
Abstract
Objectives
This study aimed to investigate the clinical manifestations, treatment, and prognosis of traumatic pneumolabyrinth caused by tympanic membrane (TM) perforation.
Methods
Clinical data were collected from 3 cases of traumatic pneumolabyrinth occurring between 2015 and 2021 and 22 cases were identified from 20 articles in PubMed database that reported pneumolabyrinth due to tympanum-penetrating injury.
Intervention
Nonoperative treatment was performed in Cases 1 and 3. Middle ear inspection was performed 1 year after the injury due to worsening vertigo upon head movement in Case 2.
Main outcome measures
Hearing outcomes and vestibular evaluations were presented for the 3 cases, and all comparable cases in the literature were reviewed.
Results
All 25 patients had a history of traumatic TM perforation, with perforations mostly located in the posterior or posterior superior quadrant (16 cases). Air signs were observed in the vestibule in all 25 patients, 15 of whom revealed stapes luxation into the vestibule. Conservative treatments were performed in 8 cases, and exploratory surgery in 17 cases. Most patients were free of vertigo (23/25). There were no significant hearing improvements in 15 cases, while hearing recovery or improvement was observed in 9 cases.
Conclusions
The clinical manifestations of pneumolabyrinth due to tympanum-penetrating injuries vary widely. Importantly, the degree of hearing loss is not directly related to the subjectively perceived vertigo but to the location and extent of pneumolabyrinth.
Introduction
Pneumolabyrinth is a condition characterized by air bubbles inside the vestibular labyrinth and/or cochlea, and was first described by Mafee et al in 1984. After tympanum-penetrating injury, dislocation of the vestibular joint of the stapes footplate leads to air entering the vestibular labyrinth, and bubbles form in part of the lymph space of the labyrinthus.1,2 Traumatic pneumolabyrinth is rarely seen in the clinical practice and is often misdiagnosed.
A high-resolution computed tomography (HRCT) scan of the temporal bone may be the most precise diagnostic method for the localization of air bubble(s) in the inner ear.3-5 Temporal bone fractures and iatrogenic causes have been reported as possible etiologic agents. Fracture/dislocation of the stapes with the consequent creation of pneumolabyrinth, however, is rarely observed after tympanum-penetrating injury.
In this study, the clinical data of 3 patients from our practice were analyzed along with 22 patients from 20 articles describing pneumolabyrinth caused by penetrating trauma to comprehensively analyze the clinical presentation, extension of inner ear involvement, management, prognosis, and possible etiopathogenesis of transcanal traumatic pneumolabyrinth.
Materials and methods
Patients
Two patients were admitted to the Eye, Ear, Nose, and Throat Hospital affiliated with Fudan University from January 2015 to May 2020; an additional patient was diagnosed with traumatic pneumolabyrinth at the Shigatse People’s Hospital in Tibet in 2018 (Figure 1). Twenty-two other cases from 20 articles in the PubMed database reported pneumolabyrinth due to tympanum-penetrating injury.6-24 Timeline of disease process, clinical manifestations, prognosis, and treatment strategy in 3 cases.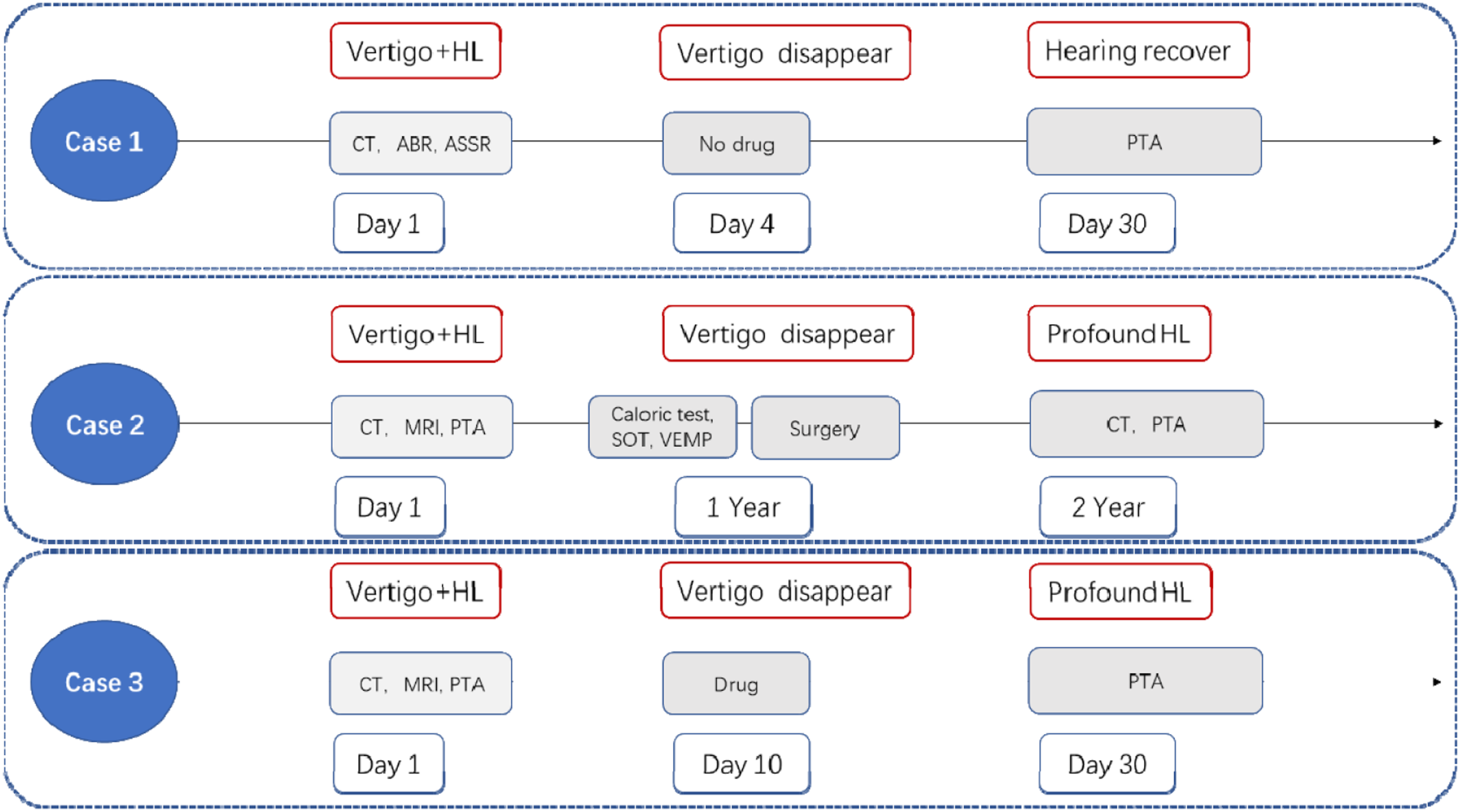
A 4-year-old child presented with ear bleeding and vertigo accompanied by slight hearing loss after an ear pick pierced the right tympanic membrane (TM) when he moved his head. Perforation was found posterosuperior on the TM. Nonoperative management (avoiding strenuous exercise and drying the external auditory canal) was performed, and the vertigo subsided after 4 days of intermittent symptoms.
