
Abstract
Objective:
To compare the effectiveness of butterfly cartilage tympanoplasty (BCT) with that of conventional surgical approaches in the treatment of tympanic membrane perforations.
Methods:
A systematic search was performed by screening the PubMed, Embase, and Cochrane Library databases up to October 31, 2020. Two coauthors independently identified studies in accordance with the selection criteria. Data were pooled and analyzed via Review Manager version 5.3 and Stata version 12.0 software. The postoperative outcomes were measured and expressed as odds ratios (ORs) and standardized mean differences (SMDs). Additionally, heterogeneity was assessed through the I2 statistic.
Results:
A total of 15 articles were eligible for final inclusion. The OR values for the graft uptake rate, compared to conventional tympanoplasty, were 1.12 (95%CI: 0.56-2.22, I2 = 52%, P = .75) and 1.22 (95%CI: 0.58-2.59, I2 = 0%, P = .60), and the OR compared to fat plug myringoplasty was 3.02 (95%CI: 1.04-8.77, I2 = 0%, P = .04). The qualitative analysis of the hearing results reflected significant postoperative auditory gains with no significant differences between the BCT and control groups, indicating satisfactory and similar postoperative hearing improvement. Moreover, the operation time was shortened (SMD = −2.19, 95%CI: −2.79 to −1.59, I2 = 82%, P < .05), and the postoperative pain was less with the BCT approach.
Conclusion:
Butterfly cartilage tympanoplasty has satisfactory efficacy in terms of anatomical and functional results in small to medium perforations. It reduces operation time and postoperative pain. However, the effectiveness on large perforation requires further assessment by well-designed studies.
Introduction
Tympanoplasty for the treatment of tympanic membrane (TM) perforations generally achieves satisfactory healing and hearing outcome. 1 Tympanoplasty can be approached by endoscopic transcanal or open via postauricular, transcanal, or endaural approaches. However, postauricular and endaural approaches can cause surgical scars, 2,3 whereas the transcanal approach is limited to selected patients in experienced hands. 3 Although tympanoplasty can be performed under local anesthesia, it is typically performed in the operating theaters under general anesthesia with its inherent risks and complications. 4,5 Taking these factors into consideration, it is essential to explore alternatives to improve the efficacy of TM repair. 4 -7
Since its introduction in 1998, 8 butterfly cartilage tympanoplasty (BCT) has been a popular technique to repair TM perforations. 9 -23 The name “butterfly” originated from the cartilage graft which is shaped like butterfly wings prior to insertion into the TM to close the perforations, much like an ear tube. 8 Though this technique is simple, practical, and effective, there is a lack of higher-level evidence investigating the efficacy of BCT in the literature. Most studies have small sample sizes and the postoperative results have been variable. To the best of our knowledge, there is no quantitative analysis that evaluated the effectiveness of BCT, especially for chronic perforations. Hence, the aim of this comprehensive meta-analysis is to assess the effectiveness of BCT for the repair of TMs.
Methods
The analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 24 The research question defined by PICOS format is for patients with TM perforations, can BCT performs similar or better postoperative results comparing to the conventional approach with autografts? 25
Search Strategy and Study Selection
A systematic search was performed by screening the PubMed, Embase, and Cochrane Library databases through October 31, 2020. After removing duplicates, 2 individuals (J.H. and B.M.T.) independently performed each step of the analysis. (Figure 1) A third author (Y.S.) was available when any disagreement was presented between two coauthors. Publications were identified by the Medical Subject Heading (MeSH) terms and text words: (1) butterfly cartilage; (2) inlay cartilage; (3) tympanoplasty, tympanoplasties; (4) myringoplasty, myringoplasties, (5) tympanic membrane(s), tympanic membrane(s); membrane(s), tympanic; eardrum(s); and (6) tympanic membrane perforation; membrane perforation, tympanic; eardrum perforation; perforation, eardrum; tympanic membrane rupture; membrane rupture, tympanic; rupture, tympanic membrane. After removing duplicates and non-English publications, studies were read and selected according to the selection criteria. The eligibility criteria were as follows: (1) patients with TM perforations; (2) patients who underwent BCT in the experimental groups; (3) patients treated by conventional tympanoplasty with temporal fascia, cartilage, or fat plug in the control groups; (4) outcomes reported with detailed data that could be analyzed; and (5) observational (prospective or retrospective) studies or randomized control trials (RCTs). The exclusion criteria were as follows: (1) use of xenogeneic, allogeneic, or other biomaterial scaffolds; (2) studies without control groups; (3) qualitative studies without detailed data; and (4) case reports, reviews, letters, animal studies and in vitro studies.
