
Abstract
Objectives
This study aimed to define the best electrode trajectory line in cochlear implant (CI) surgery using the OTOPLAN (otology planning software) reconstructed 3D model and to investigate the surgical distance of the retro-facial approach as a direct access to the round window.
Methods
Computed tomography (CT) scans of the normal temporal bone were included for analysis in this study. OTOPLAN reconstruction was used to build 3D models with specific ear structures for study analysis.
Results
Twenty-five scans were included; the average age at the time of CT scan was 6.8±12 years. Twelve scans (48%) were right-sided and thirteen (52%) were left-sided. The best trajectory line to the round window was identified in all scans. The retro-facial approach was the optimal approach for 52% of cases (13/25). In all scans, the safe distance from the facial nerve were in favor of the retro-facial approach (P = 0.0011).
Conclusion
The OTOPLAN reconstructed imaging provided a good analysis of the retro-facial approach and helped in planning the surgical trajectory line towards the round window. Additionally, calculation of the surgical distance can help the surgeon compare the retro-facial approach to the standard facial recess for preoperative planning. These findings may help in robotic surgery.
Introduction
Cochlear implants provide a good management option for hearing rehabilitation and language development in patients with severe to profound hearing loss. 1 The surgical procedure to place cochlear implants requires accuracy. It needs to be performed by a specialized surgeon, and every effort should be taken to ensure that surgical complications are avoided. 2
Identification of the skull base level, sigmoid sinus, facial nerve, chorda tympani, and opening of the round window (RW) are crucial steps in any cochlear implant surgery. In some delicate areas, surgeons only have a few millimeters as the average safe working distance, and this needs to be maintained to avoid surgical trauma. Therefore, a good review of the radiological imaging prior to any implant surgery is an important step to check for cochlear deformity and to choose an appropriate electrode. It also helps the surgeon to identify the borders of the posterior tympanotomy, namely, the mastoid segment of the facial nerve, chorda tympani, and fossa incudis that indicate the access to the RW. 3 Although this step is helpful for all cochlear implant surgeries, it is of particular interest in cases using a minimally invasive surgical approach.4,5
With the increasing number of cochlear implants being used, a combination of inputs from surgeons and technological developments by cochlear implant companies has been used to ensure that safe and effective surgeries are carried out. However, drilling of the facial recess is a highly demanding task for a surgeon, with the level of experience of the surgeon impacting the final result. The overall risk and the number of procedures performed could matter in that regard and the overall risk could be minimized by incorporating a surgical assistance method with imaging data.6-8
In 2003, Raine et al. 9 first documented a case of an ossified cochlea in which an image-guided implant was placed using a navigation system. One year later, Schipper et al. 10 published a study about image-guided surgery to demonstrate its potential benefit in preserving intra-cochlear structure with cochleostomy. Subsequently, further research conducted in that field led to the principle of robotic percutaneous cochlear implants, in which imaging data is used to build a model for precise drilling from the lateral skull surface to the cochlea.11,12
The retro-facial approach was primarily used for access to the sinus tympani for the removal of cholesteatoma.13-17 Later, it was used for difficult cochlear implant surgeries, 17 as well as coupling the Vibrant Soundbridge implant to the RW.
In this study, we planned to define the best electrode trajectory line in cochlear implant surgery by using a computed tomography (CT) scan to reconstruct a 3D model of the temporal bone with specific software. The secondary objectives were to investigate the feasibility of the retro-facial approach as a direct access to the RW and to classify the size of the retro-facial approach in relation to the size of the facial recess.
Patients and Methods
Twenty-five CT scans of the temporal bone were included for analysis in this study. CT images were used by the radiology department prior to that date as part of the preoperative work-up for cochlear implant candidates in our center. The inclusion criteria were cases with high-resolution CT scans of the temporal bone with a normal anatomy, with a section thickness of 1 mm, and that were suitable for upload and analysis by OTOPLAN (otology planning software), which was developed by CAScination (Bern, Switzerland) in cooperation with MED-EL (Innsbruck, Austria). It uses CT-based reconstructions to create a 3D model with specific ear structures.