A 44-year-old man was struck by an ear pick, which penetrated deep into the left ear canal. The patient presented with intermittent vertigo, accompanied by mixed hearing loss. The patient refused to undergo surgical exploration; however, the symptoms of vertigo worsened despite conservative management (including betahistine, glucocorticoids, and avoidance of pressure). One year after the injury, an exploratory tympanotomy was performed to relieve the vertigo (Figure 2). Postoperatively, the vertigo subsided, but the unilateral sensorineural hearing loss remained profound.
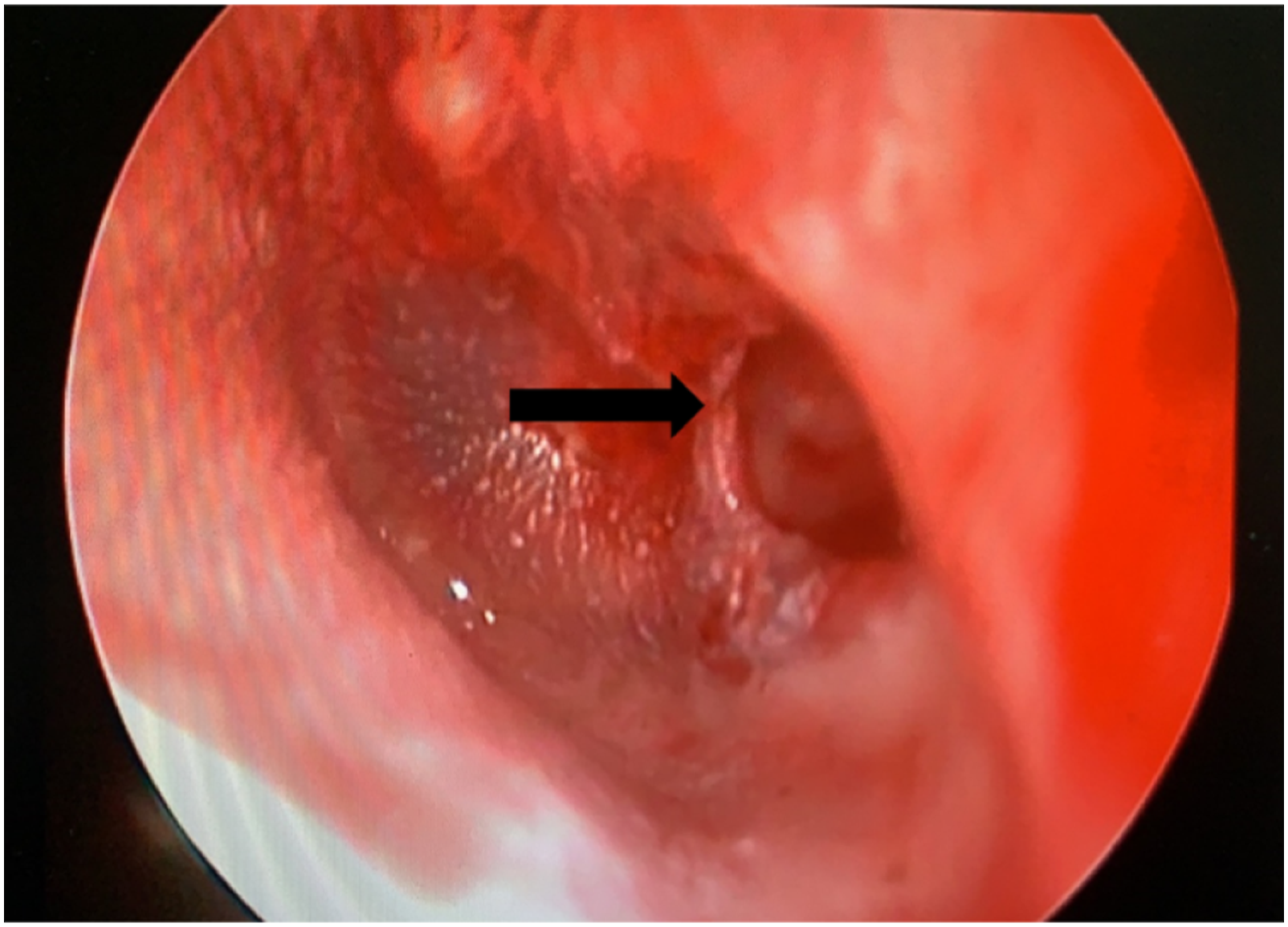
Image of otoscope in Case 2 (left ear). Arrow shows the perforation of the eardrum.