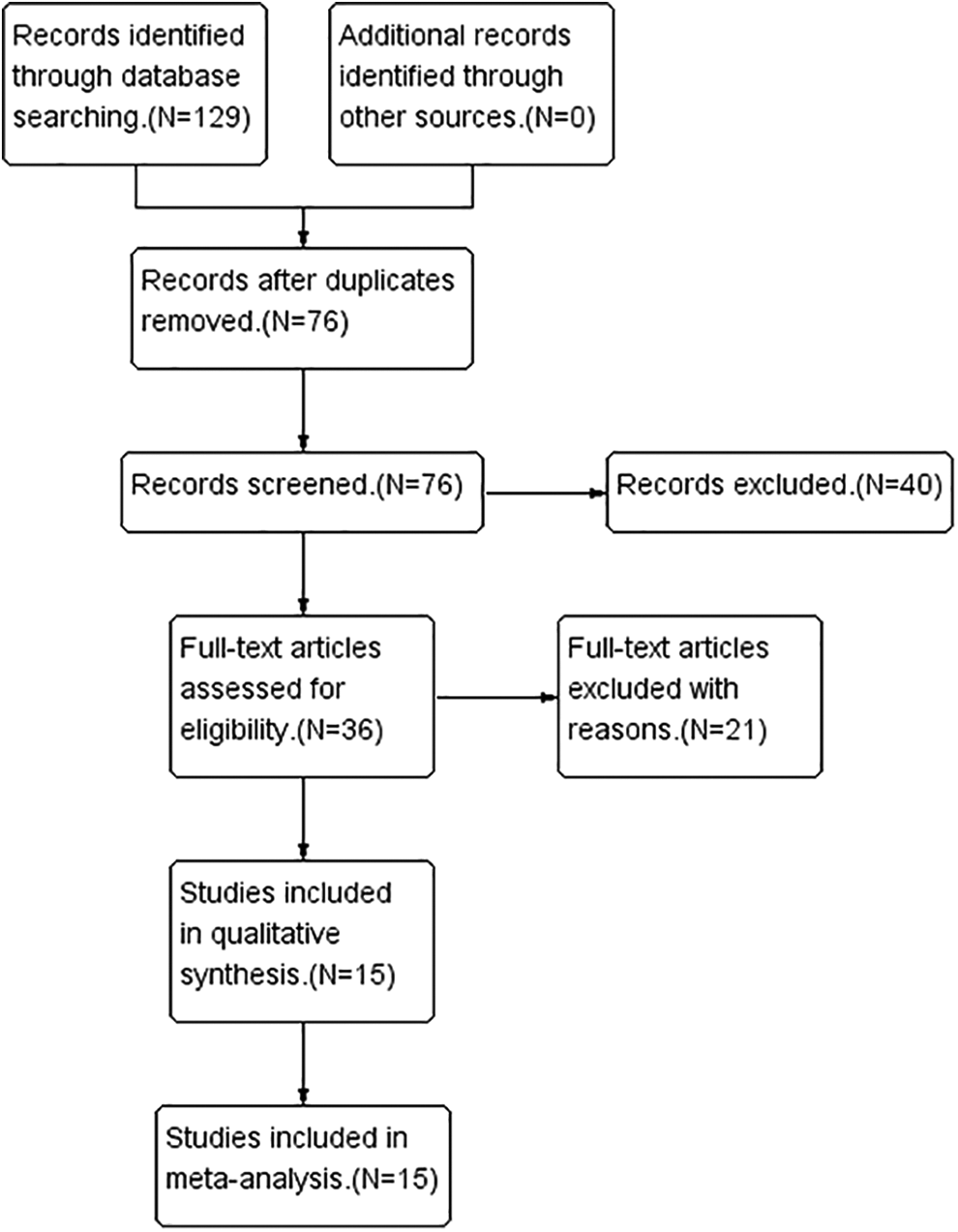
Flow diagram of the search process and search outcomes.
Quality Assessment
Subsequently, the quality of the included RCTs was judged according to the Cochrane Collaboration’s tool to assess the risk of bias among the following 7 areas: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, selective outcome reporting, and other sources of bias. 25 The symbols “+”, “?”, and “−” indicate a low, unclear, and high risk of bias, respectively. For non-RCTs including retrospective and prospective studies, the quality assessment was performed by the use of the Newcastle-Ottawa scale. 26,27 The checklist included the following 3 categories: study selection (maximum, 4 stars), comparability of the cohort (maximum, 2 stars), and assessment of outcome (maximum, 3 stars). 26,27
Statistical Analysis
Information about the included studies was extracted and summarized in Table 1. The primary outcome measure was the complete graft uptake rate in the BCT versus the control group. The secondary outcomes were the differences in hearing improvements, operation time, postoperative pain response, complications, and costs. The following data were taken or derived from the full report of the included studies for both the treatment and control groups: (i) number of subjects, (ii) percentage of closure, (iii) mean and standard deviation (SD) of operation time in minutes, and (iv) mean and SD at 3 or 4 air conduction thresholds frequencies in decibels (dB) obtained via standard pure-tone audiometric testing. Pooled data were then calculated via Review Manager version 5.3 software with the appropriate models. The graft uptake rates and incidence of postoperative pain between the BCT and control groups were compared and expressed as odds ratios (ORs). Furthermore, the operation times and postoperative pain scores were described as the standardized mean differences (SMDs). Subgroup analysis was performed according to grafts applied in the control groups. I2 was applied to assess the heterogeneity. A sensitivity analysis was performed via Stata version 12 software to test the reliability of the results. In addition, the trim-and-fill method was used to revise the results if publication bias was determined to be present by Begg’s funnel plot test. 28,29
Quality Assessment of Included Studies in Meta-Analysis.
