
Abstract
Mucoceles of the paranasal sinus are epithelial-lined cystic structures filled with mucus and have multiple etiologies, including recurrent inflammation, trauma, or intrinsic disease. Particularly, a postoperative maxillary mucocele (POMM) is a delayed complication of radical surgery of the maxillary sinus, and most cases occur after Caldwell-Luc operations. Patients mainly complain of facial swelling, toothache, and tenderness. POMM has rarely been reported from other causes; however, there have been no reports on the occurrence of POMM following orbital wall reconstruction. Herein, we report a case of a patient with a POMM that developed 20 years after the aforementioned surgery. The patient complained of facial pain with visual disturbance, and underwent marsupialization using a combination of sublabial and endoscopic approaches, and the symptoms improved without recurrence.
Introduction
Paranasal sinus mucoceles are a relatively common type of cystic tumor; although their etiology remains unclear, they are largely divided into primary mucoceles and secondary mucoceles secondary to a history of surgery, trauma, sinusitis, or nasal polyps. The frontal sinus and ethmoid sinus are the most common sites of occurrence, comprising 60% and 30% of cases, respectively. A cohort study of 118 cases reported that <1% of mucoceles are in the maxillary sinus.1-3 In many cases, secondary mucoceles are caused by iatrogenic or accidental traumas. Particularly, postoperative maxillary mucocele (POMM), also called surgical ciliated cyst or paranasal cyst, has been known to occur after radical maxillary sinus surgery. In addition to radical maxillary sinus surgery, these mucoceles have been reported to occur after midface osteotomies, mid-facial fractures, LeFort I procedures, gunshot injuries, and sinus floor raising treatments.4-7
Several hypotheses have been proposed regarding the mechanisms underlying the development of POMM. One of these is that mucoceles occur due to the obstruction of the sinus ostia. As mucus is retained in the antrum, the cyst gradually expands, causing progressive remodeling of the surrounding bone. In addition, the formation of fibrous bands may cause the anterior and posterior walls to be separated, preventing the sinus drainage system from functioning normally. Occasionally, this may be caused by an unusual mechanism. In cases where maxillary mucoceles occur after LeFort I procedures, retention may occur due to tissue reactions to metal structures, including plates or wires used for fixation, and mucoceles may occur. 5
