
Abstract
Background:
The posterior tympanum approach of cochlear implantation is easy to damage the facial nerve and cord tympanic nerve. Therefore, we need to improve the safety of cochlear implantation.
Objectives:
To discuss the safety and feasibility of active and adequate transparent exposure of the facial nerve and chorda tympani nerve during the surgery.
Methods:
A retrospective analysis was performed on all 945 patients who underwent cochlear implantation from January 2011 to September 2017. All patients have been followed up for 14 months to 5 years postoperatively and postoperative complications have been observed.
Results:
All 945 patients received artificial cochlear implantation. The facial nerves of 76 cases were above the horizontal semicircular canal plane, while narrow facial recess was observed in 44 cases. Serious chorda tympani nerve variation was found in 1 case. No facial paralysis and facial nerve irritation and abnormal taste occurred after operation.
Conclusions:
Cochlear implantation with initiative and adequate exposure of facial nerve and the chorda tympani nerve can improve the safety of the cochlear implant surgery. Our study provide a safe and effective method for clinical cochlear implantation to reduce facial nerve and tympanic cord nerve injury.
Introduction
By 2015, there has been over 300 thousand deafness patients who received cochlear implantation around the world. 1 The most common method of cochlear implantation is through mastoid process—posterior tympanic cavity—facial recess approch; the key of this operation was to fully open the facial nerve recess, expose the posterior tympanum, find the round window niche and round window membrane, accurately locate the scala tympani and open the window from the scala tympani, and insert the electrode into the cochlea scala tympani without injury. However, the anatomical structure of the facial recess was small and complex, and it is easy to injure the facial nerve, chorda tympani nerve, and other important structures during the operation. As a result, how to expose facial recess safely and efficiently has become one of the key issues that restrict the further popularization and promotion of cochlear implantation. In our study, we proposed an operation method of exposed facial nerve and chorda tympani nerve actively and adequately, in other words, exposed facial recess extremely, safely, and efficiently, so as to provide guarantee for implanting electrodes smoothly, and reduced the incidence of facial paralysis, taste abnormalities, and other surgical complications at the same time.
Patients and Methods
Clinical Data
A total of 945 patients accepted cochlear implantation from January 2011 to September 2017 in Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, were selected, including 574 males and 371 females, aging from 12 months to 73 years old. There were 901 patients younger than 18 years and 44 patients older than 18 years. All the patients had regular examinations of auditory brain stem response, otoacoustic emission, multiple frequency steady-state response, distortion product otoacoustic emission, and so on, before diagnosed as bilateral profound sensorineural hearing loss. After doing the inspections of the temporal bone lamellar computed tomography (CT) and magnetic resonance imaging thin-slice scan of facial and acoustic nerves, we found 158 patients with large vestibular aqueduct syndrome, 17 patients with Mondini malformation, 45 patients with secretory otitis media, and 2 patients with common cavity deformity.
Operation Method
All the patients have accepted cochlear implantation by approach of mastoid process—posterior tympanic cavity—facial recess under general anesthesia. Exposing the facial nerve and chorda tympani nerve actively and adequately was the specific method during the surgery, and the main points included the following aspects (Figure 1): (1) After the mastoid segment was incised and enlarged, the posterior wall of the external auditory canal was polished and made it as thin as possible. (2) Exposed the vertical segment of the facial nerve and its branch—chorda tympani nerve actively without damaging the nerve sheath. (3) Opened the facial nerve recess between the included angle of the 2 nerves under direct vision. (4) At least 3 radians were exposed after the process of opening the facial recess: the radian of vertical segment and prolong lined from pyramid segment to tympanic segment of the facial nerve; the radian of posterior wall of the external auditory canal and chorda tympani nerve; the radian of pyramidal eminence and stapedius muscle. Round window membrane was exposed after opening the facial recess and then implanted electrode at the 3- to 5-o’clock of the round window membrane. The electrode impedance and nerve reaction was tested, the incision behind the ear was sutured, and the incision was carefully pressure bandaged.