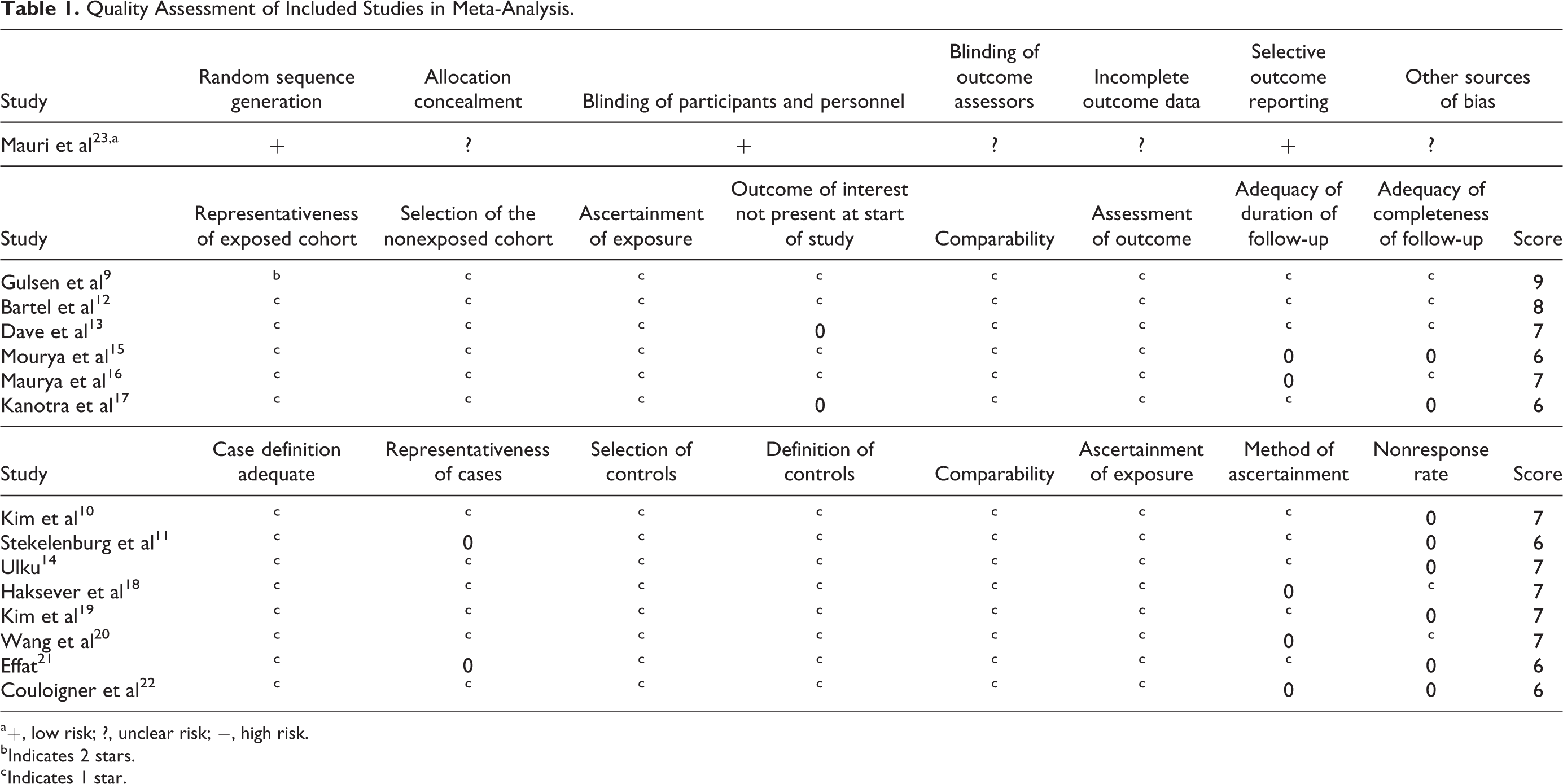
a +, low risk; ?, unclear risk; −, high risk.
b Indicates 2 stars.
c Indicates 1 star.
Results
A total of 15 studies fulfilled the selection criteria and were included. These included one RCT, 23 6 prospective studies, 9,12,13,15 -17 and 8 retrospective studies. 10,11,14,18 -22 These eligible studies were published between 2001 and 2020, with a minimum follow-up period of 3 months. Across the treatment groups, 15 groups underwent BCT, 11 underwent temporal fascia tympanoplasty (TFT), 5 had cartilage tympanoplasty (CT), and 2 underwent fat graft myringoplasty (FGM). Within these studies, data with the last outcome carried forward were used rather than data for only those who completed the study. Detailed information about the included studies is listed in Table 1, including the study design, years, number of ears, participant age, follow-up time, and treatments. Moreover, the results of the quality assessment are described in Table 2.
Characteristics of Studies Included in the Meta-Analysis.
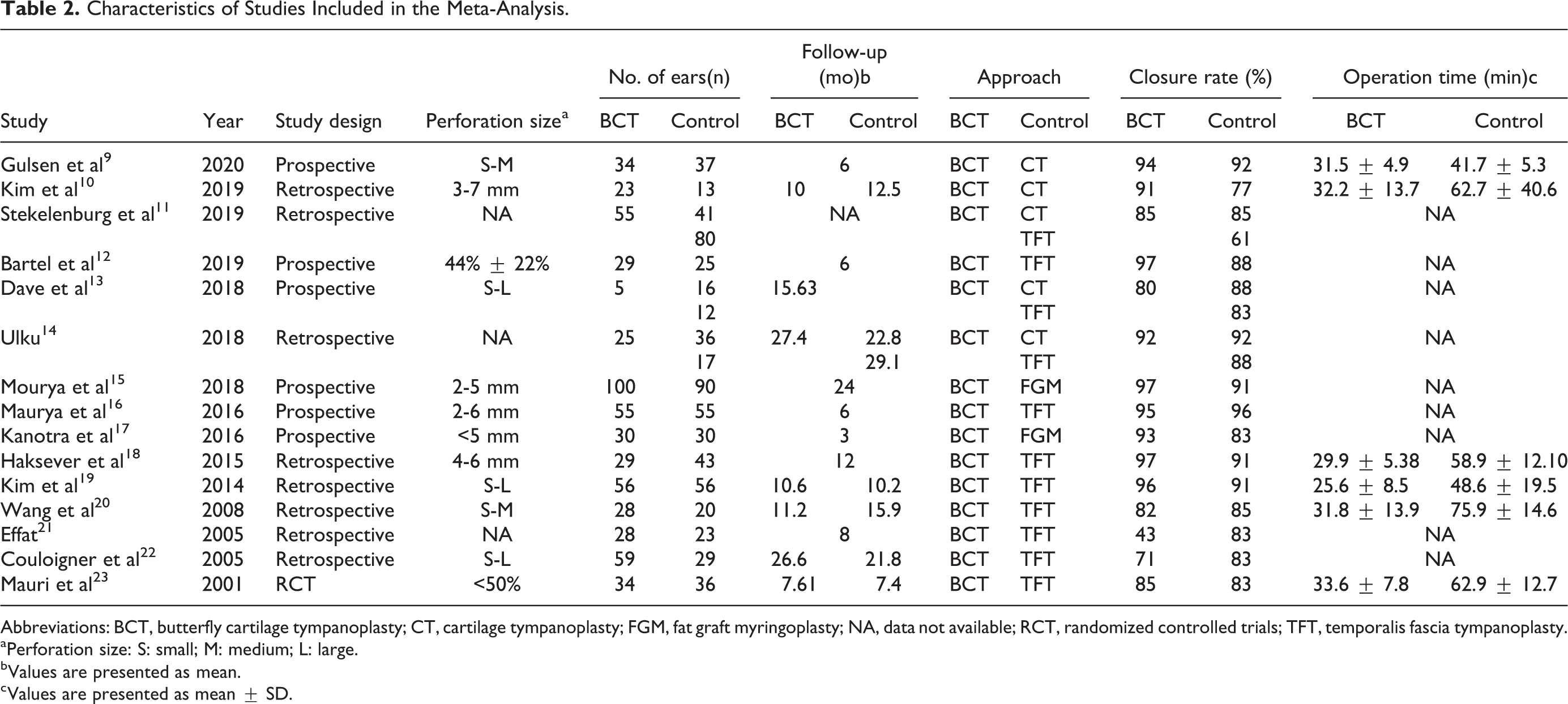
Abbreviations: BCT, butterfly cartilage tympanoplasty; CT, cartilage tympanoplasty; FGM, fat graft myringoplasty; NA, data not available; RCT, randomized controlled trials; TFT, temporalis fascia tympanoplasty.
a Perforation size: S: small; M: medium; L: large.
b Values are presented as mean.