The included scans were uploaded for the following steps:
A. Imaging preparation:
For each scan, a cochlear view was defined based on specific parameters (Figure 1A). A: OTOPLAN view is used to define cochlear parameters (diameter, width, height) in the axial, coronal, and sagittal views. B: All parameters are included to build the 3D model. C: A 3D model is used for the facial recess approach. D: A 3D model is used for the retro-facial approach. Red = basal turn of the cochlea; yellow = facial nerve (FN); orange = chorda tympani, posterior semicircular canal; purple = sigmoid sinus; pink = ossicles; blue = external canal; light blue = the trajectory line towards the round window.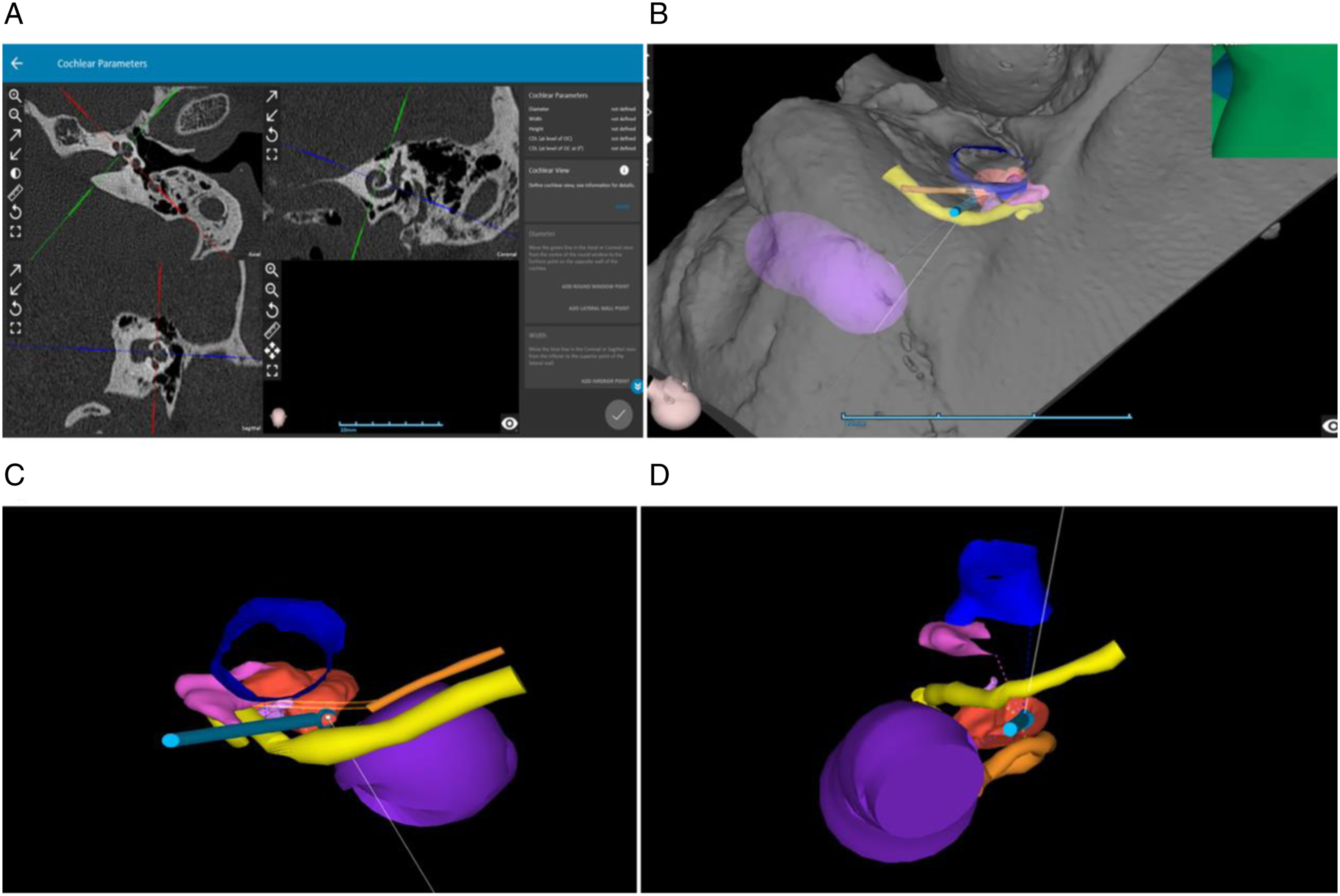
Additional ear structures were defined in a stepwise fashion by choosing different scan points for each structure in the 3 views.
