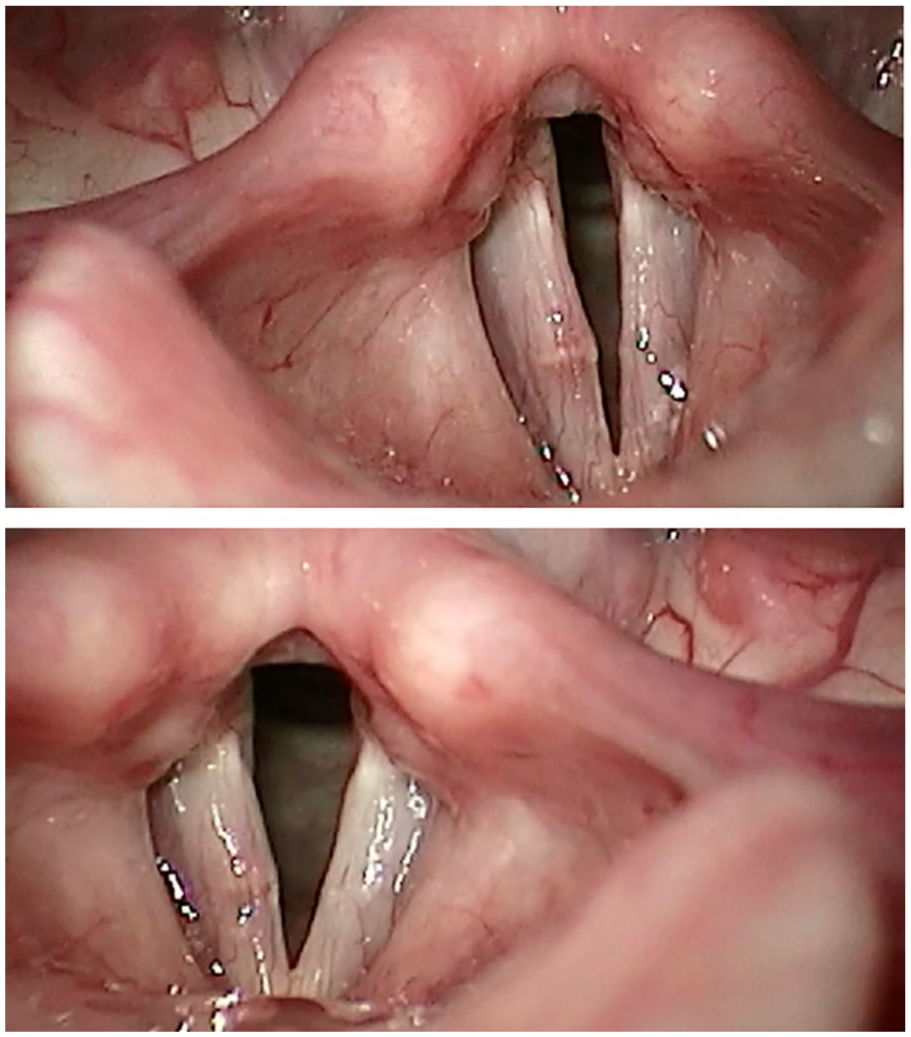
Case 2. (A, top) Pretreatment rigid stroboscopy. (B, bottom) Posttreatment after dexamethasone vocal fold injection.
Treatment Plan
Voice therapy with a SLP was pursued. Two-week gluten-free and dairy-free diet trials were initiated, also. A right vocal fold steroid injection was to be considered if her voice quality did not improve.
At her 2nd month follow-up, she reported stable voice quality after 2 voice therapy sessions and sustained gluten and dairy-free diet. Due to incomplete benefit, a right vocal fold dexamethasone injection was performed. She reported subjective benefit in voice quality; decreased size of the bamboo nodule, improved stiffness, and near-complete glottic closure were seen on SVL at the 2nd and 4th month follow-up (Figure 2B). She was followed over the next year with stable results. She reported that her voice was satisfactory during that time.
Case 3
Patient Description
A 47 year-old woman, with a past medical history of RA, Sjögren’s syndrome, allergic rhinitis with childhood asthma, and reflux esophagitis, presented to the clinic for voice evaluation.
She reported dysphagia and odynophagia beginning 2 years prior to evaluation. She described the need to turn her head to swallow effectively. She noted diplophonia while singing and that “notes would not come out.” She also reported a clicking sound on swallowing coming from the anterior superior cervical/submandibular region that began 1 year prior to the first visit. She noted improved voice quality following a period of decreased voice use. She reported occasional solid food sticking on swallowing. She denied dyspnea.
She saw rheumatology for RA and Sjögren’s syndrome and was taking hydroxychloroquine 200 mg twice daily and methotrexate 15 mg weekly. She started omeprazole 40 mg twice daily after rheumatology evaluation for dysphagia with symptom improvement, switched to famotidine per her primary care physician’s recommendation with worsening symptoms, and then resumed omeprazole 40 mg every morning. Previous endoscopy performed by gastroenterology revealed Los Angeles grade B esophagitis without hiatal hernia, which prompted an increase in omeprazole dose to 40 mg twice daily. She had started a gluten-free diet 2 years prior to consultation with us and eliminated red meat, with improvement. She denied eliminating dairy intake.