c Values are presented as mean ± SD.
Graft Uptake Rates
Graft uptake rates were analyzed as subgroups according to the different autografts in the control groups. Among comparisons to the temporal fascia, the graft uptake rates in the BCT groups ranged from 43% to 97% (median 85%), compared with those in the TFT groups ranging from 61% to 96% (median 85%). The closure rates in the BCT groups ranged between 80% and 94% (median 91%) versus those in the CT groups ranging from 77% to 92% (median 88%). For FGM, the uptake rates were 93% and 97% in the BCT groups, comparing 83% and 91% in the FGM groups. A fixed-effects model was applied to compare the effectiveness of BCT with that of CT and FGM, but a random-effects model was used due to the high heterogeneity in comparison to the TFT groups. The OR values for these 3 subgroups were 1.12 (95%CI: 0.56-2.22, I2 = 52%, P = .75), 1.22 (95%CI: 0.58-2.59, I2 = 0%, P = .60) and 3.02 (95%CI: 1.04-8.77, I2 = 0%, P = .04), respectively. The outcomes of the graft uptake rate indicate that BCT achieves similar closure rates as TFT and CT but higher closure rates than FGM (Figure 2).
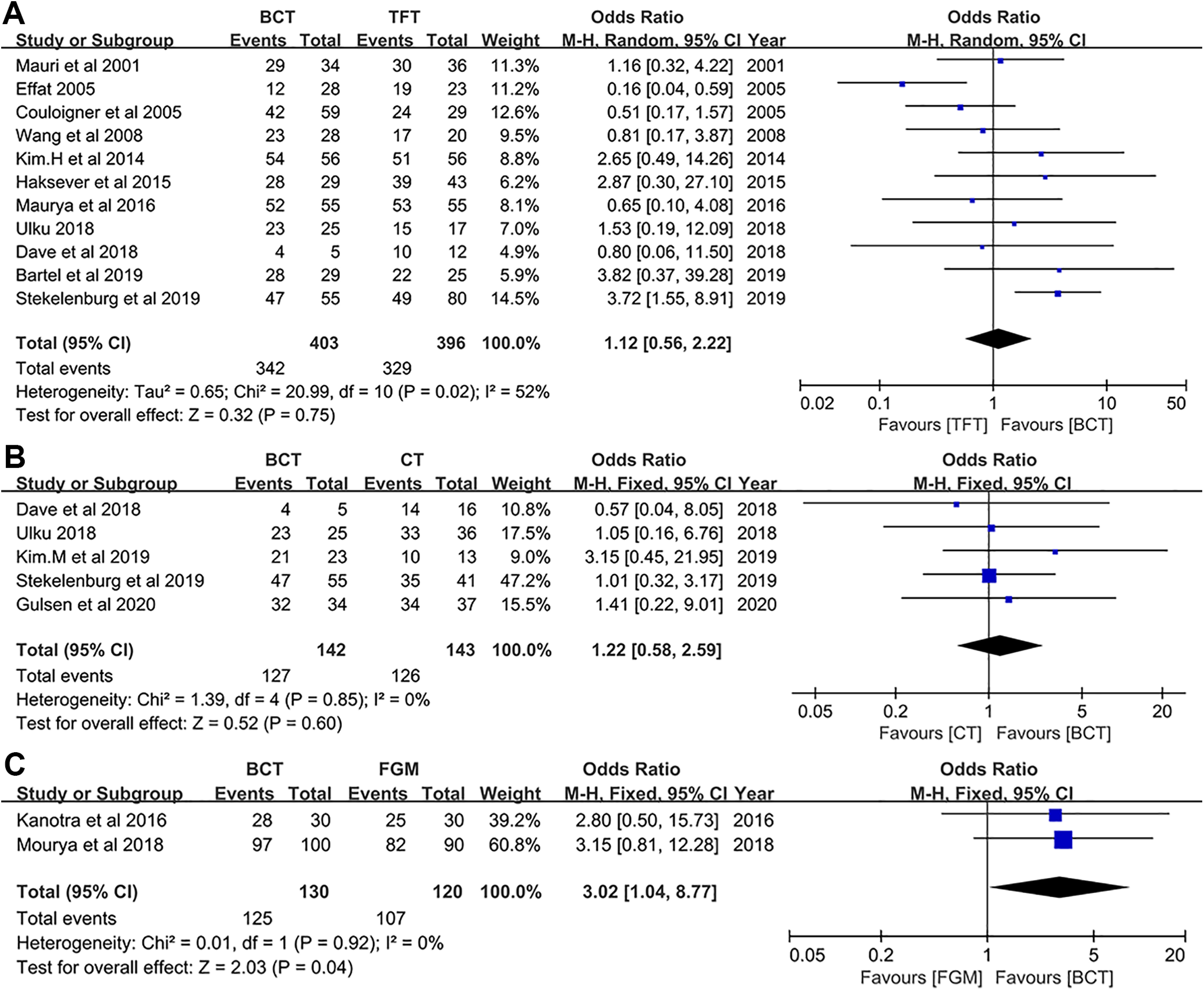
Forest plot of graft uptake rates between BCT and control groups. (A) BCT vs TFT, (B) BCT vs CT, (C) BCT vs FGM. BCT indicates butterfly cartilage tympanoplasty; CT, cartilage tympanoplasty; TFT, temporal fascia tympanoplasty.
