
Abstract
Objectives
Vitamin D (VD) plays role in wound healing and protection against infections. The relationship between plasma VD level and the outcomes of Type 1 tympanoplasty (T1T) has not been studied before.
Methods
A total of 101 patients with chronic otitis media scheduled for T1T were divided into four groups in relation with their VD levels as severe insufficiency, insufficiency, mild-to-modest deficiency and optimal VD level groups. Graft success, hearing improvement and postoperative infection rates were compared among the groups in 12-month follow-up period.
Results
The graft success rate (P = 0.014) and air-bone gap gain (P = 0.004) were significantly higher, and postoperative infection rate was significantly lower (P < 0.001) in optimal VD level group.
Conclusion
25-OH VD deficiency should be considered as a factor for failure in T1T. VD replacement may increase success of tympanoplasty in patients with low preoperative serum VD levels.
Introduction
Chronic suppurative otitis media (CSOM) is a condition characterized by perforation of the tympanic membrane (TM), intermittent or persistent ear discharge, and conductive or mixed type hearing loss. Type 1 tympanoplasty (myringoplasty) is performed to repair the TM, restore normal hearing and prevent middle ear infection and ear discharge. 1 It is also a useful procedure in terms of preventing possible squamous cell migration into the middle ear and development of cholesteatoma in the long term. 2
The success of Type 1 tympanoplasty has been reported in a wide range, between 35% and 100%. 3 Therefore, many researchers have focused on the factors affecting the success of this procedure. 4 Various factors including the age of the patient, the location and size of the TM perforation, the type of graft material, the presence of ear discharge before surgery, the condition of the contralateral ear, and the experience of the surgeon have been studied as the factors affecting a successful outcome. 1 -5 However, even if all these factors are at optimum, myringoplasty may fail.
Although 25-OH Vitamin D is primarily responsible for calcium homoeostasis and bone metabolism, its receptors have been demonstrated in the cells of many tissues including intestine, pancreas, kidney, liver, colon, immune system and the epithelial cells of bronchi and skin. 6 In fact, it has been shown that Vitamin D plays role in immune system and wound healing. 7 -9
To our knowledge, the relationship between plasma 25-OH Vitamin D level of the patients and the outcomes of Type 1 tympanoplasty has not been studied before. In this study, we aimed to determine whether plasma Vitamin D level is a factor affecting the success of Type 1 tympanoplasty.
Patients and methods
This prospective controlled study was conducted on patients who underwent Type 1 tympanoplasty due to CSOM in Balıklıgöl State Hospital, Otorhinolaryngology Clinic between June 2018 and June 2019. The study protocol was approved by the ethics committee of Harran University (dated April 5, 2018; decree no: 18/04/34). The patients included in the study were informed about the study protocol, and their written informed consents were obtained.
The inclusion criteria were presence of a perforated TM, age older than 7 or younger than 65 years, and a Middle Ear Risk Index (MERI) 10 score smaller than 6, indicating a low risk for tympanoplasty failure. The exclusion criteria were age younger than 7 or older than 65 years, current smoking, history of systemic disorders including diabetes mellitus, chronic renal or liver disease, autoimmune disorders, coronary artery disease, malignancy, peripheral vascular disorders, any known problems regarding wound healing, use of anti-epileptics, bile acid binding resins, or Vitamin D replacement. The patients who were lost to follow up and the ones who did not volunteer to participate in the study were also excluded.
Medical histories of the patients were obtained and a detailed otorhinolaryngological examination including otoscopic and microscopic examinations of the TM and middle ear was performed. An experienced audiologist performed pure-tone and speech audiometry to all patients using Interacoustics AC 3 audiometry device, two weeks prior to surgery and 12 months after surgery.
The level of 25-OH Vitamin D was measured preoperatively using ARCHITECT 25-OH Vitamin D reactive (Abbott, Ireland) with chemiluminescent microparticle immunological method (CMIA), in an ARCHITECT Plus i2000 immunoassay analyser.