A 42-year-old woman developed persistent dizziness, hearing loss, tinnitus, headache, and earache after a knitting needle pierced her right TM when struck by her child. Conservative management (methylprednisolone and methylcobalamin) was initiated. Vertigo subsided 10 days after drug administration, but sensorineural hearing loss persisted. Otoscopy, audiological examinations, and imaging evaluations were performed in all 3 patients, as described below. The 2 adults were tested using pure tone audiometry (PTA), while the child underwent auditory brainstem response (ABR) and auditory steady-state response (ASSR) examinations. All 3 patients underwent temporal bone HRCT scans, and 1 underwent magnetic resonance imaging (MRI) and vestibular function examination. A temporal bone HRCT scan was performed in 1 patient 1 year after surgery.
Treatment Strategies
Different treatment strategies were adopted for the 3 patients according to their clinical manifestations. A timeline is shown in Figure 1. Nonoperative treatment was performed in Cases 1 and 3. Case 3 was treated conservatively with methylprednisolone and methylcobalamin due to the extreme severity of hearing loss and vertigo.
In Case 2, the patient refused surgery firstly. Clinical effectiveness and complications were closely observed during the follow-up period. However, the patient developed further hearing loss and worsening vertigo upon head movement a few months later. Tympanotomy was subsequently performed 1 year after the injury, revealing luxation of the stapes footplate and an inward dislocation of the vestibule. The stapes was removed, and the vestibular window was sealed with temporalis fascia (Figure 3). (A) The stapes entered the oval window; (B) stuffing vestibular chamber using fascia.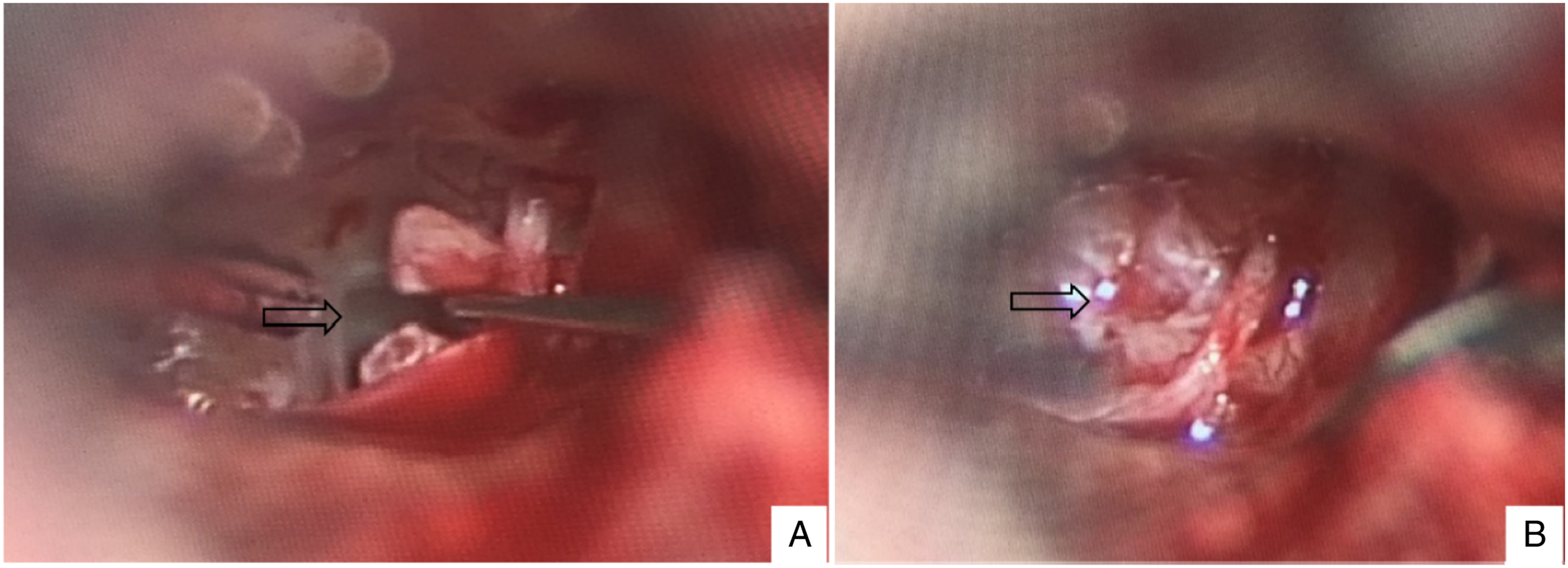
Cases From the Literature
Clinical Characters of 25 Cases with Pneumolabyrinth after Tympanum-Penetrating Injury.