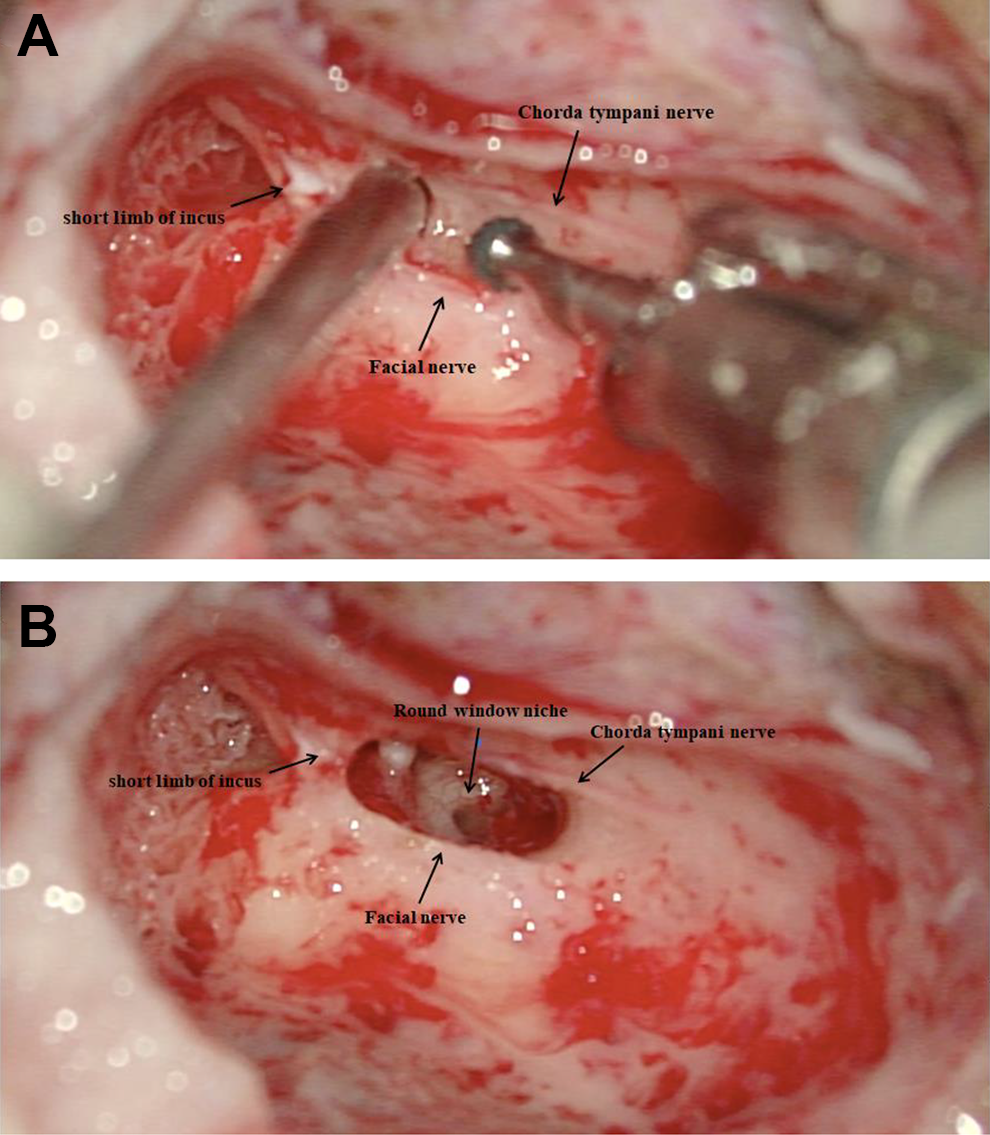
Expose round window in the surgery of cochlear implantation through opening the facial recess. A, Active and adequate exposure of the facial nerve and chorda tympani nerve. Grinding thin facial nerve bone canal, leaving only a thin layer of bony coat on the surface of facial nerve. B, Opening the facial recess between the chorda tympani nerve and facial nerve.