The defined structures included: the ear canal, incus and malleus, stapes, chorda tympani, posterior semicircular canal (SCC), sigmoid sinus, facial nerve, cochlear bony overhang, and RW, and the 3D model was finally built based on these parameters (Figure 1B).
B. Defining the trajectory line:
The 3D model was used to define the ideal trajectory line from the mastoid surface to the basal turn of the cochlea through the RW (Figure 1C,D). In the first step, the best access based on cochlear anatomy defines the ideal trajectory line.
Based on that definition, we had 3 approaches: the retro-facial, trans-facial, and facial recess approaches.
In the second step, the scan with a trans-facial approach as the ideal access was further modified to either a retro-facial or facial recess approach, based on the available safe distance, as the best available surgical option for the surgeon to avoid injury to the facial nerve.
C. Classification of retro-facial approach in cochlear implant:
Classification for the size of the retro-facial approach.
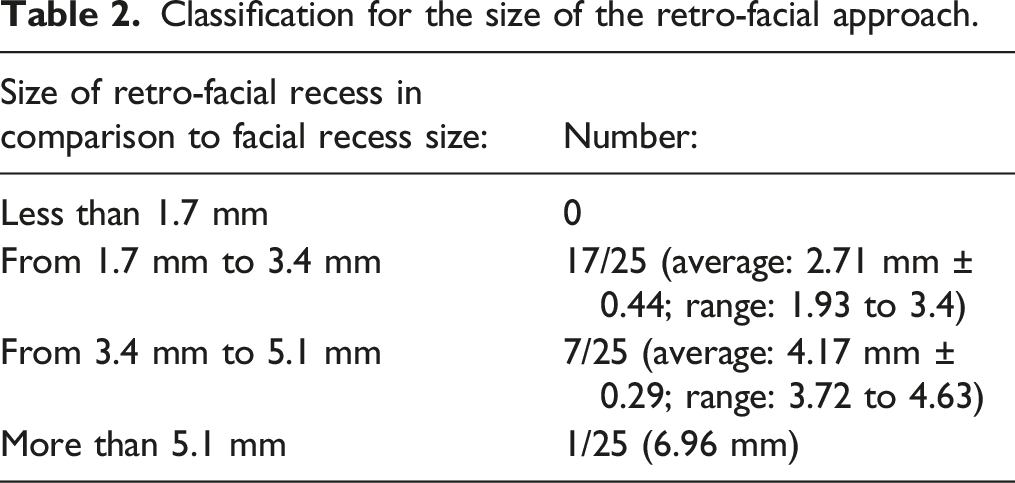
We chose the widely used approach (facial recess) as a reference for the classification: the minimum facial recess size was 1.7 mm, calculated by allowing for 0.4 mm safety margins to the facial nerve and 0.3 mm to the chorda using a 1-mm drill bit.
The retro-facial approach was classified into 4 categories: 1. Less than 1.7 mm was the “minimum facial recess size.” 2. From 1.7 mm to 3.4 mm was “double the size of the minimum facial recess.” 3. From 3.4 mm to 5.1 mm was “triple the size of the minimum facial recess.” 4. More than 5.1 mm was “more than triple the size of the minimum facial recess.”