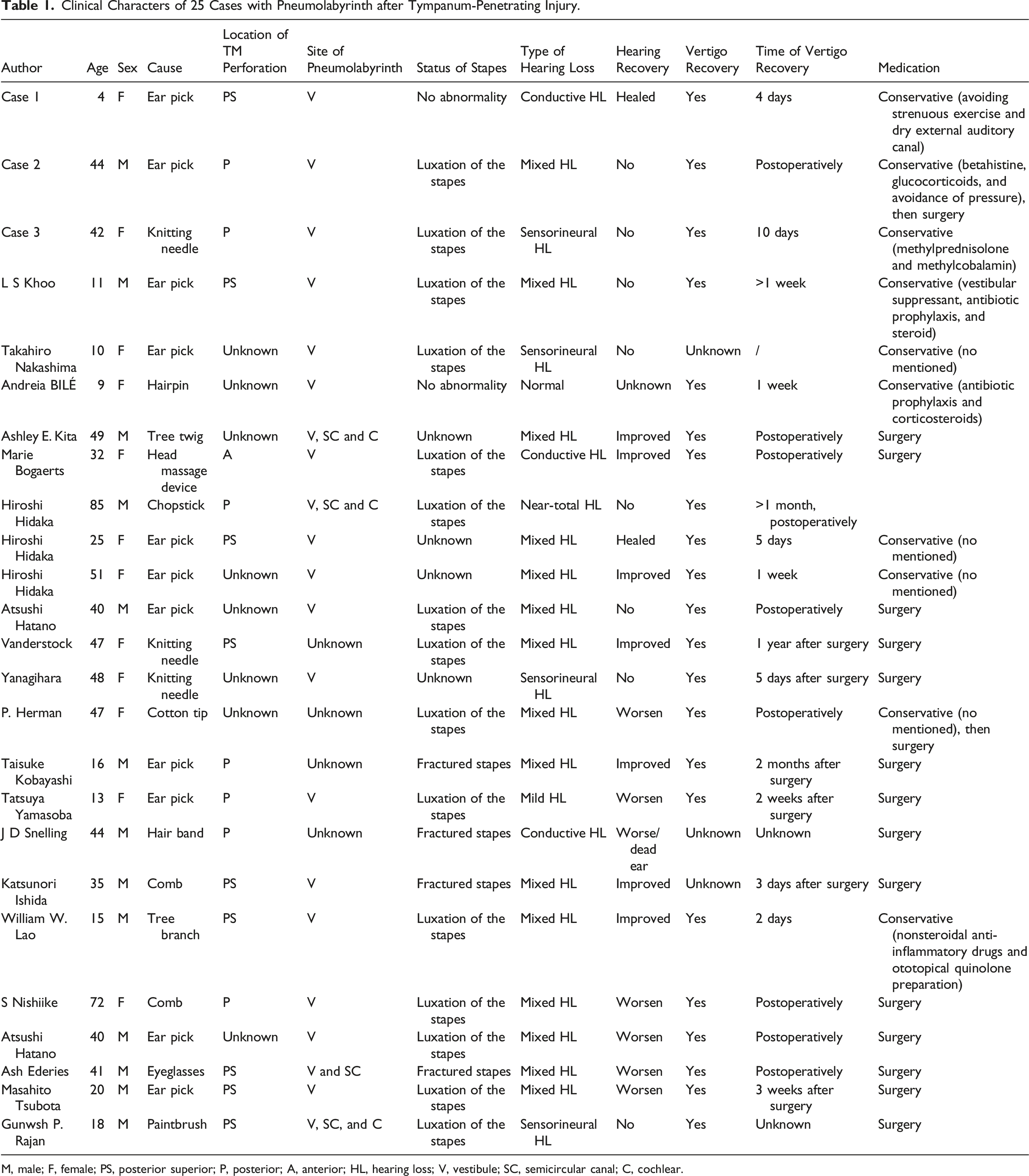
M, male; F, female; PS, posterior superior; P, posterior; A, anterior; HL, hearing loss; V, vestibule; SC, semicircular canal; C, cochlear.
Results
Characteristics of Medical History
Of the 25 patients, 13 were female and 12 were male, aged 4–85 (average 34.32) years. All patients had a history of traumatic TM perforation, with the perforations located mostly in the posterior or posterosuperior quadrant (16 cases) (Figure 2 and Table 1).
In Case 1, the perforated eardrum healed and hearing returned to normal 1 month after the injury. The patient was treated conservatively, and no drugs were administered. The vertigo in Case 2 subsided, but unilateral sensorineural hearing loss persisted postoperatively. In Case 3, vertigo subsided after 10 days of drug administration, while sensorineural hearing loss persisted.
In another 22 patients from the literature, 14 underwent surgery and 8 underwent conservative pharmacotherapy; 2 were initially treated conservatively before undergoing subsequent surgery to relieve the vertigo.