SVL examination revealed moderate reflux laryngitis, mild right vocal fold paresis with right false fold atrophy, left vocal fold bamboo nodule with associated stiffness/mild mass effect, glottic insufficiency, mild MTD, and mild Reinke’s edema (Figure 3A). On initial evaluation, the RFS was 14, which normalized to 6 on follow-up.
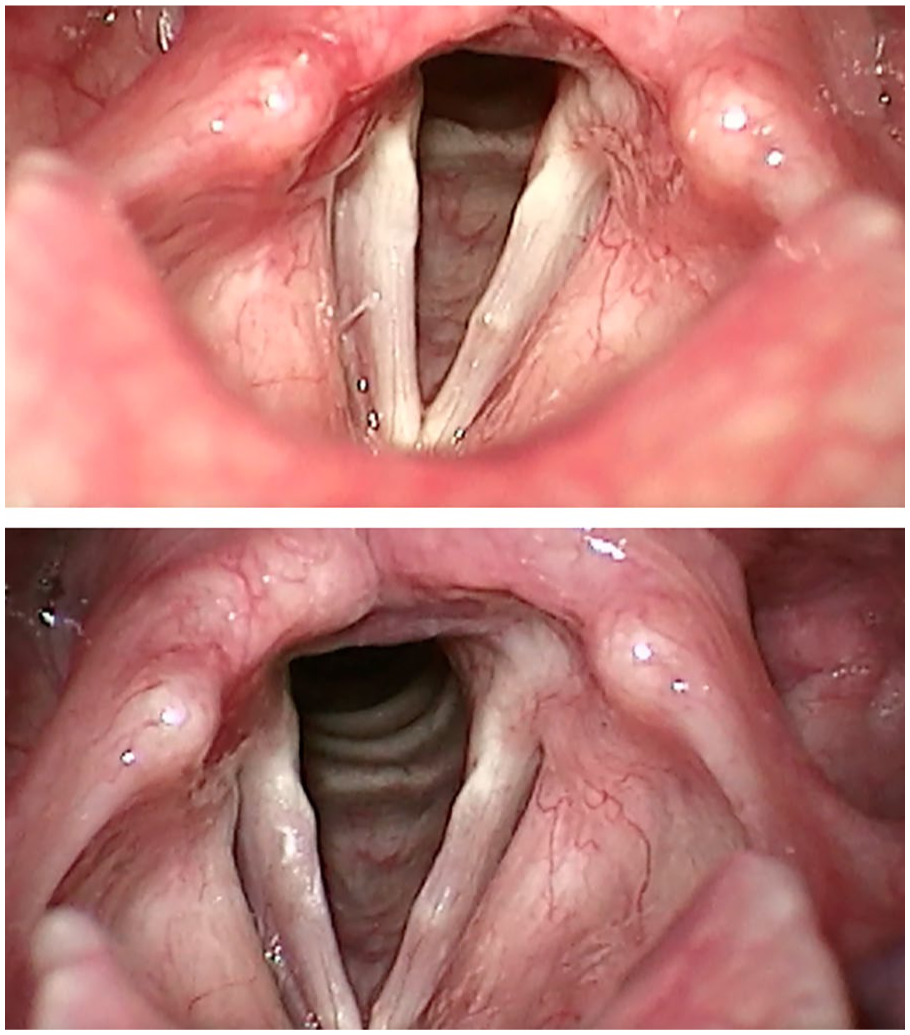
Case 3. (A, top) Pretreatment rigid stroboscopy. (B, bottom) Posttreatment after dexamethasone vocal fold injection.
Treatment Plan
She was advised to continue omeprazole 40 mg twice daily, famotidine 40 mg at bedtime, gluten-free diet, add a low-acid reflux diet, and begin voice therapy.
At her 3rd month follow-up, she reported improvement in the clicking noise while swallowing and less diplophonia while singing. Her voice quality still fluctuated, and she sometimes experienced aphonia while attempting to sing. Repeat SVL revealed markedly improved reflux and persistent left bamboo nodule. At her 5th month follow-up, a right vocal fold dexamethasone injection was performed due to incomplete therapeutic benefit. She was evaluated 3 weeks status post–dexamethasone injection with improved mucosal wave of the left vocal fold on SVL. She continued voice therapy with subjective benefit in voice.
Discussion
We presented 3 patients with rheumatological disease and a bamboo nodule. In a systematic review conducted by Chapa et al, autoimmune-associated vocal fold lesions were evaluated across 21 articles consisting of 83 cases. 9 Most of these cases were bamboo nodules (79.5%), while the others were rheumatoid nodules (20.5%). 9 Descriptive statistics were not separated between these nodule types (they were reported together); however, since most were bamboo nodule cases, comparisons may still be made with the cases presented in this report. All 3 cases presented to our clinic with dysphonia, which is the most commonly-reported complaint (95.1% of patients) in those eventually diagnosed with bamboo nodules. 9 Chapa et al reported that most of these nodules were bilateral (83.8%), multiple in number (92.3%), and located in the mid-musculomembranous portion of the vocal fold (94.5%). 9 A decreased mucosal wave was evident in most patients (93.3%), while abnormal glottic closure was less prevalent (16%). 9 While Case 1 had bilateral nodules, all were subepithelial and in the middle third of the vocal fold. All cases also demonstrated decreased mucosal wave and glottic insufficiency that improved with voice therapy. Additional benefit was achieved with a vocal fold steroid injection, if needed.