D. Statistical analysis:
All statistical analyses were performed with GraphPad Prism version 8.4.0 (GraphPad Software, La Jolla, CA, USA). The mean, standard deviation, and range (i.e., minimum and maximum value) were used to describe the characteristics of the participants. For comparison of preoperative and postoperative data, the normality of data was first evaluated. Subsequently, the parametric paired t-test was performed to test the significance of the group data with a normal distribution, and the non-parametric Wilcoxon–Mann–Whitney test was used to test the others. Statistical significance was set at P < 0.05.
Results
CT scans of 25 patients’ ears fulfilled the inclusion criteria of this study. The mean age at the time of the CT scan was 6.8 ± 12 years (range: 1 to 50 years). Twelve scans (48%) were right-sided and thirteen (52%) were left-sided. The best trajectory line to the RW was identified in all scans. As Figure 2 shows, the retro-facial approach was the optimum approach in the majority of studied cases (52%), followed by the facial nerve (44% of cases) and facial recess (4% of cases) approaches. The optimum trajectory line through the round window. RF: retro-facial, FR: facial recess, FN: facial nerve.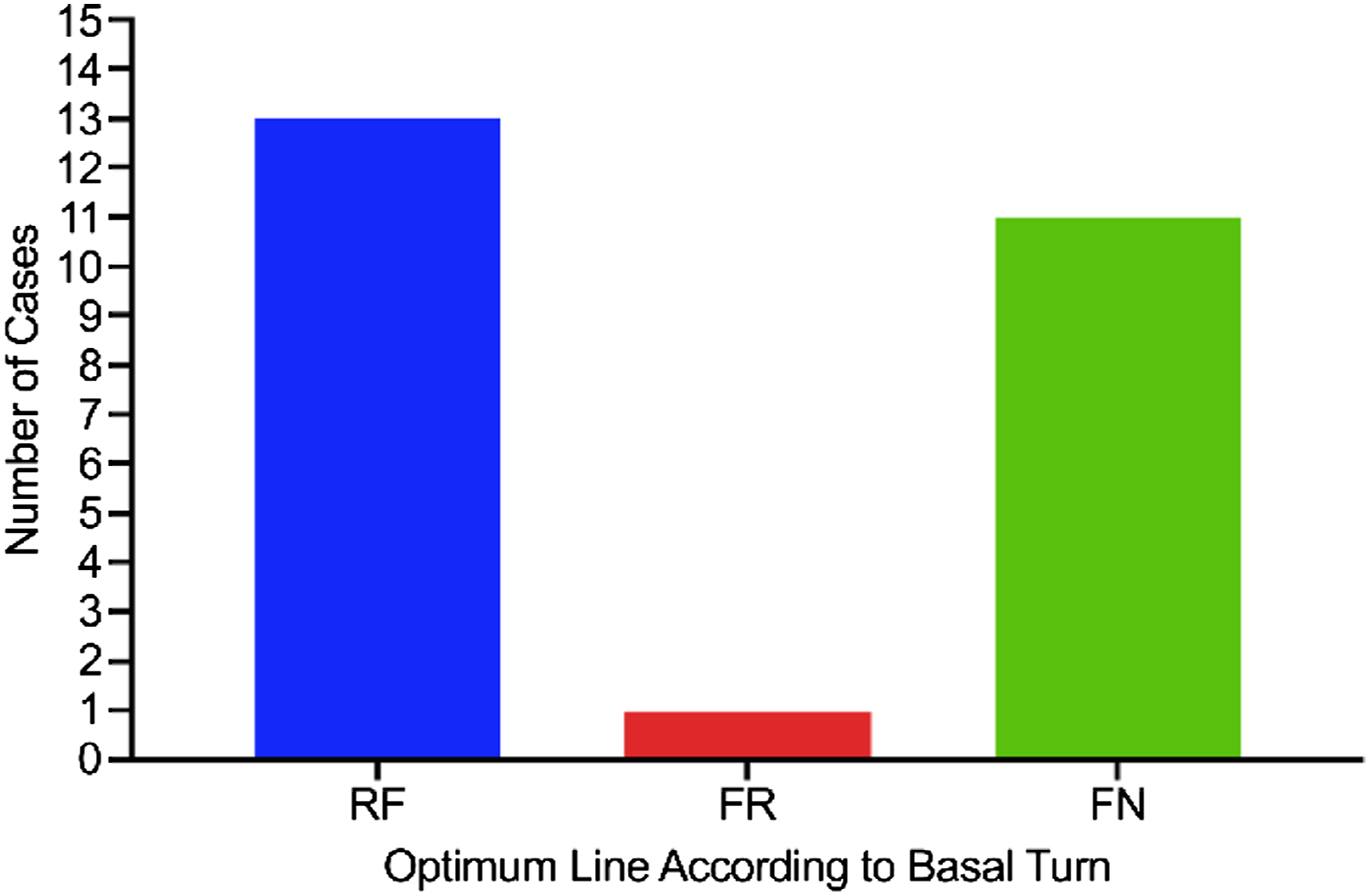
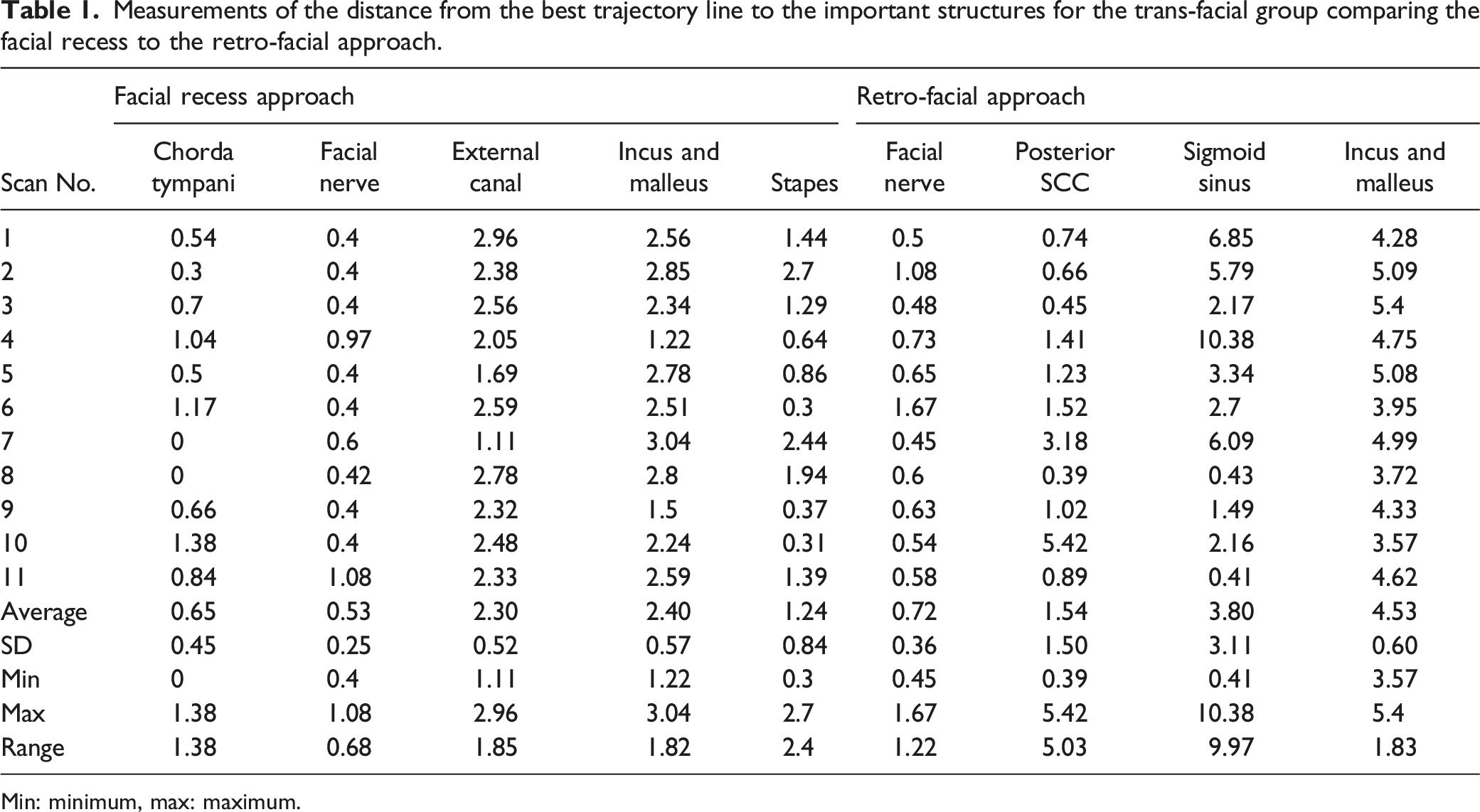
Measurements of the distance from the best trajectory line to the important structures for the trans-facial group comparing the facial recess to the retro-facial approach.