Audiometric Investigation
All 3 patients from our clinic underwent audiological examinations. The ASSR and ABR were examined in Case 1, while the other 2 underwent PTA. Case 1 had conductive hearing loss, Case 2 had mixed hearing loss, and Case 3 had profound sensorineural hearing loss (Figure 4). The hearing threshold (ASSR, bone conduction, 500–1000–2000–4000 Hz) was 10–20–25–20 dB on the left side, and 15–35–25–20 on the right side in Case 1; the ASSR threshold (air conduction, 250–500–1000–4000 Hz) was 15–15–25–25–20 dB on the left side, and 45–30–35–30–25–25 dB on the right, and the ABR threshold (air conduction) was 25 dB on the left and 45 dB on the right. Hearing in Case 1 returned to normal 1 month later without drug treatment. (A-B) Bone ASSR and air ASSR in the right ear in Case 1; (C) PTA in the left ear in Case 2; (D) PTA in the right ear in Case 3. (ASSR, auditory steady-state response; PTA, pure tone audiogram).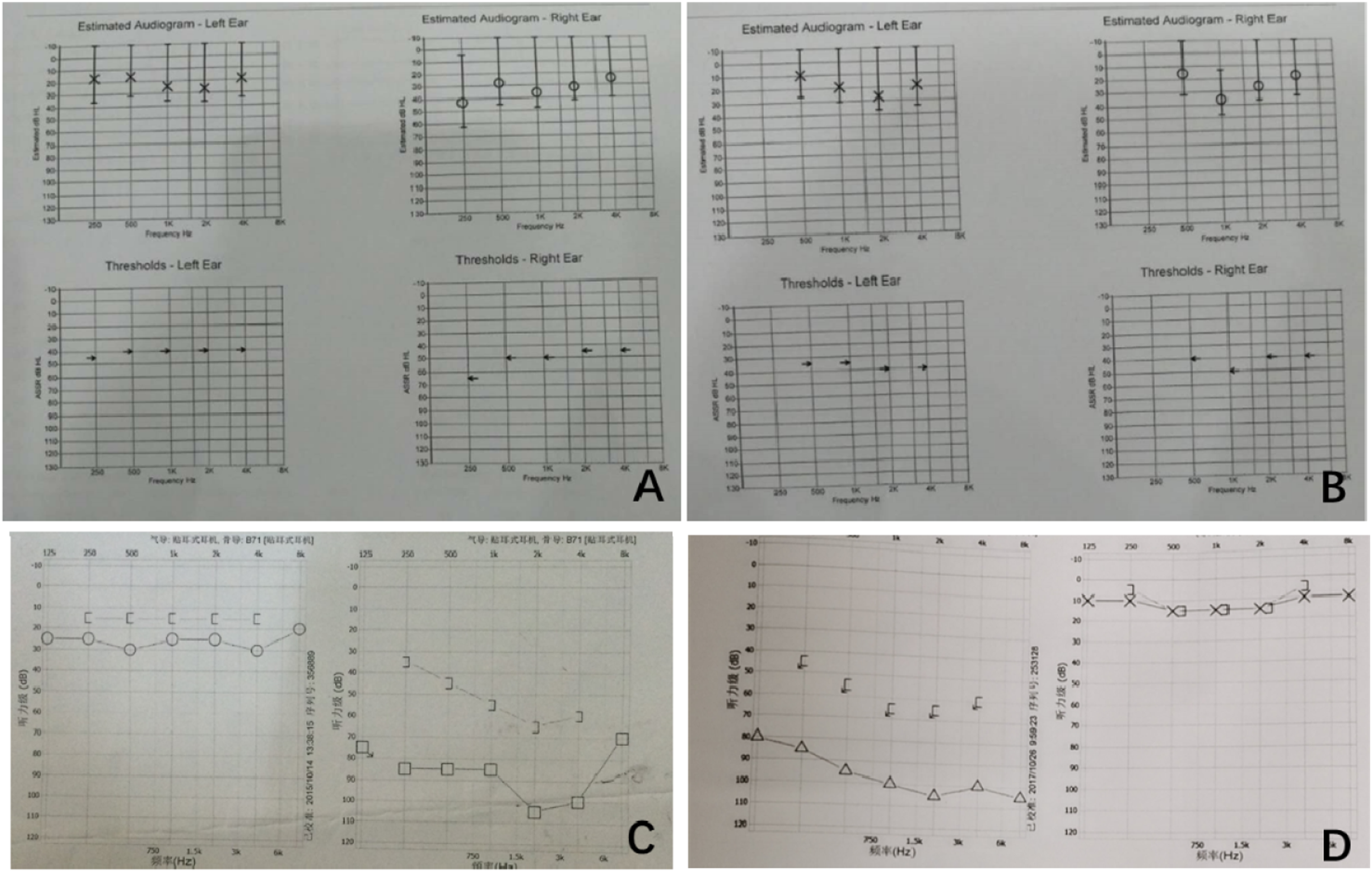
In Case 2, the average hearing threshold value of PTA (air conduction) was 21 dB on the right and 91 dB on the left; the average bone conduction PTA threshold was 15 dB on the right and 55 dB on the left side. Case 2 showed no significant hearing improvement in left ear postoperatively.
In Case 3, the average hearing threshold value of PTA (air conduction) was 100 dB on the right and 15 dB on the left, while the average bone conduction PTA threshold was over the limit on the right and 15 dB on the left. Case 3 also showed no improvement in right-sided hearing loss with drug treatment.
In the literature review, 2 cases had conductive hearing loss, 4 had sensorineural hearing loss, and 14 had mixed hearing loss. Nine patients exhibited improvement in hearing recovery, 5 of whom underwent surgery. Moreover, 13 other patients experienced either no relief, or even worsening in hearing loss postoperatively.