Observation Index and Postoperative Treatment
Counting the number of patients with high facial nerve, facial recess stenosis, and chorda tympani nerve variation, the average time of operation of every month during surgery. The time of surgery was calculated from incision to suture. The wound healing condition should be observed on the second day after surgery, and patients leave the hospital on the fifth day after surgery. The machine outside was invoked 1 month after surgery. Patients were followed up to observe the occurrence of complications, such as facial paralysis, facial nerve stimulation disease, taste abnormalities, external auditory canal inflammation, and so on.
Results
All 945 patients have the facial recess opened and implanted electrodes successfully after exposing the facial nerve and chorda tympani nerve actively and adequately, and all the patient’s facial nerve and chorda tympani nerve were kept intact during operation. The average time of operation was shortened from 75 minutes in January 2011 to 60 minutes in September 2017 as the operation quantity continuously increasing. The shortest operation time was 40 minutes. We found 76 cases of high facial nerve, which was higher than the plane of horizontal semicircular canal (Figure 2), 44 cases of facial nerve preposition, facial recess stenosis which was less than 2 mm (Figure 3), and 1 case of serious chorda tympani nerve variation, which lies transverse above half of the facial recess (Figure 4). All electrodes impedance was detected in the normal range, and all the nerve reaction tests were present during the operation. All the artificial cochlear implants worked normally when the machine outside is invoked 1 month after surgery. All the patients were followed up postoperatively from 14 months to 5 years; none of them was found to have complications of facial paralysis, facial nerve stimulation disease, taste abnormalities, and external auditory canal inflammation.
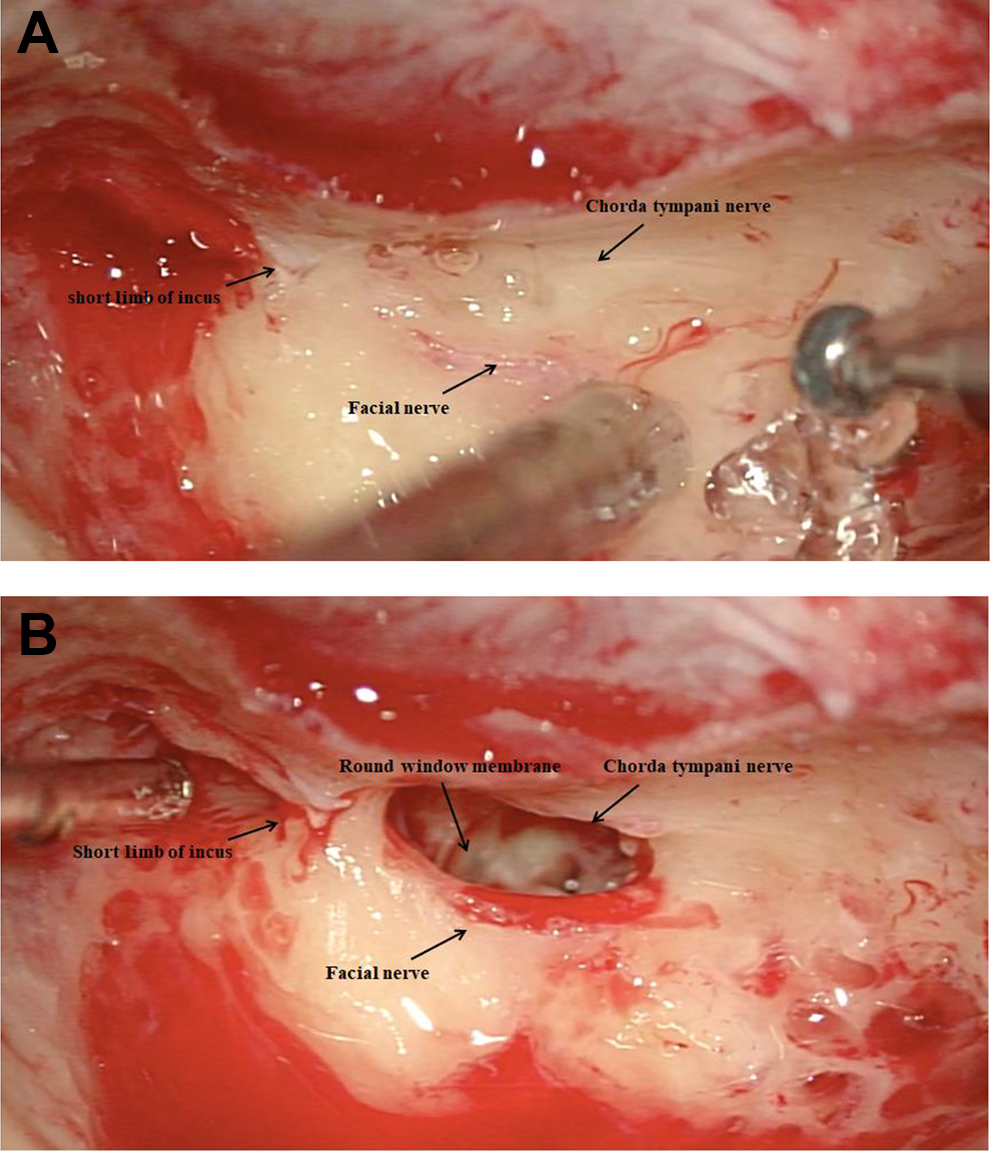
High facial nerve variation. A, High facial nerve was found during the opening the facial recess. B, Full transparency of facial nerve, removal of facial nerve surface bone, and exposure of facial nerve sheath.
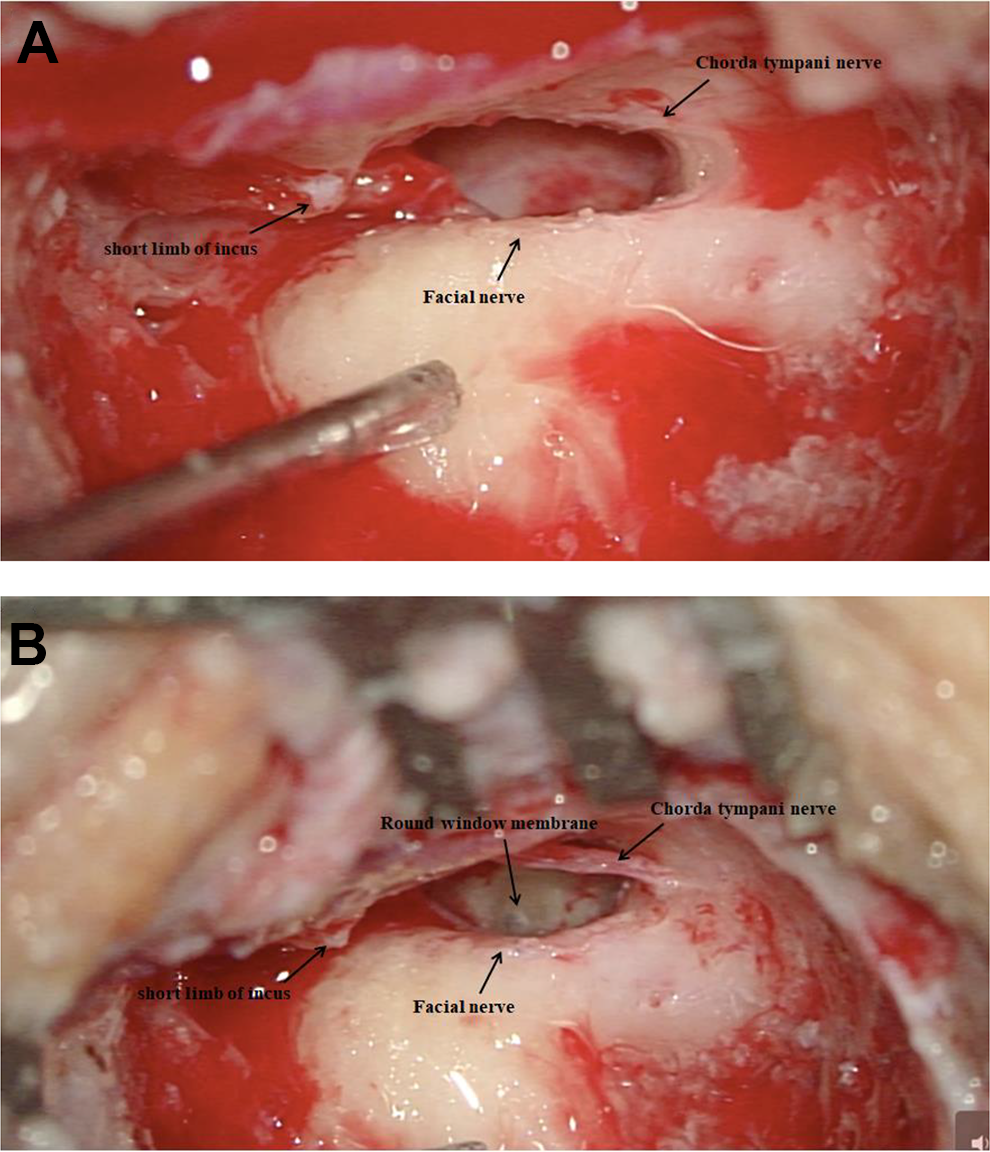
Facial nerve preposition variation (facial recess stenosis). A, Facial recess stenosis was found during the opening of the facial recess, round window niche was invisible. B, Dissection of chorda tympani nerve completely, moving the chorda tympani nerve forward, enlarged facial recess, exposure of round window membrane.