Hearing Improvements
A total of 10 articles 9,10,12 -15,18 -20,23 reported hearing improvements. The data are listed in Table 3 and expressed as the mean and SD or the number of patients for the 3 groups. The hearing improvements were described as preoperative and postoperative air–bone gaps (ABGs) or ABG gains measured as the preoperative ABG minus the postoperative ABG at an average of 3 or 4 frequencies. Air–bone gaps were grouped into 3 subgroups, and functional success was defined as a postoperative ABG less than 20 dB. According to the included studies, the auditory results were improved, with a significant difference between preoperative and postoperative ABGs. However, there were no significant differences between the BCT and control groups, suggesting similar hearing gains for these approaches. A further quantitative analysis was not performed due to the data being expressed for different frequencies.
Hearing Results About Included Studies.
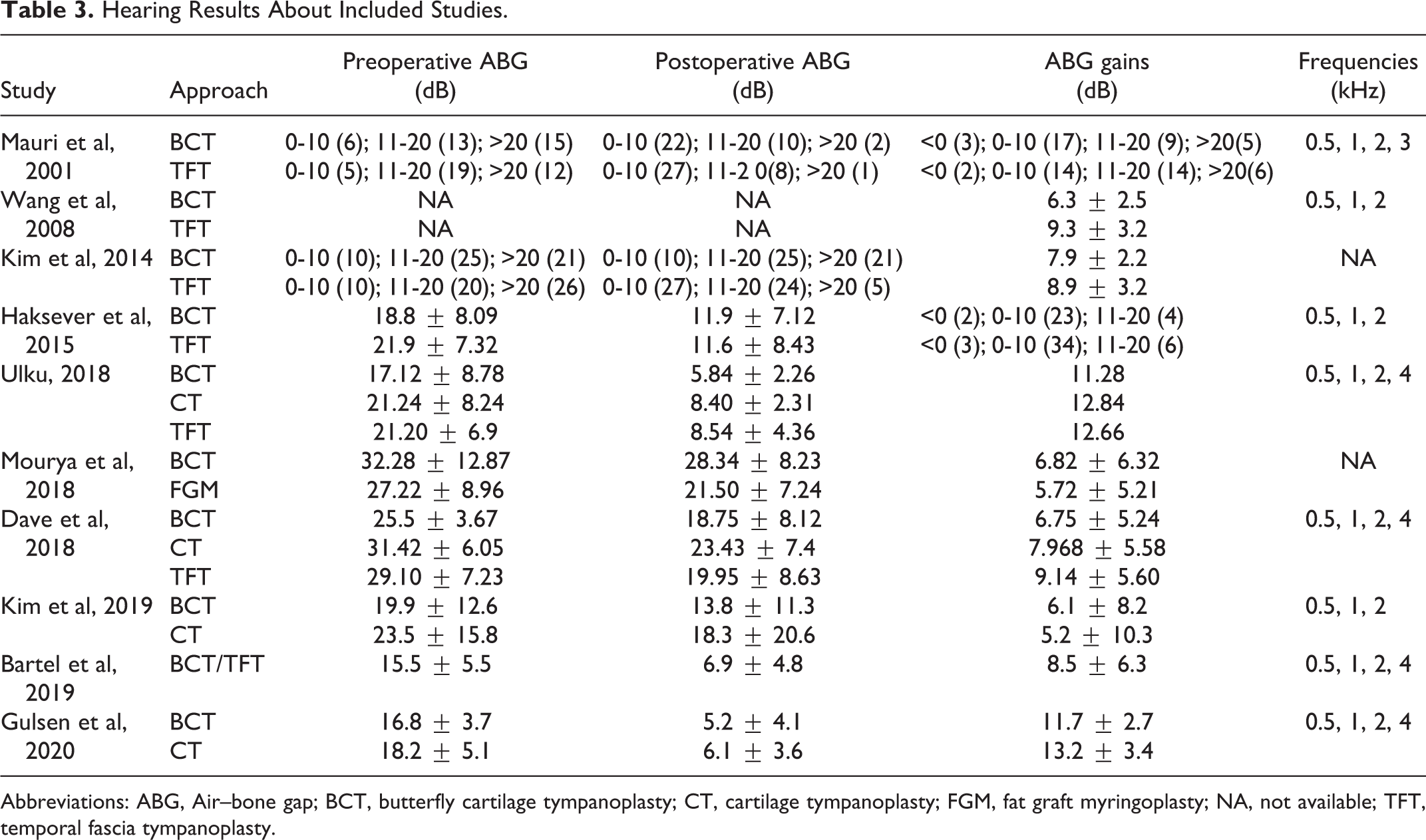
Abbreviations: ABG, Air–bone gap; BCT, butterfly cartilage tympanoplasty; CT, cartilage tympanoplasty; FGM, fat graft myringoplasty; NA, not available; TFT, temporal fascia tympanoplasty.