Min: minimum, max: maximum.
Regarding the other important structures of the retro-facial approach subgroup, the average distance was 3.8 ± 3.11 mm from the sigmoid sinus, and 1.54 ± 1.5 mm from the posterior SSC. For the facial recess approach subgroup, the average distance was 0.65 ± 0.45 mm from the chorda tympani and 2.3 ± 0.52 mm from the external auditory canal.
Based on the analysis of all included scans (Figure 3), the safe distance from the facial nerve was statistically better (P = 0.0011) in the retro-facial approach (0.79 ± 0.36 mm) than that in the facial recess approach (0.49 ± 0.19 mm). The safety distances for the facial nerve between the facial recess and retro-facial approaches are shown. RF: retro-facial, FR: facial recess, FN: facial nerve.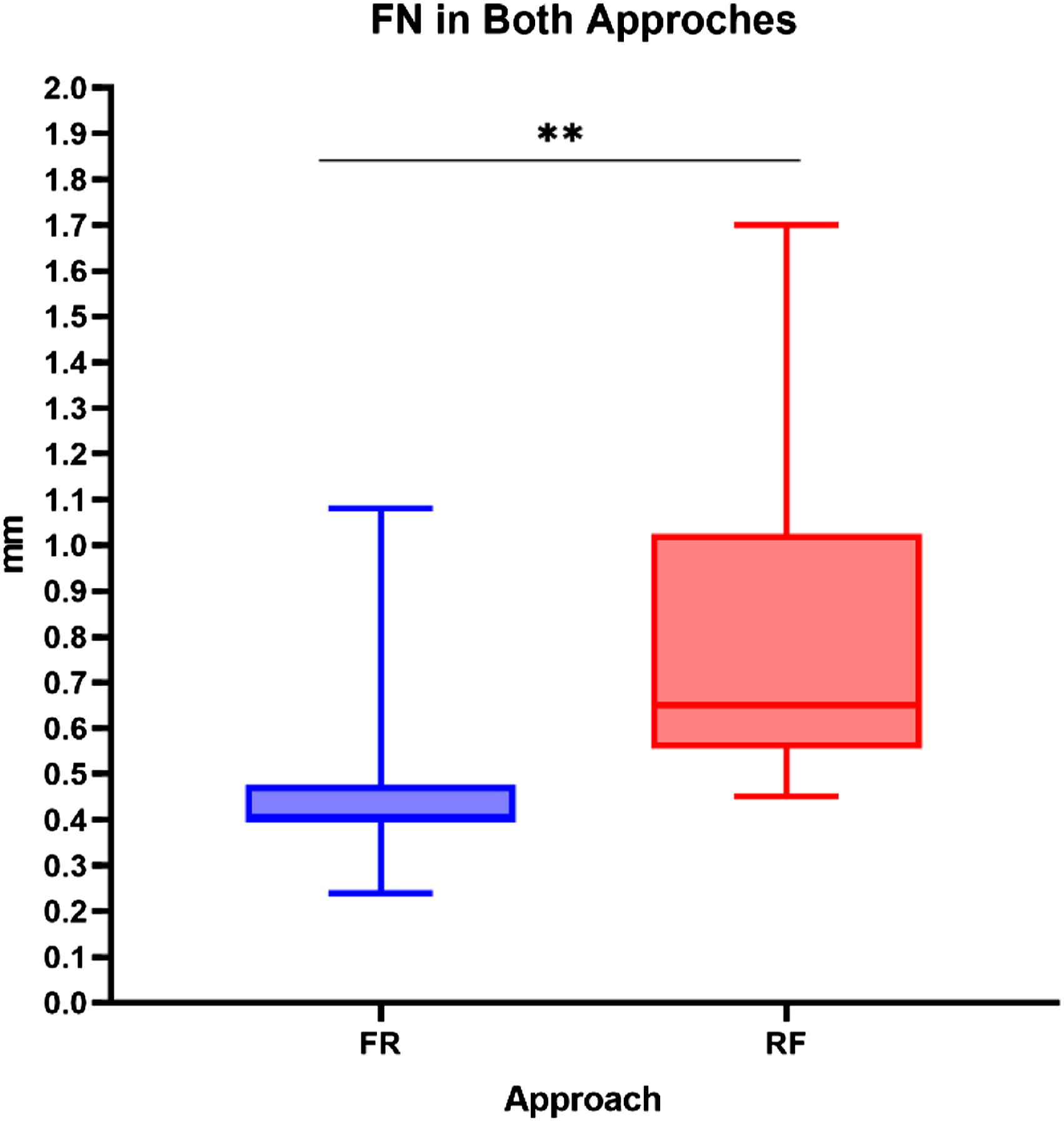
Finally, we followed the new classification method proposed in this work to categorize the retro-facial approach in all studied scans (25 ears) based on the available safe distances. The analysis revealed that 0 ears exhibited the minimum facial recess size. Most of the ears exhibited double the size of the minimum facial recess (68%), 28% exhibited triple the size of the minimum facial recess, and only 4% exhibited more than triple the size of the minimum facial recess.
Discussion
Pulec 15 first description the retro-facial approach in 1996 for cholesteatoma removal from the sinus tympani in the posterior mesotympanum. The drilling was focused in the area bordered superiorly by the lateral SCC, posteriorly by the posterior SCC, and anteriorly by the facial nerve. In almost all temporal bones with normal anatomy, the retro-facial air cells exhibit considerable pneumatization.16,17