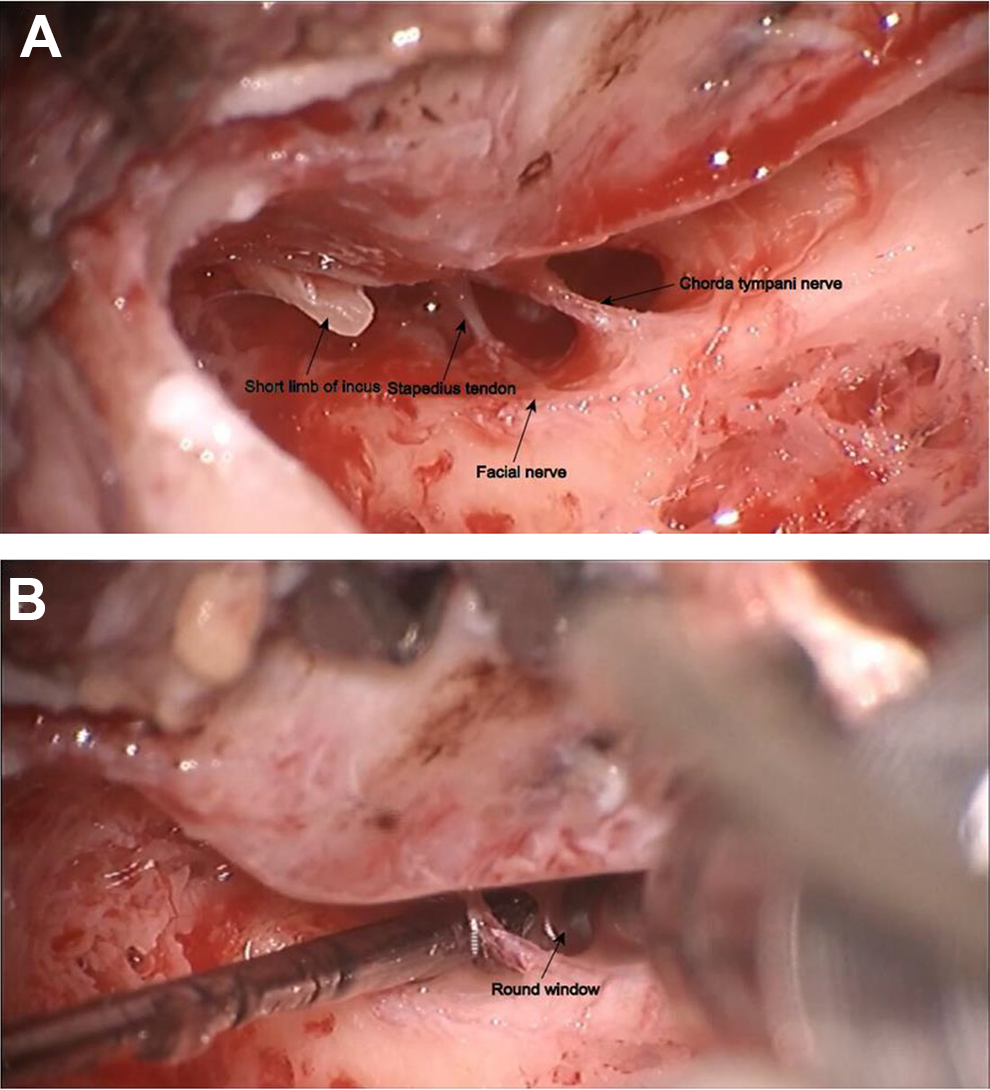
Chorda tympani nerve variation which lies transverse above half of the facial recess. A, Dissection of chorda tympani nerve completely. B, Continue to enlarge the facial recess on both sides of the chorda tympani nerve, exposure of round window.