The treatment plans presented were based on patient presentation and shared decision-making. Voice therapy with a SLP, as well as voice rest, can result in substantial improvement in voice quality in some of these patients.9,12 However, in professional voice users (people who are required to use their voice for work), voice rest may not be a feasible solution. In the review by Chapa et al, voice therapy was associated with superior outcomes compared with medical or surgical treatment alone. 9 Voice therapy plus medical treatment represented the most common intervention subtype with 94.4% of patients reporting an improvement in voice. 9 Our first case demonstrated a 60% to 70% improvement in voice quality with voice therapy alone at her 6th week follow-up. In the second patient, voice therapy was attended twice and less helpful in reaching her goals. Vocal fold steroid injection offered additional benefit. In the third case, voice therapy offered incomplete benefit, and therefore, a vocal fold steroid injection was performed in addition to continuing voice therapy. Surgery is rarely needed and reserved for cases unresponsive to therapy, injections, and/or treatment of underlying rheumatologic disease.
Management of rheumatologic disease with an anti-inflammatory diet also may show beneficial voice outcomes.13,14 Our first case achieved a “99%” improvement in symptoms after voice therapy and reflux management. The second case had a satisfactory improvement in voice following a vocal fold injection with steroid and incorporating a gluten and dairy-free diet. In the third case, voice quality improved on additional reflux medication and diet modifications in the setting of moderate reflux laryngitis.
Bamboo nodules are often preceded by a diagnosed autoimmune condition but may also be the first sign of disease. 9 If symptoms persist despite conservative management, further evaluation is warranted.9,15 In a case report by Malinvaud et al, a 30 year-old woman had persistent dysphonia despite smoking cessation and anti-reflux medication management for 2 months. 15 Physical examination was consistent with bamboo nodules, and an underlying autoimmune condition was suspected. 15 Further history revealed a 10 year history of intermittent malar rash and hair loss (among other symptoms) with confirmatory testing that supported a diagnosis of SLE. 15 Systemic treatment with prednisolone and hydroxychloroquine substantially improved her voice. 15
Our report is limited by the small sample size of 3 patients. So, correlational data examining bamboo nodules and rheumatological disease could not be performed. Additionally, validated clinical outcome data, such as the Voice Handicap Index-10 score for assessing subjective voice quality and acoustic or aerodynamic function for objective voice quality, were not available for review. In these cases, percent improvement in voice quality was obtained directly from the history of present illness section of the office visit notes.
Rheumatological disease processes affecting voice quality occurs also in the absence of bamboo nodules.16 -18 Cricoarytenoid and cricothyroid joint arthritis, mucosal edema, myositis of the intrinsic laryngeal muscles, vocal fold mobility impairment, inflammation, and vocal fold fixation seen in RA, SLE, and Sjögren’s syndrome contribute to dysphonia, as well.16,17 In a study conducted by Beirith et al, 27.7% of patients with RA presenting with dysphonia had had a normal laryngoscopic examination. However, patients who had the disease for over 15 years were more likely to have detectable laryngeal alterations. 15 In patients with bamboo nodules, the prevalence of underlying autoimmune disease ranges between 80% and 100%. 17 The presence of bamboo nodules has been associated with active disease.17,18 So, it is possible that the lower end of the prevalence range may be due to inactive autoimmune disease.17,18
Given the female predominance of bamboo nodules, future research could examine the role of HRT in developing these lesions. Estrogen displays various downstream effects based on the receptor to which it binds. 19 Variations in receptor expression patterns across tissues and life-stages also contribute to estrogen’s diverse effects in the body. 19 This may explain why estrogen can have both anti-inflammatory and pro-inflammatory properties. 19 Case 1 experienced dysphonia shortly after beginning estrogen-containing HRT. Although a causal relationship cannot be confirmed, further investigation into this relationship seems warranted. Donor body studies and postoperative pathologic evaluation support the presence of these receptors in the vocal fold, with estrogen receptors residing mostly in the musculomembranous portion.19,20 There is evidence to support estrogen’s expression in edematous laryngeal tissue and in laryngoceles; however, its association with the development of bamboo nodules has not been established. 19
Conclusion
The presence of a bamboo nodule on the vocal fold should raise clinical suspicion for autoimmune/rheumatologic disease. Voice therapy is recommended as a first-line treatment to improve voice quality. Establishing a diagnosis of any underlying disorder and on addressing patient-specific aggravating factors is also essential.
Footnotes
Ethical Considerations
Our institution does not require IRB approval for reporting individual cases or case series with 3 subjects or fewer.
Consent for Publication
Informed consent was obtained from the individuals via email or phone.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Additional data on these cases cannot be shared ethically due to identity compromise.