Vestibular Functions Evaluation
In our 3 cases, 1 patient underwent vestibular function examination 1 year after injury (Figure 5). As expected, the caloric and sensory organization tests (SOT) revealed abnormal responses in this case. Similarly, no responses were observed in the ocular vestibular-evoked myogenic potential (oVEMP) test or cervical VEMP (cVEMP) test in the damaged ear. Unfortunately, we failed to record the results of vestibular function tests for Case 2 when the injury started. (A-D) The vestibular function at 1 year after injury in Case 2, including the caloric test (A), sensory organization test (SOT) (B), cVEMP (C), and oVEMP (D) test.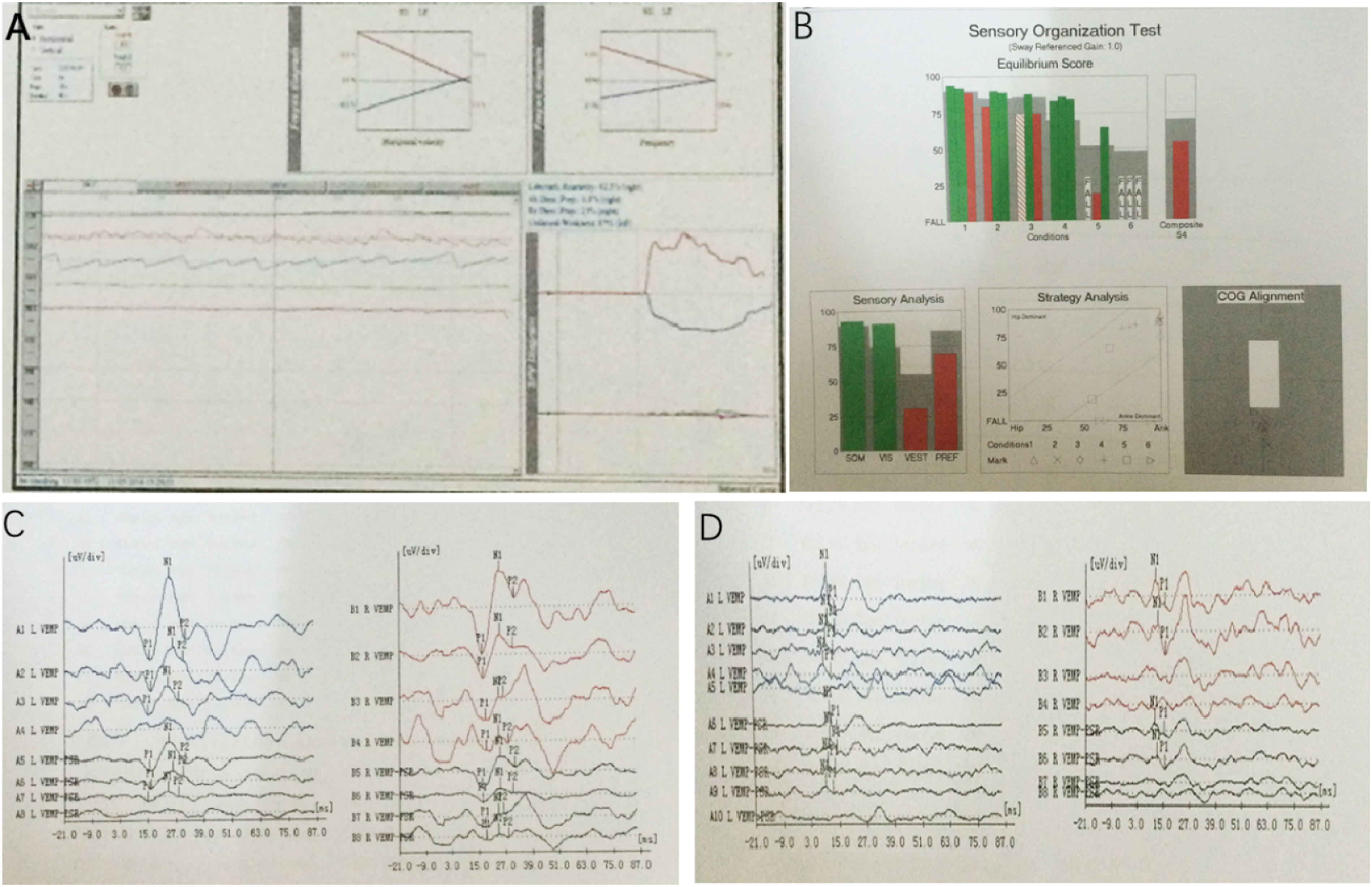
In the other 22 cases reported in the literature, vestibular function was slightly decreased in 1 case using the caloric test, while no other patient underwent vestibular function examinations (SOT, oVEMP, cVEMP, etc.).
Imaging Features
In all 25 cases, air bubbles were detected in the vestibule using HRCT of the temporal bone; 3 had air bubbles in both vestibule and cochlea and 4 had air bubbles in the vestibular, cochlea, and semicircular canals as well.