The patients were divided into four groups in relation with their 25-OH Vitamin D levels: • Severe insufficiency group: 25-OH Vitamin D level ≤10 ng/ml, • Insufficiency group: 25-OH Vitamin D level 10–20 ng/ml • Mild-to-modest deficiency group: 25-OH Vitamin D level 20–30 ng/ml • Optimal Vitamin D level group: 25-OH Vitamin D level ≥30 ng/ml.
Surgical technique
Type 1 tympanoplasty was performed with a postauricular approach, under general anaesthesia. Vascular strip incision was made along the tympano-squamous and tympano-mastoid suture lines in the external auditory canal, and the vascular strip was elevated to facilitate the exposure of the middle ear and perforation margins. The middle ear cavity was explored and integrity of the ossicular chain was ensured. Temporal muscle fascia was used as a graft using the underlay technique.
Follow-up and success of surgery
The patients were called for follow-up visits at postoperative 1st, 3rd, 6th and 12th months. Both otoscopic and microscopic examinations were performed, and even minute perforations were regarded as graft failure. Any purulent discharge in the external ear canal was regarded as infection.
Postoperative audiological test was performed at postoperative 12th month. A postoperative air-bone gap improvement greater than 10 dB was regarded as hearing gain.
Statistical analysis
Statistical analyses were performed using SPSS v. 20 software. The conformity of the variables to the normal distribution was examined using visual (histogram and probability graphs) and analytical methods (Kolmogorov-Smirnov/Shapiro-Wilk tests). Descriptive analyses are presented as mean and standard deviations (mean ± SD) for normally distributed variables, median (minimum, maximum) for non-normally distributed variables, and frequency tables for ordinal variables. Since it was determined that age and pre- and postoperative air-bone gaps did not show normal distributions, they were compared among the study groups using the Kruskal–Wallis test. The difference in gender distributions of the groups was analysed with the Mann–Whitney U-test. Results are presented as number and percent. Graft success, postoperative infection, and air-bone gap gain ordinal data were compared among the study groups using the Mann–Whitney U test. A p value ≤ 0.05 was considered statistically significant.
Results and analysis
The analysis of the study groups in relation with their serum Vitamin D levels.
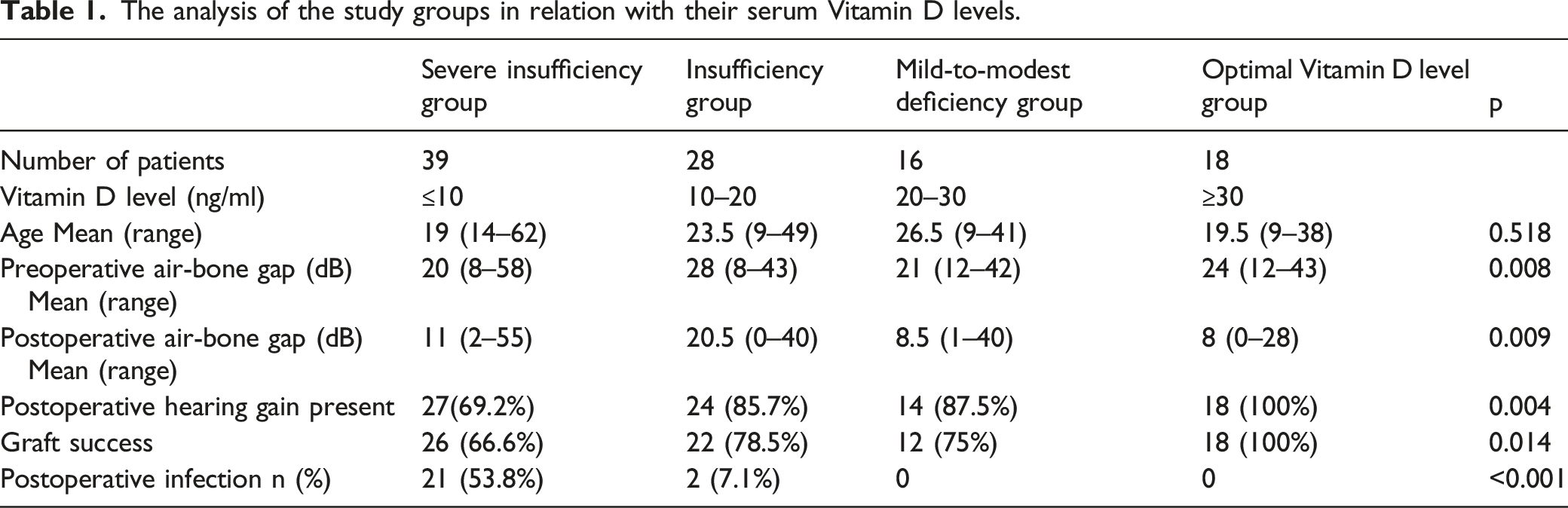
The graft success rate at postoperative 12th month was 66% in severe insufficiency group while it was 100% in optimal Vitamin D level group, with a significant difference among the groups (P = .014). As seen in Table 1, the graft success rate decreased as the serum 25-OH Vitamin D level decreased.