We included normal scans in this analysis for which the facial recess approach (posterior tympanotomy) was the preferred technique for cochlear implant placement in most cases. However, the surgeon may need alternative options in some cases, especially if a malformation or anterior displacement of the facial nerve is encountered, as a narrow facial recess may not provide adequate exposure to the RW.
This study showed that, in the majority of scans in the first analysis (13/25, 52%), the retro-facial approach represented the best trajectory line. In the second analysis, 8/11 (73%) scans showed that, based on the best available surgical distance and RW exposure, the retro-facial approach provided the ideal trajectory line for the subgroup with a trans-facial trajectory.
In contrast to cholesteatoma surgery, cochlear implant surgery did not require full exposure of the posterior mesotympanum and sinus tympani. Only the RW area needs to be exposed for electrode insertion.
However, adequate visibility to the RW is an important measure to avoid the risk of the electrode being misplaced to other areas, such as the eustachian tube, air cells of the hypotympanum, and carotid canal.18,19
RW visualization is also vital for atraumatic electrode insertion. Anatomical variations and inner ear anomalies may affect visualization through the standard facial recess in around 7% to 24% of patients during cochlear implant surgery.20,21 In such circumstances, other approaches can be used to improve the visualization, including expansion of the facial recess by scarifying the chorda tympani, canal wall down mastoidectomy with canal closure, the endoscopic trans-canal approach, the combined trans-canal/trans-mastoid approach, and the retro-facial approach.