While there have been many reports of POMM, POMM after orbital wall reconstruction has been rarely reported. 8 Although a small number of orbital mucoceles have been reported after orbital wall reconstruction, the occurrence of maxillary mucoceles has rarely been reported. Herein, we report a case of a patient with edema in the right cheek area and upward deviation of the right eyeball that occurred 20 years after orbital rim reconstruction. These manifestations were diagnosed as POMM and successfully treated by surgery.
Case report
A 49-year-old male visited the otolaryngology department with a chief complaint of right-sided facial pain that had occurred 4 years prior. Additionally, the patient complained of a visual disturbance on the right side with a blurry appearance 8 months prior to his visit. Physical examination showed swelling in the right cheek and protruding soft tissue measuring approximately 1 × 1 cm under the right lateral canthus. Facial bone computed tomography (CT) showed a visible foreign body as a metal wire under the right eyeball and a suborbital well-defined cystic lesion involving the maxillary and orbital floor. The well-defined mass-like lesion pushed the maxillary sinus medially, bulged into the extraconal space, and partially compressed the eyeball. Adjacent bone erosion and remodeling without bone destruction were observed (Figure 1A and B). Contrast-enhanced paranasal sinus magnetic resonance imaging showed a hyperintense lesion in T1, which was not enhanced with gadolinium, and a heterogeneous lesion in T2. There was no sign of invasion into the orbit; however, the well-defined mass resulted in a slightly superiorly displaced eyeball (Figure 1C and D). Based on the imaging, the mass was suspected to be a delayed mucocele, and surgical drainage was planned. Preoperative vision and visual field examination by the eye department were normal. Preoperative images. Coronal (A) and axial (B) CT imaging shows a well-defined expansible mass involving the right maxilla and orbital floor. There was no bone destruction, but adjacent bony erosion and remodeling could be seen. Bulging into the right extraconal space was also observed. There were metallic foreign bodies (possibly metallic wire) on the orbital floor and inside the cyst (arrow). Coronal (C) and axial (D) MR imaging showed a round bulging mass with T1 hyperintensity and no remarkable contrast enhancement. There was no invasion of the mass into the orbit in the coronal scan, but the right eyeball had slightly upward displacement (arrow) (C).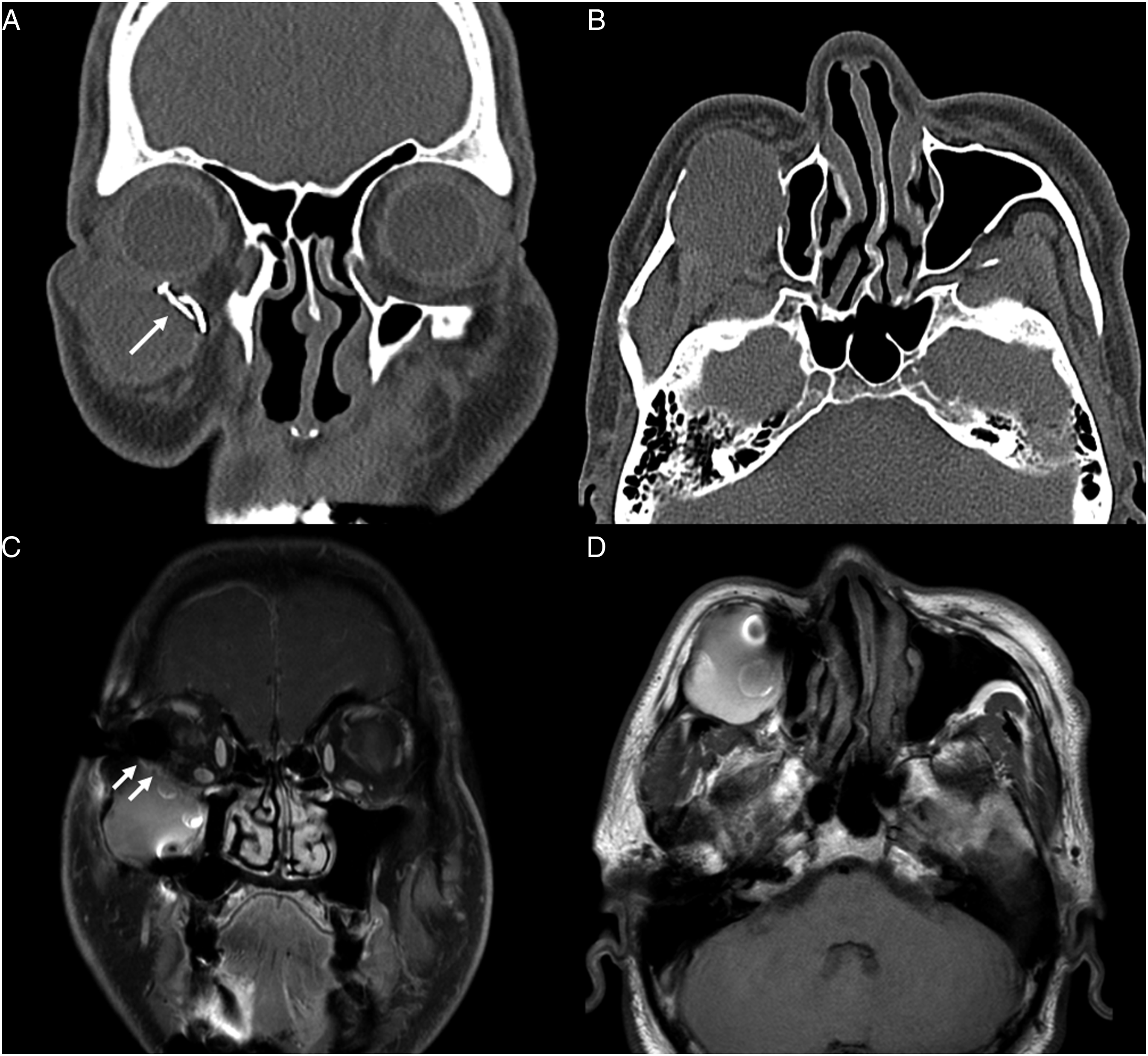
