
Abstract
Objective
To systematically review the results of type 1 tympanoplasties with temporalis fascia (TF) vs cartilage grafts in patients with chronic otitis media.
Methods
Eligible studies were identified from PubMed, Ovid, and EMBASE databases prior to November 2021. We analyzed the pure tone audiometry (PTA) and air-bone gap (ABG) data as continuous variables, and the success rate was analyzed as a dichotomous variable.
Results
Forty-four studies, including 4582 patients, were eligible. The cartilage graft overall morphologic success rate was higher than that of the TF grafts (P < .001). In the palisade (P < .004) and island grafts (P < .001) subgroups, the analysis was significantly different. However, there was no significant difference in the inlay butterfly grafts subgroup. For hearing outcomes, the analysis revealed that TF grafts had a smaller mean post-operative ABG (P = .009). However, the subgroup analysis showed no significant difference in the mean post-operative ABG. For PTA, there was no significant difference in hearing improvement. However, the palisade cartilage graft subgroup resulted in a better hearing outcome than the TF graft subgroup in terms of the mean post-operative PTA (P = .007). There was no significant difference in the functional success rate or mean ABG gain.
Conclusion
Cartilage grafts have a better success rate than TF grafts in tympanoplasty. Both cartilage and TF tympanoplasty provided similar improvements in hearing outcome, while TF grafts generated a better outcome in post-operative ABG and palisade cartilage grafts in post-operative PTA. This may be related to the biological characteristics of the grafts. Further thorough studies need to be conducted.
Introduction
Tympanoplasty, a surgical repair of the tympanic membrane and the middle ear ossicles, has been well established as the surgery of choice for chronic otitis media.1,2 Various tissue grafts have been used in tympanoplasty, including the temporalis fascia (TF), cartilage, perichondrium, periosteum, vein, fat, and skin. 3 Of these grafts, TF is usually the most popular graft used by surgeons since it is easy to harvest. 4 TF graft failures are primarily related to retraction pockets, infection, and technical errors. 5 TF is also found to shrink, undergo atrophy, and have unpredictable changes due to its poor graft stability, with potential subsequent failure. 6 Therefore, cartilage grafts have been the usual choice for tympanic membrane reconstruction since these grafts exhibit resistance to retraction and resorption. 7 However, due to its thickness and characteristic rigidity, there is no consensus regarding its audiological aspects.8-10 This study aimed to conduct a comprehensive meta-analysis of existing studies to assess the results of type 1 tympanoplasties with TF vs cartilage grafts in patients with chronic otitis media.
Materials and methods
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement. 11
Search strategy
A systematic literature search in PubMed, Ovid, and EMBASE databases was conducted to identify relevant studies published in English prior to November 2021. The following terms were used in the search procedure: (“tympanoplasty” OR “myringoplasty” OR “type 1 tympanoplasty” OR “tympanic” OR “membrane”) AND (“fascia” OR “temporalis fascia” OR “graft”) AND (“cartilage” OR “tragal cartilage” OR “tragus” OR “cartilage with perichondrium” OR “graft”). Additional manual searches were performed using a list of references to eligible studies to retrieve other papers related to our topic and discard duplicate studies.
Selection criteria and data extraction
At the first level of filtering, two investigators examined the titles and abstracts of all identified studies and then reviewed the full articles of the titles or abstracts of eligible articles. Studies were included in the meta-analysis if the following inclusion criteria were fulfilled: (a) studies involving patients diagnosed with chronic otitis media and treated with type 1 tympanoplasty. Patients with a history of traumatic perforations, ossicular discontinuity, cholesteatoma, previous otologic surgeries, or syndromes affecting the status of the middle ear were excluded; (b) studies with complete preoperative and postoperative pure tone audiometry (PTA) tests, graft success rates, and patient air-bone gap (ABG) data; and (c) Studies published in English. Reviews, meta-analyses, and individual case reports were excluded. Two independent authors extracted the data with standardized data extraction tables, and any discrepancies were resolved through discussion or consultation with a third researcher. The collected data included authors, publication year, study type, age, surgical mode, sample size, follow-up time, and outcome.
Quality assessment and statistical analysis
We used the Cochrane Collaboration’s tool for assessing the risk of bias to determine the quality of the randomized controlled trials and the Newcastle‒Ottawa Scale to assess the quality of case‒control studies and cohort studies. Meta-analyses were performed with Stata version 15.0 (StataCorp., College Station, TX, USA). We analyzed the PTA and ABG data as continuous variables (mean ± standard deviation) and estimated with standard mean differences (SMDs). The success rate was analyzed as a dichotomous variable and estimated with odds ratio (OR). Heterogeneity was assessed with Cochran’s Q test. P values of <.1 denoted heterogeneity. The I2 statistic was used to evaluate the magnitude of heterogeneity. If I2 was >50%, the degree of heterogeneity was substantial. We selected the random effects model in this study. To evaluate the source of statistical heterogeneity, we performed subgroup analysis according to the type of evaluated use of palisade, inlay butterfly grafts, and island techniques. Egger’s test was used to quantify the publication bias, and trim-and-fill analysis was used to evaluate the effect of publication bias on the results. P values <.05 were considered statistically significant for all statistical analyses.