Discussion
The classic pathway to expose round window niche in the surgery of cochlear implantation is opening the facial recess. 2 The key step of operation is to expose the round window niche and pyramidal eminence in posterior tympanum after opening the facial recess. The premise of ensuring the safety of operation is to fully understand and master the anatomical structure of the inner ear, especially the anatomy of facial nerve and chorda tympani nerve. Facial recess is the lateral part of posterior tympanum, inside of which is the vertical segment of facial nerve. The lateral part of facial recess is just the deep part of the external auditory canal and chorda tympani nerve, and incudal fossa is above the facial recess. So there is a direct relationship between the size and shape of facial recess and the development of incus, facial nerve, and chorda tympani nerve. At present, the main method of cochlear implantation is still to implant electrodes through the posterior tympanum approach. Because of the narrow operation range and the anatomical variation in facial nerve and chorda tympanic nerve, it is easy to cause facial nerve and chorda tympanic nerve injury. With the continuous improvement in cochlear implant surgery technology, the incidence of facial nerve and tympanic cord nerve injury decreased year by year. Cohen et al reported that the incidence of facial nerve injury was 1.74% in 1988, 3 Hoffman and Cohen reported 0.73% in 1995, 4 and Fayad et al reported 0.71% in 2003. 5 Lloyd et al reported that the incidence of dysgeusia was 45%, 6 Alzhrani et al reported that the incidence of dysgeusia was 19.2%, 7 and Mikkelsen et al reported that the incidence of dysgeusia was 17%. 8 Nevertheless, facial nerve and tympanic cord nerve injury was still one of the most common complications of cochlear implantation. 9 Whether contoured facial nerve and chorda tympanic nerve are needed in surgery has been controversial, especially the chorda tympanic nerve, which is often not well protected, or even worn away and sacrificed. Therefore, how to avoid facial nerve and chorda tympani nerve injury is the key to the success of operation.
To avoid injuring the facial and chorda tympani nerve, some ear microsurgery doctors choose to keep a distance from them. These otologist often identify the general direction of the front wall of facial recess according to the direction of short crus of incus and open facial recess from the middle while keeping away from the facial nerve and chorda tympani nerve as far as possible. This approach appear to avoid nerve injury and relatively safe; however, the variation of facial nerve and chorda tympani nerve is not rare in clinical operation. It is precisely because of the blindness of the facial nerve and tympanic nerve, thus increasing the risk of facial nerve and tympanic nerve injury during the operation.
We have been carried out cochlear implantation since 2003. Based on the work in the 8 years since 2003, a safe and efficient procedure for cochlear implant surgery was summarized. The most important technique was how to open facial recess safely because the critical point of cochlear implantation was not only electrode insertion but also facial nerve and chorda tympani nerve protection. Therefore, we proposed the methods of opening facial recess after exposing the facial nerve and chorda tympani nerve actively and adequately during artificial cochlear implantation for patients accompanying with secretory otitis media in 2009. 10 After further exploration and accumulation, we confirmed that it also applied to general artificial cochlear implantation and began to use it routinely in all cochlear implantations subsequently. It was not only a surgical technique but also an operation concept that has been accepted and applied by part of the domestic ear surgeons.