There were no obvious shifts of the ossicular chain or dislocation of the stapes and footplate in Cases 1 and 3 (Figures 6A and 6C). In Case 2, both preoperative and postoperative HRCT indicated that there was an air bubble in the vestibular labyrinth, and the volume had significantly reduced after surgery (Figure 6B). Due to dislocation of the incudostapedial joint and stapes falling into the vestibular cavity in Case 2, contrast-enhanced MRI was performed; results suggested endolumphatic hydrops in the left cochlea. Importantly, labyrinthitis ossificans was ruled out on HRCT after the surgery. In the other 22 cases, all cases had air bubbles in the vestibular, 4 cases had air bubbles in the semicircular canal, and 3 cases had air bubbles in the cochlea at the same time. (A) There was air sign in the vestibule using temporal bone high-resolution CT scan in the right ear in Case 1. (B) There was air sign in the vestibule using temporal bone high-resolution CT scan in the left ear in Case 2 before surgery (B1) and after surgery (B2); B3, MRI in the left cochlea in Case 2. (C) There was air sign in the vestibule using temporal bone high-resolution CT scan in the right ear in Case 3. Arrows revealing air bubbles.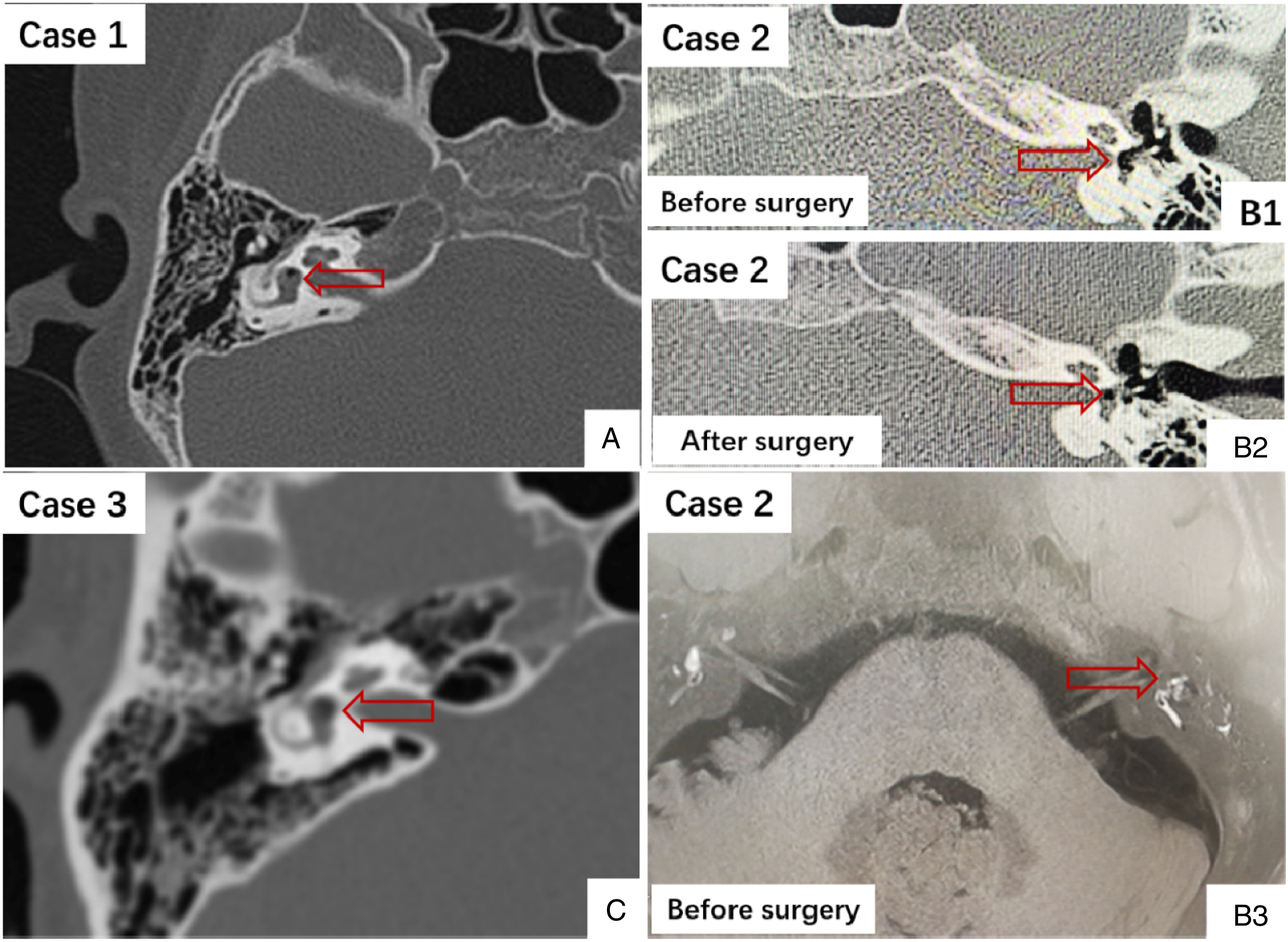
Clinical Prognoses
After conservative or surgical treatment, TM perforations healed and vertigo disappeared in all 3 patients (4 days, more than 1 year, and 10 days after tympanic trauma, respectively), but the prognoses of hearing loss were quite different. Hearing returned to normal in Case 1, deteriorated after surgery to total deafness in Case 2, and there was profound sensorineural deafness in Case 3.
In the other 22 cases, 8 cases fully recovered or improved hearing; vertigo disappeared in 20 cases.
Discussion
Diversity of Hearing Performance, Severity, and Recovery are Related to the Location and Scope of the Air Labyrinth
Although there are some case reports of pneumolabyrinth after a temporal bone fracture, it is a very rare condition secondary to traumatic perforation of the TM. One of the main clinical manifestations is varying degrees of hearing loss or complete deafness.23,25,26 Nishio proposed the hypothesis that air bubbles of perilymphatic fistulas could enter the perilymphatic space, which might cause acute, reversible, and profound sensory hearing loss. 27 Some reports indicated that hearing may return to the initial level if the bubbles in the labyrinth can be absorbed within a short time;28,29 this hypothesis could explain the recovery of pneumolabyrinth-related hearing loss due to traumatic tympanum-penetrating injury to some extent.
In this study, 22 patients reported diverse types of hearing function, including conductive hearing loss, mixed hearing loss, and profound sensory hearing loss. No obvious stapes displacement was observed in our 2 patients, and it was speculated that pneumolabyrinth might have been caused by the impact force and cracks around the stapedial footplate; consequently, air entered the oval window via the cracks between the stapedial footplate and vestibule, and no dislocation of the ossicular chain was found. Hearing loss level is likely not positively correlated with stapes displacement, indicating that attention should be paid to both medical history and imaging characteristics in clinical practice.