Results
A total of 44 studies that met the inclusion criteria for the meta-analysis involving 4582 patients were published between 2005 and 2021 (Figure 1).5,12-54 A total of 2294 patients underwent cartilage tympanoplasty, and 2288 patients underwent TF tympanoplasty. All the articles passed the quality assessment (Figure 1 and Table 1). Table 1 shows the general characteristics of the included studies. There were 11 prospective trials, 33 of which were retrospective. ABG was divided into two datasets: mean ABG gain and mean post-operative ABG. PTA was divided into two datasets: mean PTA gain and mean post-operative PTA. The success rate was divided into two groups: morphologic success and functional success. Morphologic success was defined as graft uptake at the final follow-up. Functional success was defined as a post-operative ABG of <20 dB.
55
Flowchart for the records selection process of the meta-analysis. General characteristics of the studies included in the meta-analysis. PTA: pure tone audiometry; ABG: air-bone gap.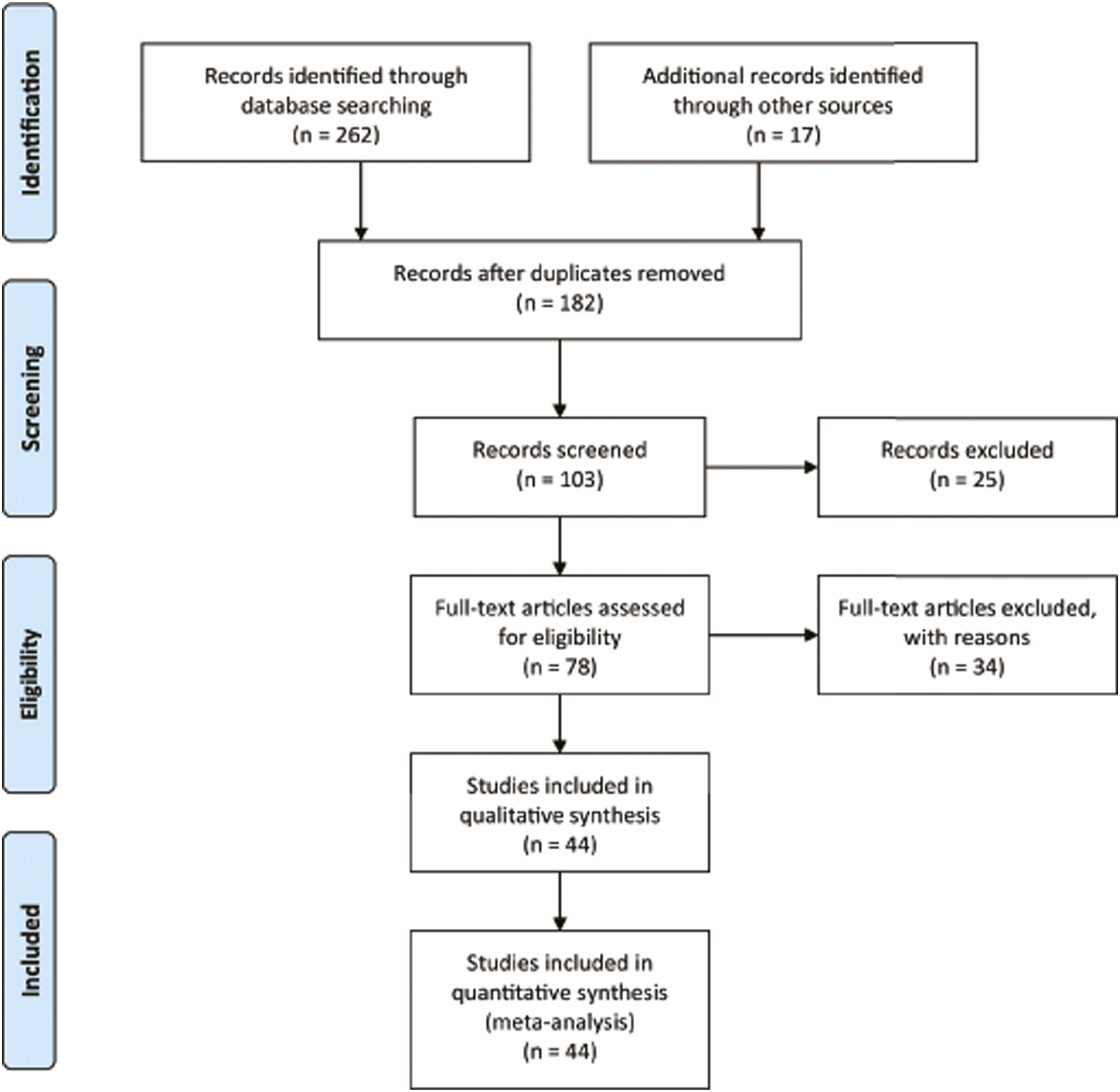

Success rate
For the morphologic success rate, 35 studies with 3558 patients were available for analysis.5,12,14,16-21,23-39,43,44,47-52,54 There was no obvious evidence of heterogeneity among the trials. The difference was significant, and the pooled OR for the morphologic success rate was 2.67 (95% CI: 2.05-3.47; P < .001; Figure 2). In the palisade cartilage graft subgroup, 8 available studies with 508 patients were analyzed. The difference was significant, and the pooled OR