Operation Times
Six studies 9,10,18 -20,22 investigated the operation time for the surgeries, including 4 comparisons to TFT and 2 comparisons to CT. The average operation times in the BCT groups were 32.2 and 31.5 minutes, compared with those in the CT groups of 62.7 and 41.7 minutes. For comparison with the TFT group, the BCT groups’ operation times were 25.6, 29.9, 31.8, and 33.6 minutes, compared to those of the TFT groups, which were 48.6, 58.9, 75.9, and 62.9 minutes, respectively. According to the random-effects models, the total SMD for the operation times was −2.19 (95%CI: −2.79 to −1.59, I2 = 82%, P < .05), indicating shorter operation time compared with conventional tympanoplasty. The SMDs in the subgroup analysis were −2.50 (95%CI: −3.32 to −1.69, I2 = 85%, P < .05) and −1.58 (95%CI: −2.41 to −0.75, I2 = 69%, P < .05), which also coincided with previous studies suggesting that the use of BCT can significantly decrease the operating time (Figure 3).
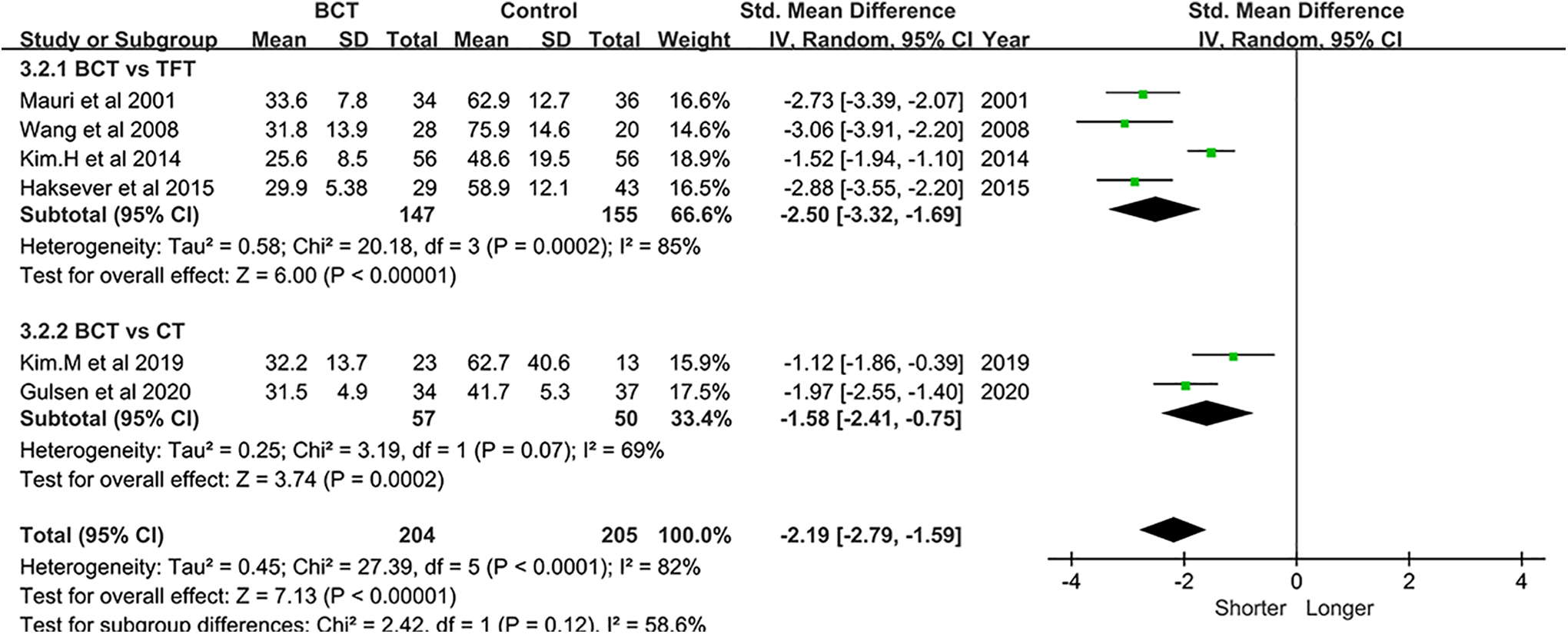
Forest plot of operation time between BCT and control group. BCT indicates butterfly cartilage tympanoplasty; CT, cartilage tympanoplasty.
Postoperative Pain
Postoperative pain assessment was performed via the visual analog scale score and was ranked into 5 levels according to the scores: no pain (0), mild pain (1-3), moderate pain (4-6), severe pain (7-9), and the worst pain (10). Three of the included studies investigated pain and expressed the results as the mean ± SD or the percentage of patients who responded to pain. Referring to these 3 articles, 19,20,23 there were fewer patients who felt pain (31/60 vs 50/56), and the average pain scores in BCT were 1.7 ± 1.2 and 1.5 ± 1.2, compared to those of the TFT groups, which were 4.6 ± 1.9 and 4.9 ± 1.7. As shown in the forest plot with the fixed-effects model (Figure 4), the percentage of pain responders between the BCT and TFT groups was expressed by an OR of 0.09 (95%CI: 0.03 to 0.26, I2 = 0%, P < .05), indicating a lower incidence of postoperative pain in the BCT groups. Similarly, the SMD for the postoperative pain scores was −2.15 (95%CI: −2.55 to −1.74, I2 = 18%, P < .05), suggesting less pain experienced with BCT. All these data indicated that BCT produces less postoperative pain than TFT.