The method of exposing facial nerve and chorda tympani nerve transparent actively and adequately can be realized on the base of solid skills of otomicrosurgery. The main advantages are: (1) Exposing facial nerve and chorda tympani nerve actively ensures the safety of operation while protects the facial nerve and chorda tympani nerve. (2) On account of this method, we can open facial recess boldly and adequately, even if the patient’s facial recess is very narrow or had nerve variation. We find a considerable number of patients with narrow facial recess and high facial nerve from temporal bone lamellar CT preoperatively; some of their facial recess was only about 2 mm. Some scholars point out that taste abnormalities caused by chorda tympani nerve injury is temporary in most cases of narrow facial recess, so they think chorda tympani nerve can be sacrificed if necessary. 11 However, there are still a portion of patients who have taste abnormalities and dry mouth symptom after surgery irreversibly. 12 On the other hand, based on the concept of binaural artificial cochlear implantation, there is a possibility of bilateral chorda tympani nerve injury during the contralateral cochlear implantation in the future. 13 Hence, we advocate that the chorda tympani nerve should be preserved as far as possible during operation in order to avoid irreversible taste abnormalities and dry mouth symptom as a result of bilateral chorda tympani nerve injury. All the chorda tympani nerve are integrally reserved for our patients, including one patient with chorda tympani nerve anatomical variation. (3) There is no necessary to use facial nerve monitor during surgery, which can save the cost of health care. Some scholars point out that monitoring facial nerve during surgery can reduce facial nerve injury. 14 But we don’t think it is necessary for facial nerve monitor. (4) Exposing facial nerve and chorda tympani nerve actively can improve operation efficiency, as the included angle of the 2 nerves will be gradually revealed at the same time of exposing nerves actively. There’s no need to take the nerves into account and repeated the actions again. In consequence, exposing nerves actively could save the operation time. After a certain accumulation, we can control our average operation time in 60 minutes, minimum of 40 minutes, no matter how complicated the cases are. The time of surgery is calculated from incision to suture. (5) Promoting and assist residency to be standardized train learning and recognizing the structure of the ear microsurgery anatomy knowledge. After exposing the facial nerve and chorda tympani nerve actively and adequately during surgery, we can see the structure of facial recess sufficiently. The structures like the tympanic segment, pyramid segment, mastoid segment of facial nerve, incudal fossa, pyramidal eminence, stapes tendons, anterior and posterior foot plate of stapes, incudomalleolar joint, and other microstructure can be clearly exposed after adjusting the microscope. (6) As we all know, if dysgeusia was caused by unilateral chorda tympanic nerve injury after unilateral cochlear implant, contralateral chorda tympanic might compensate taste function several months later. However, with the popularization of bilateral cochlear implants, 15 preserving the integrity of the chorda tympanic nerve is even more important. Our approach is active and adequate exposure of the chorda tympanic nerve under direct vision, which can avoid the blindness of nerve injury, whether or not there are facial nerve and chorda tympanic nerve variation. It seem dangerous, but much safer.
However, this method also had some limitations, which were the requirement of a wealth of surgical experience and a good command of the anatomic structure, especially potential anatomic variation. The study was a retrospective analysis; more quality prospective studies were needed to validate our findings.
In summary, we expose facial nerve and chorda tympani nerve actively and adequately, which could decrease the incidence of facial paralysis, taste abnormalities, and other complications; facial nerve monitoring is not necessary, which also can improve the safety of the cochlear implantation and save operation time.
Footnotes
Authors’ Note
Ling Lu and Maohua Wang are co-first authors.
Acknowledgments
The authors gratefully thank to the support of China Disabled Persons’ Federation and Jiangsu Disabled Persons’ Federation and the government support children with congenital deafness who are the vast majority of our patients to receive cochlear implantation for free every year.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from Jiangsu Provincial Medical Youth Talent of the Project of Invigorating Health Care through Science, Technology and Education (QNRC2016002), National Natural Science Foundation for Young Scientists of China (No.81700913), The Project of Invigorating Health Care Through Science Technology and Education (ZDXKB2016015), National Natural Science Foundation of China (No.81771019) and Sixth talent peaks project in Jiangsu Province(YY-073).