for the morphologic success rate was 2.27 (95% CI: 1.30-3.99; P < .004; Figure 2). The morphologic success rate in inlay butterfly graft tympanoplasty between the two groups in the analysis of 3 studies with 168 patients was not significantly different (OR: 2.50; 95% CI: .63-9.96; P = .193; Figure 2). In the island cartilage graft subgroup, 8 studies with 786 patients were available for analysis. The difference was significant, and the pooled OR for the morphologic success rate was 2.82 (95% CI: 1.67-4.80; P < .001; Figure 2). Morphologic success rate in chronic otitis media patients after type 1 tympanoplasty with temporalis fascia and cartilage grafts. (A) Pooled analysis of morphologic success rate, (B) subgroup analysis with cartilage technique.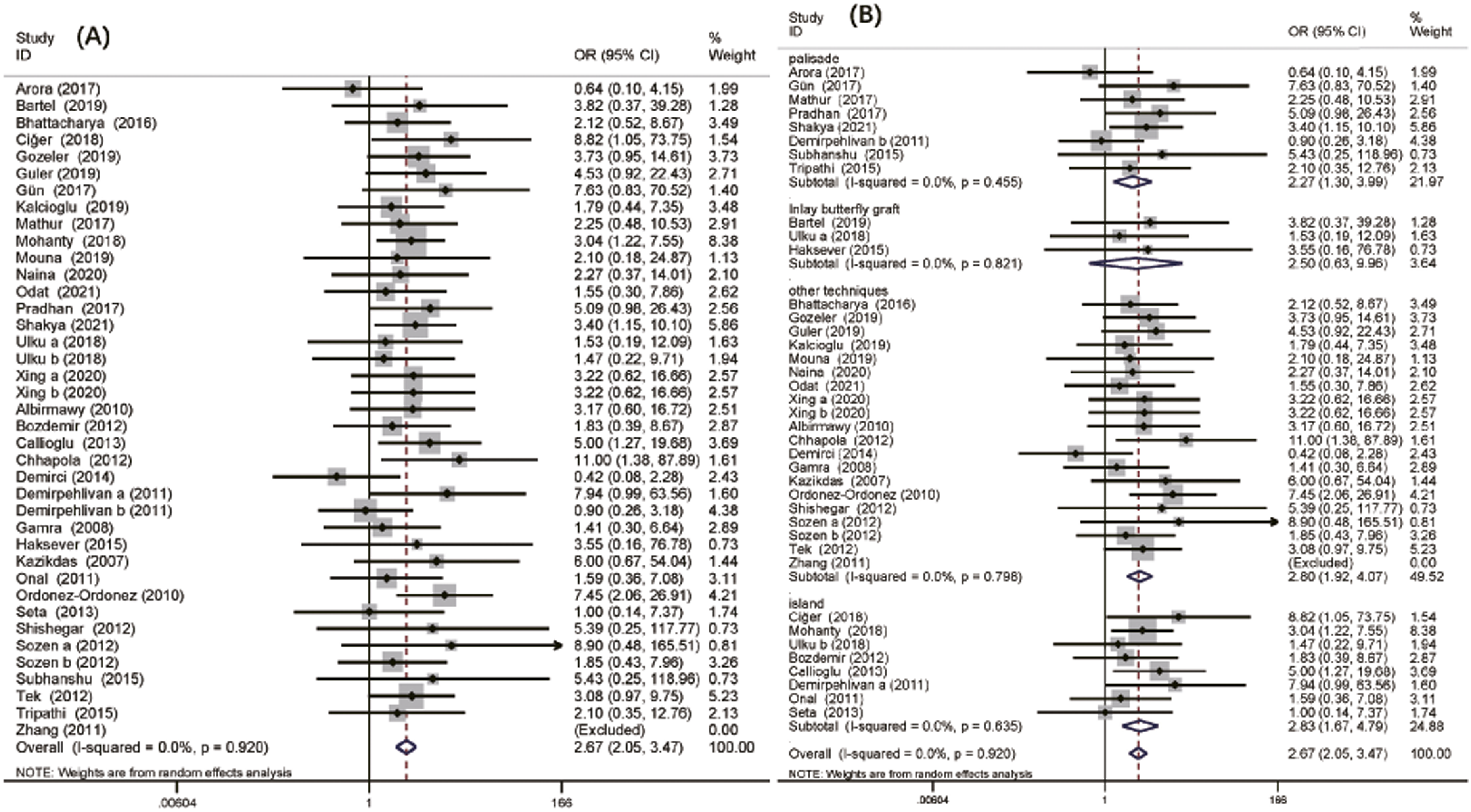
For the functional success rate, 9 studies with 1125 patients were available for analysis.19,25,31,35,37,40,45,46,53 The functional success rate was higher for the cartilage tympanoplasty analysis in all studies, and the difference was not significant (OR: 1.50; 95% CI: .89-2.53; P = .126; Figure 3). Functional success rate in chronic otitis media patients after type 1 tympanoplasty with temporalis fascia and cartilage grafts.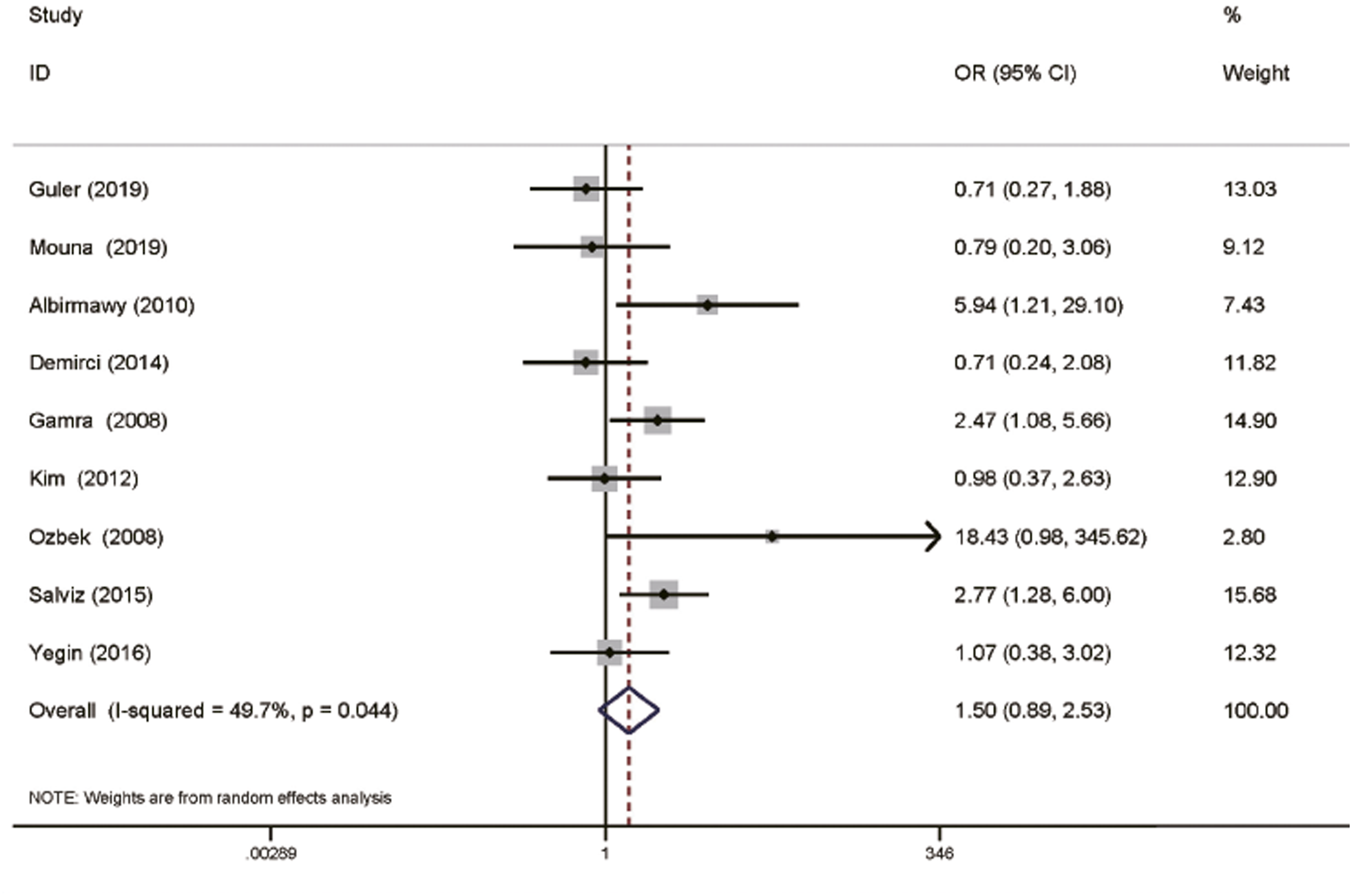
Mean air-bone-gap
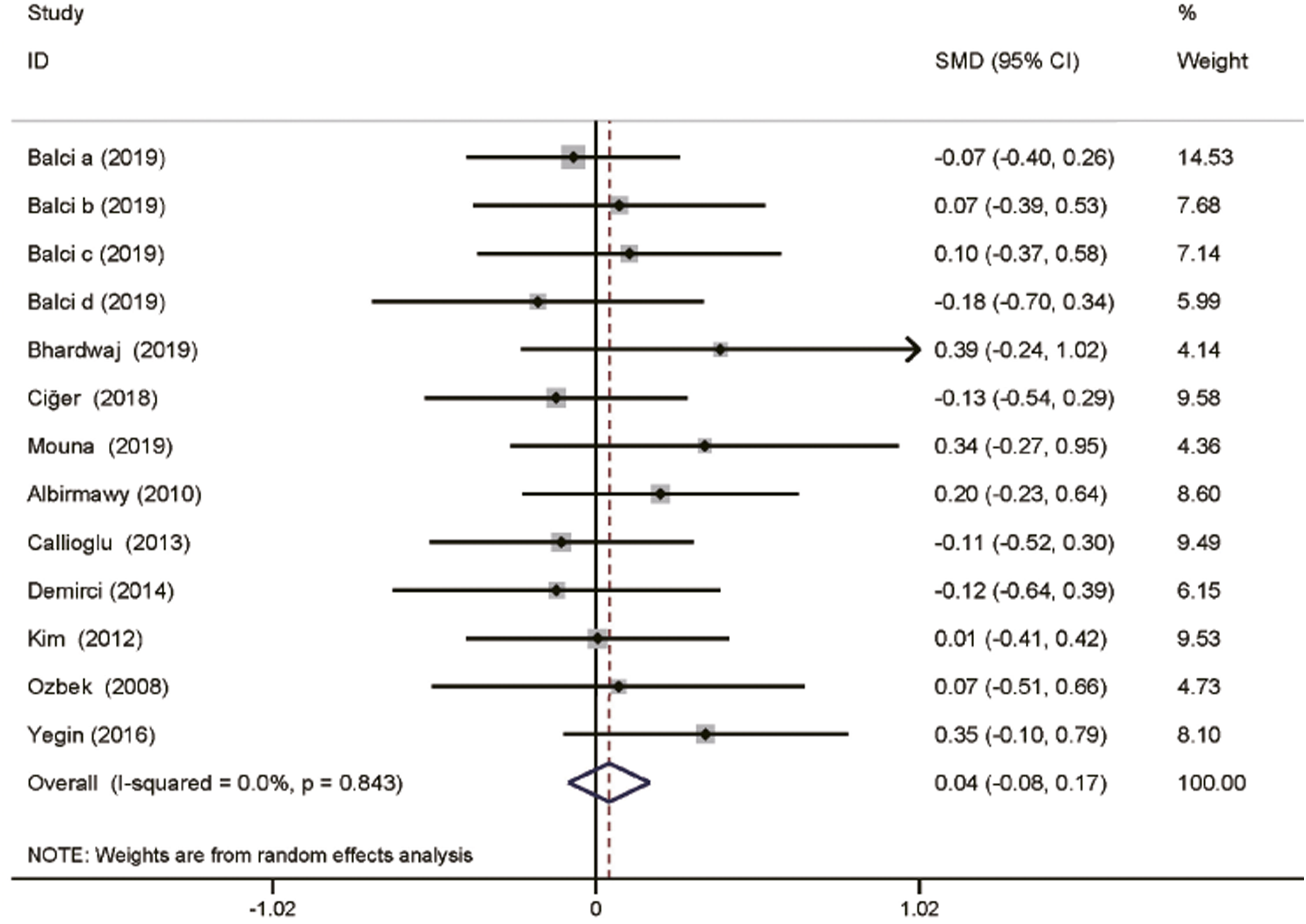
For the mean post-operative ABG, 23 included studies with 2689 patients were available for analysis.5,16-18,22,23,25,29,31,33,35,37-43,45,49,51,53 There was no obvious evidence of heterogeneity among the trials. The overall SMD was −.13 (95% CI: −.23-.03; P = .009; Figure 4). In the palisade, island, and inlay butterfly graft subgroups, the analysis was not significantly different (P = .56, P = .65, and P = .40, respectively; Figure 4). Data regarding mean ABG gain (Figure 5) were available for 10 included studies with 1114 patients.13,15,17,25,31,33,35,40,45,53 The analysis showed no significant difference between the cartilage grafts and TF grafts (SMD: .04; 95% CI: −.08-.17; P = .51; Figure 5). Mean post-operative ABG in chronic otitis media patients after type 1 tympanoplasty with temporalis fascia and cartilage grafts. (A) Pooled analysis of mean post-operative ABG, (B) subgroup analysis with cartilage technique. ABG: air-bone gap. Mean ABG gain in chronic otitis media patients after type 1 tympanoplasty with temporalis fascia and cartilage grafts. ABG: air-bone gap.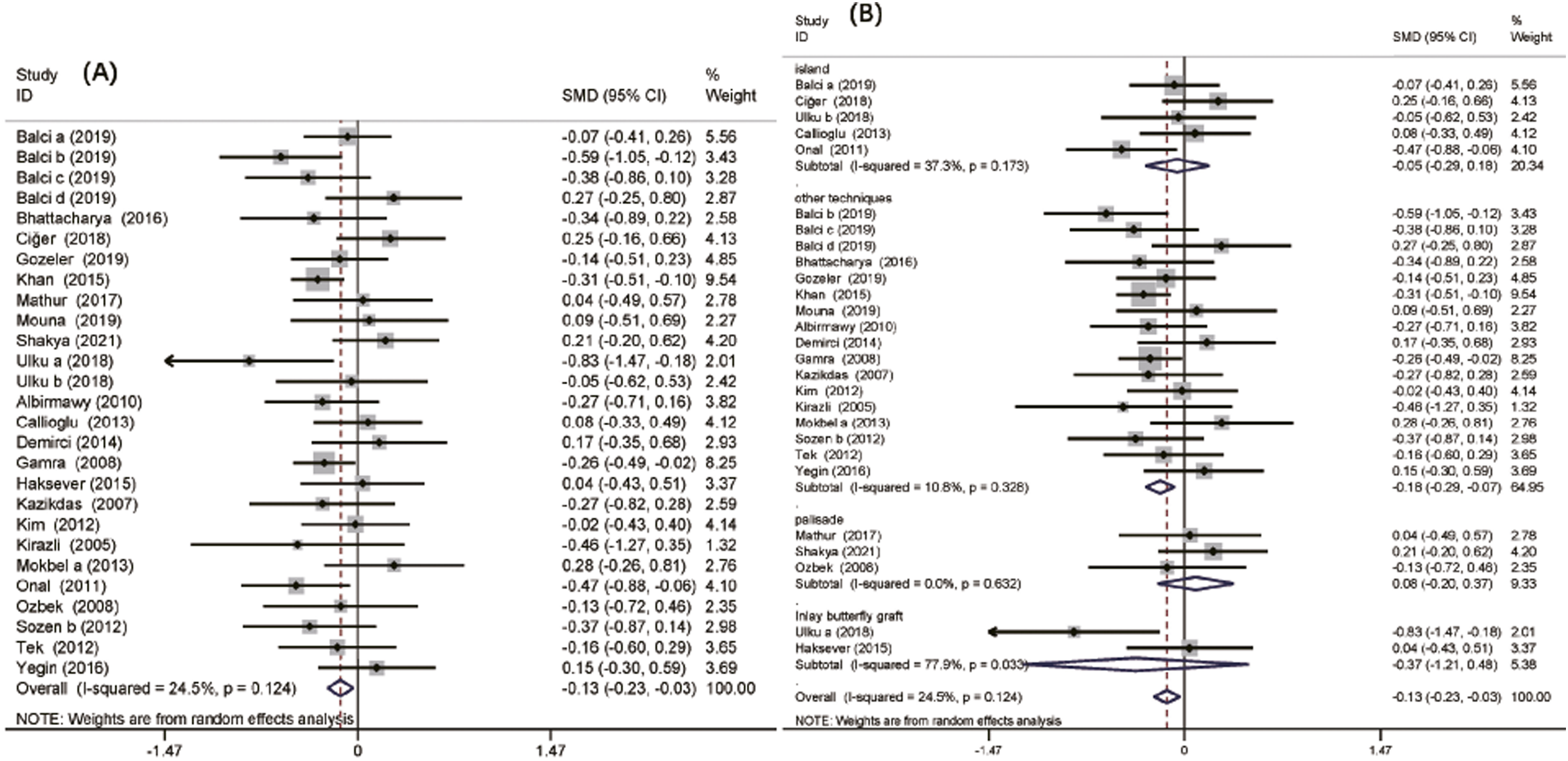
Mean pure tone audiometry
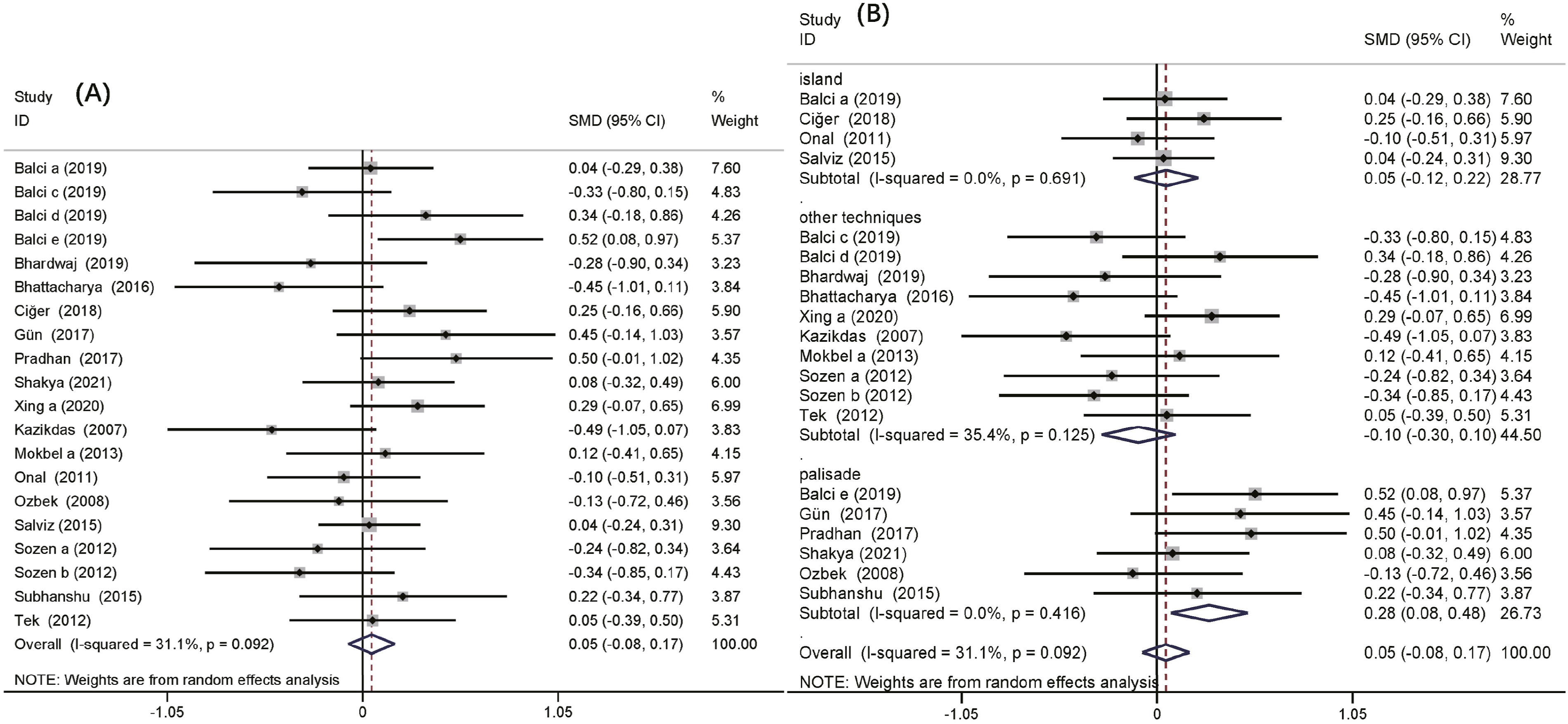
Data regarding mean PTA gain (Figure 6) were available for 8 included studies with 1361 patients.13,16,17,19,30,37,46,51 There was no obvious evidence of heterogeneity among the trials. The analysis showed no significant SMD between the cartilage grafts and TF grafts (SMD: −.10; 95% CI: −.25-.03; P = .14). The SMD for the mean post-operative PTA from 16 studies with 1707 patients was .05 (95% CI: −.08-.17; P = .45; Figure 7), and the difference was not significant.5,13,15-17,20,28,30,39,42,43,45,46,49-51 However, in the palisade cartilage graft subgroup, the SMD for the mean post-operative PTA was .28 (95% CI: .08-.48; P = .007; Figure 7), and the difference was significant, which means that the palisade cartilage grafts resulted in a better hearing outcome than the TF grafts. Mean PTA gain in chronic otitis media patients after type 1 tympanoplasty with temporalis fascia and cartilage grafts. PTA: pure tone audiometry. Mean post-operative PTA in chronic otitis media patients after type 1 tympanoplasty with temporalis fascia and cartilage grafts. (A) Pooled analysis of mean post-operative PTA, (B) subgroup analysis with cartilage technique. PTA: pure tone audiometry.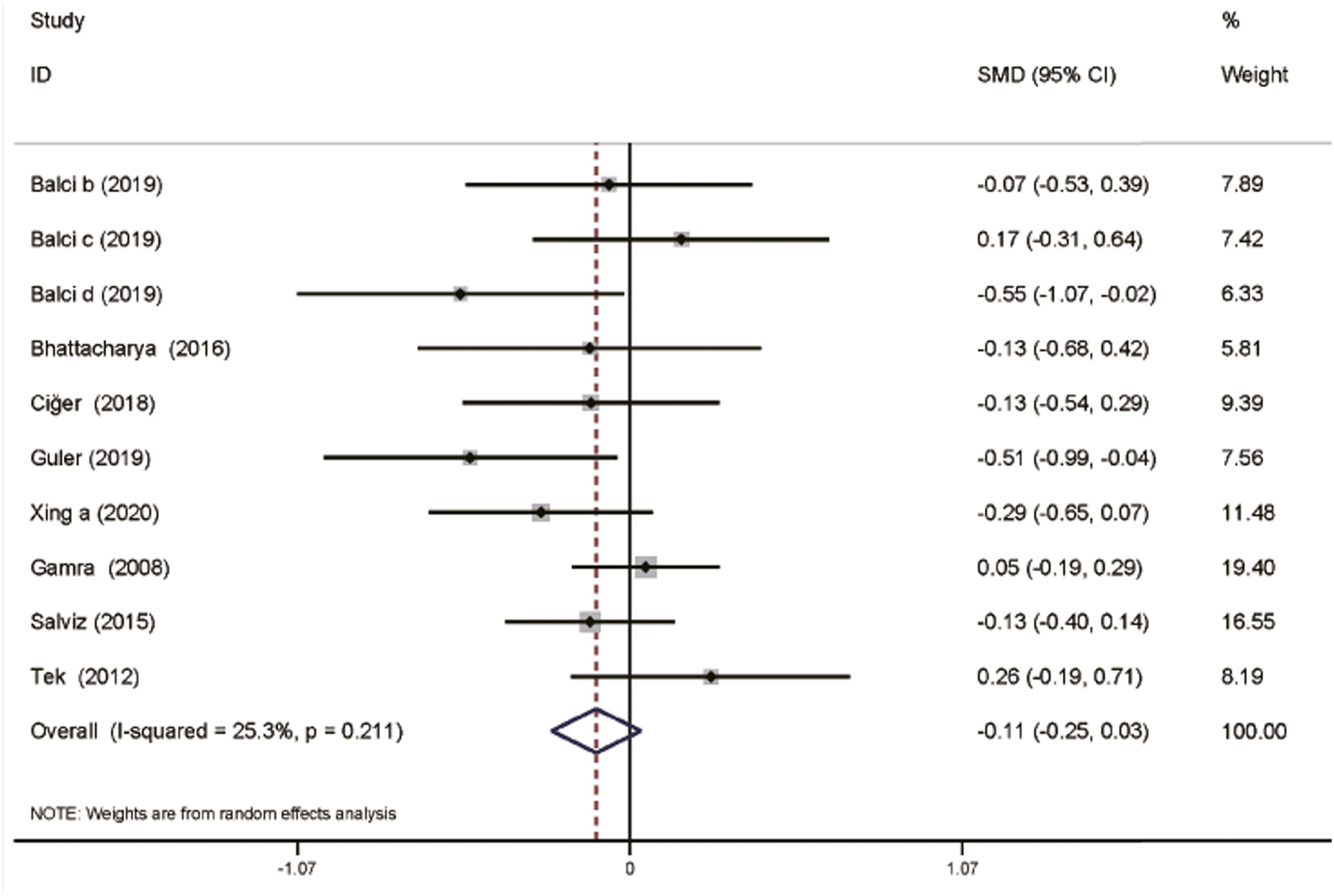
Discussion
Summary of main results
Our comprehensive meta-analysis included a large number of samples from different studies, 33 retrospective studies, and 11 prospective studies involving 4582 patients, investigating the efficacy between cartilage and TF grafts in type 1 tympanoplasties. The present meta-analysis showed that among the reported study population, the overall morphologic success rate of cartilage grafts was higher than TF grafts. In the palisade cartilage and island grafts subgroups, the morphologic success rate was significantly different. However, there was no significant difference in the inlay butterfly grafts and TF grafts subgroups. There was no significant difference in the functional success rate. The meta-analysis revealed that TF grafts had less mean post-operative ABG for hearing outcomes. However, in the palisade, island, and inlay butterfly grafts subgroups, hearing improvement was not significantly different