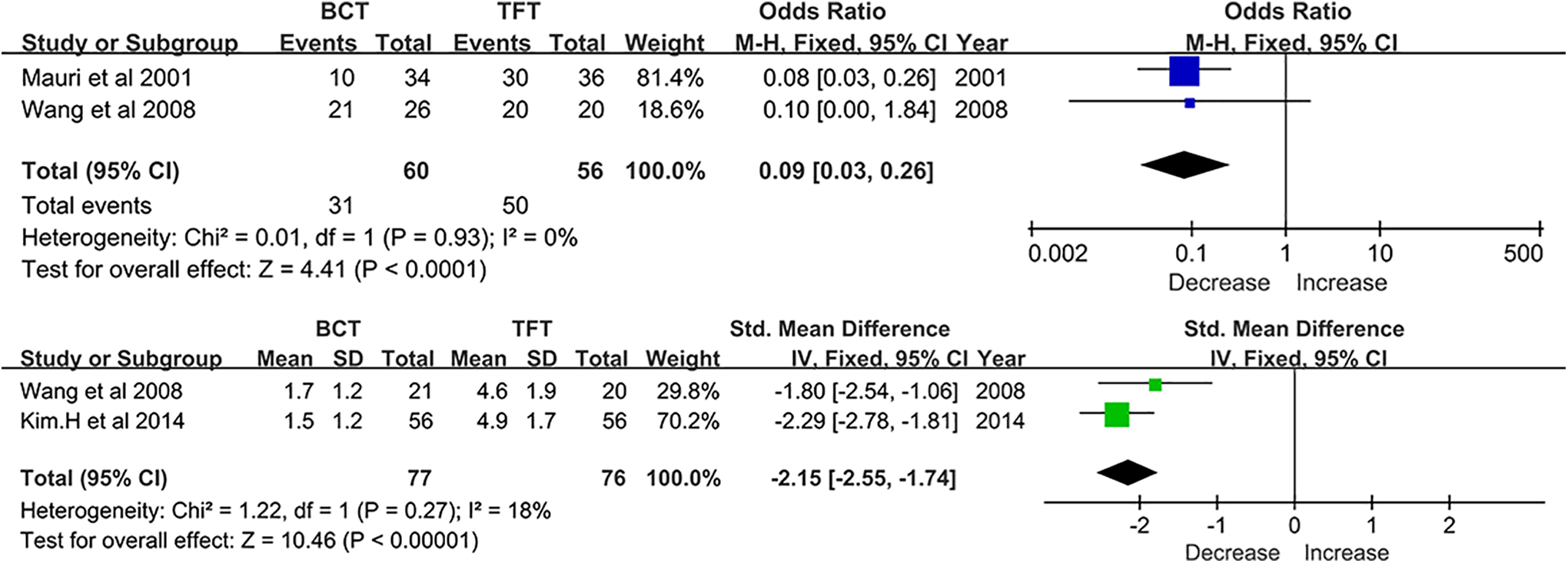
Forest plot of postoperative pain assessment between BCT and TFT group. BCT indicates butterfly cartilage tympanoplasty; TFT, temporal fascia tympanoplasty.
Postoperative Complications
Several cases of postoperative complications were reported in 6 eligible articles, 9,10,13,15,22,23 including reperforations, infections, myringitis, retraction pockets, granulations, lateralization, and medialization. No iatrogenic hearing loss or residual cholesteatoma was reported for the included studies. Due to the variety of complications being reported in different articles, a further statistical comparison was not performed to evaluate the incidence of complications.
Medical Costs
Only one of the included articles 23 compared the costs of surgeries. The estimated charge for BCT in this institution was 65% less expensive than that for underlay CT.
Sensitivity Analysis and Publication Bias
The sensitivity analysis was conducted via Stata version 12.0 software and did not change the results of the analysis, which reflects the reliability and stability of the results. There was also no presence of publication bias after being tested by Begg’s funnel plot.
Discussion
Generally, surgical approach and choice of graft in tympanoplasty depend on patient factors (eg, availability of graft, previous surgeries, immune, and nutrition status), disease factors (eg, site and size of perforations, presence of cholesteatoma, scarring, mucosal disease, and Eustachian tube dysfunction), surgeon factors (eg, preference and training), and institutional factors (eg, availability of biomaterials). 1,6,7 Currently, underlay technique using a temporal fascia graft is the preferred method in primary tympanoplasty. 3,30 However, underlay technique needs elevation of the tympanomeatal flap which can potentially injure the ossicles, tympanic annulus, and chorda tympani, with its associated morbidity. 31 Fat graft myringoplasty is minimally invasive typically performed under local anesthesia, however, the earlobe fat graft achieves less anatomic and functional success in large perforations. 32,33 Butterfly cartilage tympanoplasty is also minimally invasive and a success rate of up to 100% for repairing TM perforations has been reported. 8 However, the impact of BCT on TM repair requires quantification with larger numbers of patients.