Surgical training plays a major role in choosing between different approaches. However, the sacrifice ear structures and the addition of steps in the surgical setup (e.g., endoscopy) are important factors to consider. However, the most important factor is the feasibility of the approach in that particular case. Theoretically, the retro-facial approach requires neither the sacrifice of any ear structures nor the addition of equipment, but it remains uncertain what advantages it has over the facial recess approach for RW visualization. An anterior displacement of the sigmoid sinus and high jugular bulb are notable difficulties for the retro-facial approach. It is worth mentioning that this approach can be improved by decompression of the jugular bulb or sigmoid sinus with adequate mastoidectomy. However, we do not recommend the decompression step if the RW is clearly visible without it.
In 1995, Pickett et al. 22 described the anatomical considerations for the retro-facial approach and reported that it is less likely to be affected by the presence of an anterior sigmoid sinus or a high jugular bulb. During the safe distance analysis, we found that, in the retro-facial approach, the average distance of surgical drilling was 3.8 ± 3.11 mm from the sigmoid sinus and 1.54 ± 1.5 mm from the posterior SSC.
In other reports, the average distance between the facial nerve and posterior SCC to the plane of the RW is approximately 2.98 ± 0.41 mm.16,17 The retro-facial approach has advanced from being a part of cholesteatoma surgery to an alternative approach for difficult cochlear implant surgeries. Allen et al. 23 reported on 3 patients who underwent cochlear implantations with the retro-facial approach as an intraoperative decision when the standard facial recess did not provide adequate visualization of the RW. Although they did not report any surgical complications, a preoperative analysis of the images could have helped provide the surgeon with a plan B, which would have saved time and effort. In another report in almost the same period, the retro-facial approach was used in 2 children (3 cochlear implants) with malformed ears. Although the facial recess approach was initially attempted, the RWs could not be visualized despite maximization of the facial recess opening. In the first patient, an intraoperative decision was taken to open the middle ear through a retro-facial approach for full electrode insertion. In the second case, the primary surgery was aborted, and the patient was sent to another senior doctor who performed a subtotal petrosectomy and closure of the external auditory canal to achieve the desired exposure of the RW. However, the exposure remained insufficient. When the surgeon proceeded with a retro-facial approach, full insertion of the cochlear implant electrode was achieved through the RW. 24 From the second case in that series, we concluded that the number of surgical trials could be minimized if the retro-facial approach was considered in the first surgery, keeping in mind the advantages of adequate RW exposure and a safe surgical distance with minimal limitations from the surrounding structures (posterior SSC, sigmoid sinus, etc.).
In this study, the use of OTOPLAN-reconstructed imaging helped us to analyze the retro-facial approach, plan the surgical trajectory, and calculate the surgical distance, but an important novel point was that we could compare this approach to the standard facial recess approach by classifying the different sizes. We believe that this classification will help in the surgical planning of cochlear implant surgeries in the future, and in expanding utilization of the retro-facial approach in other ear surgeries (e.g., for implantation of other devices).
The primary limitation of this study is the small sample; thus, future studies should investigate a larger sample and include cases with abnormal anatomies.
In conclusion, OTOPLAN-reconstructed imaging provided a useful analysis of the retro-facial approach and helped in planning the surgical trajectory line towards the RW. Additionally, the calculation of the surgical distance can help the surgeon to compare the retro-facial approach to the standard facial recess approach during preoperative planning. These findings may also help in robotic surgery.
Footnotes
Acknowledgments
The authors extend their appreciation to the Deanship of Scientific Research at Imam Mohammad Ibn Saud Islamic University for funding this work through Research Group No. RG-21-11-03.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deanship of Scientific Research at Imam Mohammad Ibn Saud Islamic University [Research Group No. RG-21-11-03].
Ethical Approval
The ethics committee of King Saud University College of Medicine approved the study protocol with reference number: 20/0091/IRB.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Verbal informed consent was obtained from legally authorized representatives for anonymized patient information to be published in this article.
Availability of Data and Materials
The datasets used and/or analyzed from the current study are available from the corresponding author on reasonable request.