from that of the TF grafts. Analysis was not significantly different in hearing improvement compared to TF grafts. Furthermore, no relevant difference was found between cartilage and TF grafts in the analysis of mean ABG gain. For PTA, there was no significant difference in the hearing improvement of the two groups. However, the palisade cartilage graft subgroup resulted in a better hearing outcome than the TF grafts in terms of the mean post-operative PTA.
Overall completeness, quality, and applicability of the evidence
For the success rate, we carefully scrutinized the included studies to ensure that we included the patients’ unique data and two outcomes: morphologic success and functional success. Similar to previous studies,56-58 cartilage grafts are superior to TF grafts in terms of the morphologic success rate of tympanoplasty. Subgroup analysis of palisade and island grafts compared with TF grafts revealed a significant difference in the morphologic success rate favoring cartilage tympanoplasty. Nevertheless, there was no discrepancy in the result of the inlay butterfly graft subtest. More studies with larger sample sizes are needed to clarify this observation in the future. We found no significant difference in the functional success rate between cartilage grafts and TF grafts. These differences can be explained by the following reasons: (a) there were few studies included and there was a lack of randomized controlled studies and (b) the length of follow-up was different. Hence, it was impossible to judge the cumulative effect. Accordingly, more studies with larger sample sizes are needed.
Jalali et al 57 showed no significant difference in the ABG closure of <10 dB between the two groups. The subanalysis of prospective studies showed that patients in the TF group had a lower mean post-operative ABG. In our present study, analysis of the mean post-operative ABG revealed the superiority of TF grafts over cartilage grafts. However, there was no discrepancy in the subtest results of the palisade, island, and inlay butterfly grafts. More high-quality randomized controlled research is needed in the future. In agreement with our result, Yang et al 56 showed no significant difference in mean ABG gain between those treated with cartilage grafts and TF grafts.
The mean PTA gain is used to analyze the hearing improvement on cartilage and TF graft tympanoplasties. Our analysis revealed that the TF grafts had a better outcome. However, there was no significant difference between the two groups. Accordingly, more studies with larger sample sizes are required to study mean PTA gain. In addition, there was no significant difference in the mean post-operative PTA between those treated with cartilage grafts and TF grafts. However, the palisade cartilage grafts resulted in a better hearing outcome than the TF grafts for mean post-operative PTA.
Potential bias in the review