Both healing and hearing results serve as important standards to evaluate the effectiveness of a surgical approach. 1,4,5,7 With regard to primary outcomes and graft uptake, BCT and conventional tympanoplasty with a temporal fascia or cartilage graft achieve similar closure rates. Nevertheless, when compared with FGM, it performs better, with an OR of 3.02. Previous studies also supported these results that BCT achieves satisfactory graft uptake rates for TM repair. 9 -23 Furthermore, cartilage grafts were preferred in patients with retraction pockets, Eustachian tube dysfunction, chronic mucosal dysfunction, and residual or reperforation. 34,35 Although the auditory gains may theoretically be influenced by the thickness and rigidity of the cartilage, 36 the results with short-term follow-up suggest identical ABG closure between cartilage and fascia grafts, 37,38 which coincides with our qualitative analysis. For long-term postoperative hearing gains, cartilage grafts seem to achieve even better hearing gains compared with the temporal fascia for large perforations. 38 In our study, the enrolled patients had simple chronic TM perforations instead of other severe middle ear disorders, and hearing improvements were mostly assessed with short-term follow-ups. Thus, supported by the previous clinical evidence, the hearing results of our analysis can be considered reliable despite the lack of further quantitative analysis.
Similarly, patients who underwent BCT suffered less pain and discomfort in the postoperative period. The minimal incision without ear packing, canalplasty, or tympanomeatal flap elevation can significantly decrease postoperative discomfort. 7,34 However, in terms of postoperative complications, there is limited evidence to reveal which approach has the lowest incidence. Mauri et al. 23 reported 6 cases of postoperative infection in the BCT group and 15 cases in the TFT groups, suggesting less postoperative morbidity with BCT. Nevertheless, Couloigner et al 22 reported similar reperforation rates between the BCT and TFT groups albeit 5 cases of retraction pockets were observed in the BCT group (zero in the TFT group). Other studies also indicated similar or no incidence of complications after surgery. 9,10 The cartilage graft lacks vasculature and receives its nutrition from the attached perichondrium. 23 In dry ears, a cartilage graft with perichondrium on one or both sides has better viability than totally naked cartilage, 39 which may significantly decrease the risk of infections and reperforation. It was also suggested that closure should be obtained with an underlay cartilage graft in cases of contralateral tympanic retraction or otitis media with effusion. 22 Therefore, it is crucial to explore options to improve the outcomes while minimizing complications.
Based on our analysis, the total SMD for operation time was −2.19, indicating that BCT can significantly shorten the time spent in surgery. As a minimally invasive approach, BCT avoids tympanomeatal flap elevation 7 and it can be performed easily with the assistance of an endoscope, 9 thereby shortening the operation time. 3,28 Additionally, BCT can be performed in adult patients under local anesthesia as an outpatient procedure, 40 with reduced morbidities and health care costs. Particularly, one-session BCT endoscopic surgeries can be performed simultaneously in patients with bilateral perforations, 40,41 which reduces the pain, risks, and costs associated with 2 separate operations. 40 -42 For surgeons, the BCT technique is easy to learn and perform. Stekelenburg et al indicated that butterfly grafts had good success rates when used by both experienced surgeons (87.1%) and intermediate surgeons (88.9%). 11 Even when operated on by inexperienced surgeons, the success rate can reach 66.7%.
Although the anatomic and functional results of BCT paralleled those of conventional tympanoplasty, some factors still remain to be considered. In recent decades, the BCT approach mainly focused on perforations that are small to medium in size. 10 As Kim et al described in their article, there is not enough TM remnant to stabilize the cartilage grafts when the perforation sizes are larger than 7 mm. 10 However, Ghanem et al extended its indications and applied BCT in the treatment of perforations larger than half of TMs. 43 Although there is a need to elevate medial canal wall skin to expose the bony annulus, 44,45 several studies reported high closure rates in large perforations. 13,19,46 Hence, for patients with small to medium size, simple and central perforations, especially bilateral or residual perforations, BCT is an excellent alternative. For large perforations, the effectiveness of BCT remains to be further assessed. Moreover, since tympanomeatal flaps are not raised, it may be difficult to assess the ossicles and middle ear cavity. Thus, for patients with middle ear diseases (eg, ossicular chain discontinuity), a conventional underlay approach with fascia or cartilage would be more appropriate. In addition, it can be technically challenging to produce a butterfly wing-shaped cartilage. 44,46 Better anatomic results were achieved when the graft diameter was fashioned to be at least 2 mm larger than the perforation. 22 Heavier weight and pressure of the graft may tear the fibers and affect the blood supply of the TM, resulting in graft failure. 47 Hence, it is essential to precisely measure the size and shape of the perforation in relation to the size of the cartilage graft to reduce errors caused by inaccurate visual observation and judgment. 48 Importantly, a meticulous middle ear evaluation is necessary as the opacity of cartilage may hide diseases (eg, cholesteatoma) behind the TM 23 ; this could be assisted with an endoscope. 49 In addition, some factors may limit the application of this technique such as the size of perforation, type of perforation (marginal), perforation involving malleus handle or ossicular chain erosion, adhesive otitis media, presence of cholesteatoma, and revision cases.
There are several limitations in our study. The main limitation is that majority of eligible studies were non-RCTs without a well-designed control group. To reduce the heterogeneity caused by multiple factors (eg, small sample size), well-designed RCTs with large populations are warranted. Moreover, the effectiveness of BCT for the treatment of large TM perforations needs to be further investigated. Most studies included in this analysis were based on a short-term follow-up which was less than a year; evaluations on long-term results are warranted in future studies. Therefore, future studies should focus on long-term healing and hearing results.
Conclusion
Butterfly cartilage tympanoplasty has satisfactory efficacy in terms of anatomical and functional results for the treatment of small to medium TM perforations. Moreover, this procedure is well tolerated with high patient satisfaction, reduced operation time, and postoperative pain. However, the effectiveness for the repair of large perforations needs further assessment by well-design studies.
Footnotes
Acknowledgment
All authors have participated sufficiently in the work to take public responsibility for the content of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No. 81670920), Zhejiang Provincial Natural Science Foundation (No. LY15H130003), Zhejiang Provincial Medical and Health Science Research Foundation (No. 2020RC107), Ningbo Natural Science Foundation (No. 2018A610363), and Ningbo Huimin Technology Research and Development Project Fund (No. 2015C50026).