A few points should be noted about this case. First, the mucocele was located on the lateral side of the maxillary sinus. Second, we considered removal of the metal component observed in the imaging study; however, the stability of the orbital floor after mucocele removal was not certain. Due to these two reasons, we decided to use the Caldwell-Luc approach rather than the minimally invasive endoscopic approach. Marsupialization via the Caldwell-Luc approach was implemented. After exposing the gingivobuccal incision, we found that the infraorbital wall was intact. Subsequently, a thick brown-yellowish discharge was sucked out from the infected mucocele. A floating metal pin used during orbital wall reconstruction was found inside the cyst, and the floating metal pin was subsequently removed (Figure 2A). The metal wire fixed to the orbital floor was exposed and had adhered to the adjacent tissue; however, we did not remove the exposed metal wire to maintain orbital wall stability (Figure 2B). Subsequently, inferior meatus antrostomy (IMA) and middle meatus antrostomy (MMA) were performed using an endoscopic approach to communicate with the nasal cavity (Figure 2C). Intraoperative endoscopic photograph (A–C). The maxillary mucocele was approached through the maxillary anterior wall using the Caldwell-Luc approach. (A) The floating metal pin (white arrow) found in the cyst was removed. (B) Metal wire (white arrow) and screw (arrowhead) fixing the infraorbital implant exposed to cyst. (C) MMA (white arrow) and IMA (arrowhead) were performed using an endoscope to communicate the drained mucocele with the middle and inferior meatus. Postoperative CT image 6 months after operation (D). Coronal and axial scan showed a marsupialized maxillary mucocele. It can be seen that the metallic wire holding the orbital floor was not removed and there was no evidence of recurrence.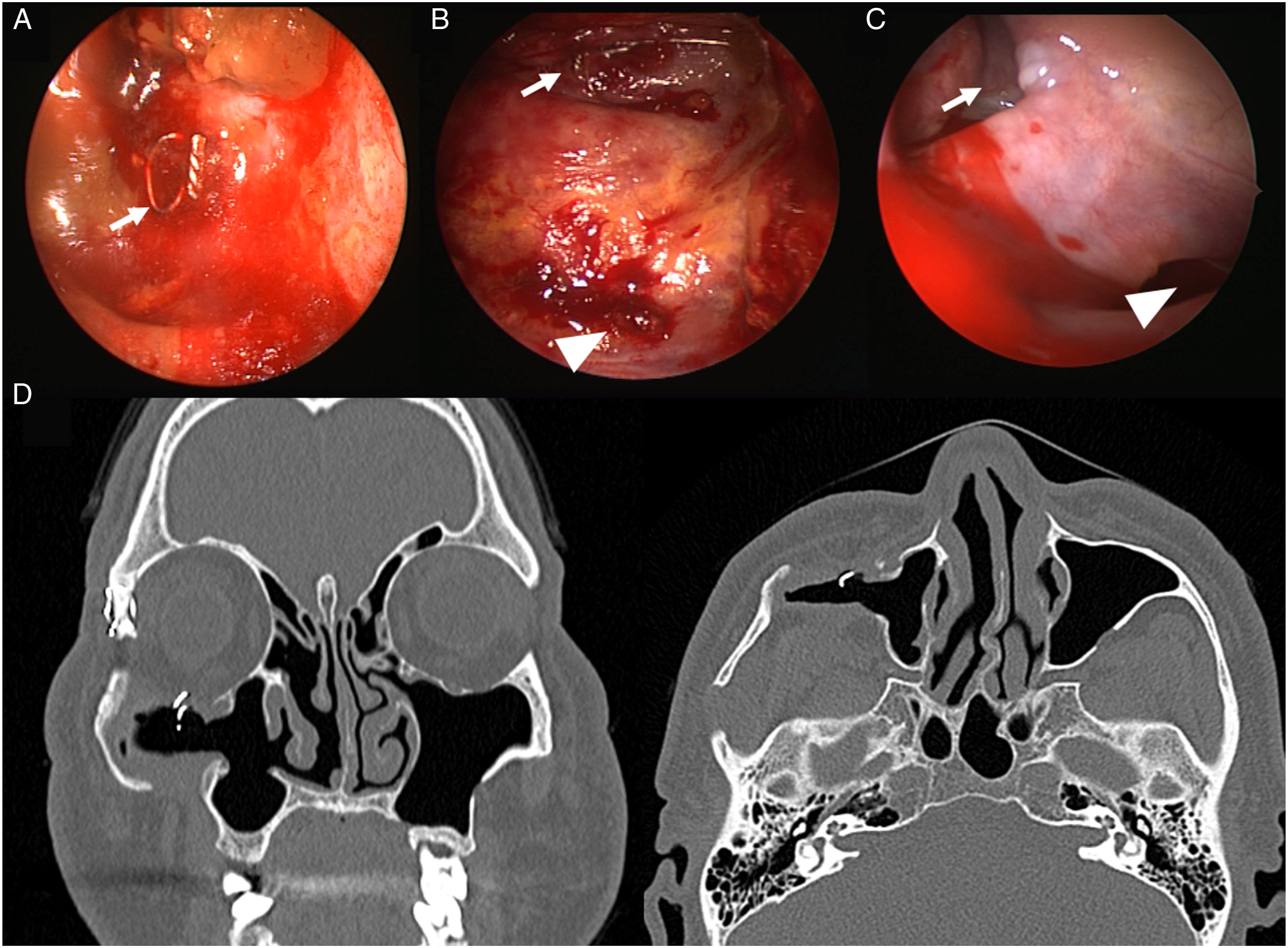
On the 2nd day postoperatively, the patient did not complain of any pain and was discharged with an elastic band to compress the empty cavity where the mucocele was previously located. At the outpatient clinic, the swelling of the right cheek had significantly decreased, and the upward deviation of the eyeball had returned to normal. Endoscopic examination showed maintenance of the inferior and middle meatal antrums. Follow-up paranasal sinus CT 6 months postoperatively showed no evidence of recurrence with favorable ventilation (Figure 2D).