Several limitations of our meta-analysis merit discussion: (a) our meta-analysis included several design studies. Therefore, confounding bias for inclusion in the study could not be excluded; (b) larger and more detailed studies are needed to reduce the possible impact of confounding factors such as age, sex, and type of cartilage; (c) due to the inconsistent follow-up time in the included studies and the limited data regarding the follow-up, we were unable to conduct an in-depth analysis of the changes in efficacy between cartilage and TF grafts in type 1 tympanoplasty over time; and (d) there may be publication bias against reports of spuriously inflated effects and positive trends in smaller, retrospective studies.
Implications for clinical practice and research
Based on a large number of studies to date, our meta-analysis revealed that cartilage grafts have a better success rate than TF grafts in tympanoplasty. Both cartilage and TF tympanoplasty provided similar improvements in hearing outcomes. At the same time, TF grafts generate better hearing outcomes than cartilage grafts in post-operative ABG, and palisade cartilage grafts are better than cartilage grafts in post-operative PTA. This may be related to the biological characteristics of the grafts. Further comprehensive and thorough studies need to be conducted.
Footnotes
Authors’ note
The material, which is presented in this manuscript, has not been published or submitted elsewhere.
Author contributions
Kai Chen, design of the study, collected and analyzed data, revised article, final approval, accountable for all aspects; Rui Zhao, collected and analyzed data, drafting, revised article, final approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Approval compliance with ethical standards.