Kobayashi et al demonstrated that the severity of hearing loss is related to the location where air enters lymphatic fistulas. In their study, the air in the scala vestibuli induced severe and irreversible hearing loss, while air perfusion in the scala tympani gave rise to relatively mild, at least partially reversible, decreased cochlear potentials. 30 In the 25 cases examined here, 4 had air bubbles not only in the vestibular and semicircular canals but also in the cochlea; all had severe hearing loss. Of these 4 cases, 3 had poor hearing recovery, and only 1 had hearing improvement. This finding suggested that the degree of hearing loss was related to the scope of the air labyrinth; in these patients, the scope of the air labyrinth was large, the hearing damage was serious, and hearing recovery was poor.
Stapes Footplate Prying after Tympanum-Penetrating Injury May Induce Vertigo
Clinical data show that pneumolabyrinth often causes severe rotational vertigo accompanied by nausea, vomiting, and other vestibular symptoms. 31 Vertigo might be aggravated by breath-holding, nose-blowing, or head movement, which is associated with the compression of the utricle and saccule caused by air in the vestibule. The clinical manifestations and imaging features in Case 2 indicated air bubbles inside the vestibular labyrinth before surgery as well as after when the vertigo disappeared due to the sealed vestibular system. This suggests that vertigo is related to the movement of air bubbles in the vestibular cavity, and that simply the presence of air trapped in the vestibule may not be the cause.
In 2 patients (Case 2 in our manuscript and 1 case by P. Herman et al), vertigo did not disappear until exploratory tympanotomy or labyrinthectomy was performed through a posterior translabyrinthine approach. 15 Only one case reported no vertigo recovery because the patient refused to undergo surgery. 7 From the above results, the remedy of stapes intrusion into the vestibule may contribute to the recovery from vertigo. Moreover, early surgery could prevent further hearing loss in patients with persistent vertigo.
No Direct Correlation Exists Between Vertigo and Hearing Loss Level
The 25 patients in this study had varying degrees of vertigo, and presented with different levels of hearing loss. Clinical information, especially from the literature review, indicated no direct correlation between the severity of vertigo (including the duration and prognosis of vertigo) and hearing loss (including the type and severity of hearing loss). Kobayashi et al established animal models and found that Reissner’s membrane collapsed in 12 of 17 cochleae, indicating a possible pathological mechanism for hearing loss caused by pneumolabyrinth. 30 According to etiological analysis, the bubbles in the labyrinth suggested the existence of a lymphatic fistula, and the pathological communication between the middle ear and the inner ear led to vertigo. However, hearing loss is more directly related to cochlear injury or hair cell loss and not to pressure differences.
Surgical Exploration Should be Recommended if there is Persistent Vertigo or Recurrent Vertigo
No significant correlation was found between the extent of the pneumolabyrinth and hearing loss. Surgical treatment had no obvious advantage over conservative treatment in terms of hearing improvement (4/7 vs 5/17). Patients with rapid relief from vertigo within a few days or without significant hearing loss can therefore be treated conservatively. However, early surgical treatment may prevent permanent hearing loss in patients with persistent or recurrent vertigo as was seen in 3 cases in this study.7,15
Vertigo may not be restored or compensated if there is persistent pathological communication between the vestibule and middle ear, and explorative tympanotomy should be recommended to close the existing external lymphatic fistula. Further, vestibular symptoms would be improved or completely abated within a closed vestibule via a compensatory mechanism, regardless of dizziness at the onset.
From the natural history and clinical course in Case 2, it was the pathological communication between the middle ear and the inner ear, but not the air bubbles in the labyrinth, was the etiology of vertigo. Furthermore, semicircular canals, but not the utricle/saccule, played an important role in vertigo attacks from vestibular function examination in this case. Hiroshi et al found that vestibular symptoms would disappear in almost all cases (40/42) using systematic regression and suggested that it was presumably induced by vestibular compensation or rehabilitation. 11 This was consistent with the results found here; after conservative treatment or surgical treatment, the 25 cases mostly all recovered from vertigo (88%, 22/25).
Stapes Protrusion into the Vestibule Indicates Poor Hearing Prognosis, and Stapes Extraction has No Significant Effect on Hearing Improvement
The prognosis of hearing loss is worse than that of the vestibular symptoms. A review by Tsubota et al proposed 3 predictive factors for postoperative hearing improvement in the pneumolabyrinth: the bone conduction hearing level at the onset, interval until surgery after injury, and existence of a stapes lesion. 32 In addition to these 3 factors, Hiroshi found that the location of air accumulation in the inner ear may be related to hearing recovery. 11 One patient presented with conductive hearing loss without a dislocated ossicular chain and complete hearing recovery, which agreed with Tsubota’s predictive factor. From the results of this study, protrusion of the stapes into the vestibule indicates a poor hearing prognosis, and stapes extraction has no significant effect on hearing improvement.
Nishioka established an animal model to elucidate the pathophysiological mechanism of hearing impairment and its prognosis examining ectolymphatic fistula leading to sudden hearing loss. 27 He also observed that it was not damage to the round window membrane but pressure damage that caused electrophysiological changes, which was followed by sensorineural hearing loss. 27 Therefore, further studies are required to identify the pathophysiological mechanism of sensorineural hearing loss in pneumolabyrinth, similar to membranous labyrinth rupture.
Conclusion
It is important to remain vigilant of patients with ear trauma followed by sudden hearing loss, especially those with vertigo. These signals suggest that clinicians should probe more deeply into possible changes in the cochlear labyrinth and potential cases of pneumolabyrinth. In terms of prognosis, vestibular function can be restored or compensated for, but the prognosis of hearing loss is poor. Moreover, hearing results are not directly related to the severity of vertigo symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Excellent Doctors-Excellent Clinical Researchers Program (Nos. SYB202008); domestic science and technology cooperation project (18695840700); the National Natural Science Foundation of Tibet (XZ2017ZR-ZYZ17).