When the air-bone gap gain after Type 1 tympanoplasty was compared among the study groups, 69.2% of the patients in severe insufficiency group had hearing gain while this rate was 100% in the optimal Vitamin D level group. The difference among the study groups was statistically significant (P = .004, Table 1).
Comparison of the study groups for infection in the 12-month follow-up period showed that 53.8% of the patients in severe Vitamin D insufficiency group had infection at the site of surgery while this rate was 7.1% in Vitamin D insufficiency group. The patients in mild-to-modest deficiency and optimal Vitamin D level groups did not have any infection in the postoperative period (P < .001; Table 1).
Discussion
In our study, we investigated the role of plasma 25-OH Vitamin D level on the outcome of type 1 tympanoplasty, and found that both graft success and hearing gain rates were significantly higher and postoperative infection rate was lower in the patients with optimal serum Vitamin D levels.
The graft success rate after myringoplasty has been reported in a wide range. van Stekelenburg et al. reported a success rate of 91.9% in cartilage tympanoplasty performed by experienced surgeons, and a success rate of 66.7% in temporal fascia graft tympanoplasty performed by less experienced surgeons. 4 The main factors affecting a successful outcome have been reported as the type of graft material, age, gender, surgical technique, surgeon’s experience, dry middle ear at the time of surgery, the condition of the opposite ear, Eustachian tube dysfunction and presence of chronic disorders including diabetes and chronic kidney failure. 4
The prevalence of Vitamin D deficiency may be up to 80% in the society, 11 including our country. 12 The risk factors for Vitamin D deficiency include advanced age, less exposure to sunlight due to wearing traditional clothes, spending more time in indoors, use of sunscreen creams, physical inactivity, smoking, air pollution, kidney disease, liver disease and use of medications that affect Vitamin D metabolism such as anticonvulsants and glucocorticoids. 11 Wearing head cloths and traditional cloths have been reported as a risk factor for hypovitaminosis D even in sunny countries. 13,14 Wearing head clothes and traditional clothes leaving bare only the hands is very common among men and women in Urfa, where this study has been conducted, and this may be a reason for vitamin D deficiency in our study population.
Season and ethnicity have been reported as important factors affecting the serum Vitamin D level and lower serum Vitamin D levels have been reported in fall and winter. 11 Therefore, our study was designed to include all seasons, and only the patients of the same ethnic origin were included.
It has been have shown that Vitamin D has an effect on the modulatory proteins of the immune system, and also plays role in the immune response against the viruses causing upper respiratory tract infections. 15 The Th1/Th2 balance hypothesis is the most widely accepted mechanism explaining the role of Vitamin D on immune system. As known, Th1 cells provide cellular immunity against viruses, intracellular pathogens and cancer cells while Th2 cells provide humoral immunity against extracellular pathogens through Ig activation. 16 Vitamin D is the natural stimulator of Th2 pathway. It has been supposed that Vitamin D deficiency impairs humoral immunity through decreased activity of Th2 cells. In addition, it has been known that 1,25(OH)2D, the active form of Vitamin D, enhances the secretion of antimicrobial peptides and supports immune system against infectious agents. 16 The role of Vitamin D levels on acute otitis media (AOM) has also been studied. Cayir et al. investigated Vitamin D levels in children with AOM and healthy controls, and found significantly lower levels in the ones with AOM. 17 Marchisio et al. reported that a higher AOM prevalence when serum 25-OH Vitamin D levels were <30 ng/mL, and administration of 1000 IU/day Vitamin D was associated with a significant reduction in the risk of uncomplicated AOM. 18 In our study, we followed up our patients for AOM attacks, and found a higher postoperative middle ear infection rate in those with low Vitamin D levels.
Vitamin D also plays role in wound healing. Yuan et al. showed that nuclear factor-ĸB pathway is activated, pro-inflammatory cytokines (IL-1β, IL-6 and TNF-α) are increased and wound healing is delayed in case of Vitamin D deficiency. 19 In fact, skin is both the source and the target of Vitamin D, and it has been shown that Vitamin D plays role in cutaneous wound repair through proliferation, migration and differentiation of epidermal stem cells. 7,8 The graft success of type 1 tympanoplasty depends on a healthy wound healing, therefore optimal Vitamin D levels may be required for a successful surgical outcome. However, no studies up to date has investigated the relationship between serum Vitamin D level and outcomes of type 1 tympanoplasty.
Other vitamins, including vitamins A, C, E, K, B1, B2 and B5 have been suggested to play role in cutaneous wound healing. 20 Although a number of basic science studies investigated the effect of vitamins on wound healing, 20 controlled trials, such as our study, are needed for further understanding of their role in postsurgical patients.
In our study, a statistically significant correlation was found between the graft success rate and the serum Vitamin D level in patients undergoing type 1 tympanoplasty due to TM perforation, and graft success rate was significantly higher in the ones with optimal Vitamin D levels. Improvement of air-bone gap was also significantly better in the ones with higher serum Vitamin D levels. Since we found lower infection rates in the ones with higher Vitamin D levels, we suppose that higher graft success rate and improvement in hearing in the ones with higher Vitamin D levels is due to positive the effects of Vitamin D on wound healing and protection against infections.
The relation of Vitamin D levels with AOM or otitis media with effusion has been studied by various authors, 17,18,21 -23 serum Vitamin D level was found to be significantly correlated with AOM and otitis media with effusion, and it was reported that those with low serum Vitamin D levels had significantly worse prognoses. On the other hand, a meta-analysis reported that plasma Vitamin D level might play an important role on the progression of AOM; however, it had no significant effect in patients with chronic otitis media. 24 However, no studies up to date investigated the success of the type 1 tympanoplasty in relation with the Vitamin D levels of the patients. In this respect, our study is the first one.
The most important limitation of our study is that the serum Vitamin D levels of the patients were not measured in the follow-up period. Serum Vitamin D level may vary in relation with the seasons. In our study, the serum Vitamin D levels of some patients might have increased or decreased due to seasonal changes during the 1-year follow-up period.
Conclusion
In conclusion, in this study, it was determined that Vitamin D deficiency significantly decreased graft success rate and increased the rate of postoperative infection. Therefore, 25-OH Vitamin D deficiency should be considered as a reason for failure in tympanoplasty/myringoplasty. Vitamin D replacement may increase success of tympanoplasty in patients with low preoperative serum Vitamin D levels by reducing postoperative infection and improving wound healing. Further prospective studies are needed to better enlighten the subject.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Accessibility Statement
The dataset of this research has been kept by the authors and may be requested from the