Discussion
A POMM is a cyst that accumulates secretions and gradually increases in size. When the maxillary sinus wall is stimulated or bone destruction occurs, symptoms such as buccal swelling or discomfort may occur. Ocular symptoms, including a protruding eyeball, reduced visual acuity, diplopia, and strabismus, develop when the lesion invades the bottom of the eyeball. 9 It is not common for POMM to directly invade the orbit due to the maintenance of the membranous wall of the maxillary mucocele. POMM affecting orbital symptoms has been reported in 7% of cases, which is very low compared to the 90% probability of orbital invasion in the frontal, ethmoid, and sphenoid sinuses.1,10 In this case, upward deviation and visual field discomfort in the right eye improved after mucocele marsupialization.
POMM has been reported by several authors as a late complication following radical maxillary sinus surgery. Hasegawa et al. reported that 131 of 132 patients with maxillary sinus mucocele had a history of maxillary sinus radical surgery. 1 The most widely accepted explanation is that mucoceles may occur because of residual mucosa trapped in a wound. 11 The occurrence of a maxillary sinus mucocele for causes other than radical maxillary sinus surgery has been reported in the literature, with causes including midface osteotomies, mid-facial fractures, LeFort I procedures, gunshot injuries, and sinus floor raising treatments.4-7 The occurrence of a POMM is rare in patients with a history of orbital reduction surgery, as was found in our case. Mucocele development has been reported after orbital fracture repair in less than 10 cases. 8 Moreover, to the best of our knowledge, this is the first study to report the appearance of maxillary mucoceles after orbital fracture repair, which most often appear as orbital mucoceles in the orbit.
The patient in this case had fractures of the lateral rim and orbital floor as a result of trauma 20 years ago, which were surgically reconstructed and fixed with implant insertion and a metal wire. According to imaging studies and surgical field findings, part of the metal wire that should have been fixed was floating in the cyst, and the mucous membranes showed severe inflammatory changes. Mucocele usually occurs when the drainage of the maxillary sinus is obstructed. In past facial and orbital reconstruction operations, direct damage to the maxillary sinus mucosa may have occurred; however, a foreign body reaction caused by a metal wire was thought to be the reason behind the problem of the maxillary sinus. In orbital rim reconstruction, any type of implant placement can cause a chronic inflammatory response and epithelium transplantation during the manipulation process, which is often indicated to be the cause of mucocele formation. 12
There have been two reported cases of POMM due to a chronic tissue reaction of the metallic screw exposed to the maxillary sinus mucosa following LeFort I procedures.13,14 We believe that the implant sheet and metallic wire exposed inside the cyst in this patient also caused a similar inflammatory reaction. When fixing the metallic wire or implant sheet, damaged mucosal cells inserted into the bony edge may result in cystic degeneration. 6 Metallic wires and implants exposed to the inside of the cyst were partially removed in consideration of the stability of the orbital floor, and there was no evidence of recurrence during follow-up; however, if suspected, complete removal and orbital inferior wall reconstruction will be required.
There are two main treatment methods for POMM. One is the endoscopic intranasal approach for marsupialization through the MMA or IMA. However, if the POMM is located at the lateral or anterior position or bony wall of the inferior meatus is too thick, the Caldwell-Luc approach can be considered for management of POMM. 15 Moreover, in the case of mucoceles caused by malignant diseases or multiple septated cysts, surgery through an external approach is still recommended. In this case, we decided not to use the intranasal approach because the position of the mucocele was too lateral, and the middle meatus adhered due to previous surgery. Therefore, we marsupialized the mucocele using the Caldwell-Luc approach and performed IMA and MMA for endonasal drainage; there is no evidence of recurrence thus far.
In conclusion, we report on a patient who complained of cheek swelling and visual disturbance due to a delayed POMM following orbital fracture reconstruction 20 years prior. Marsupialization was successfully performed using a combination of the Caldwell-Luc approach and endoscopic approaches via the MMA and IMA. Orbital rim reconstruction is not considered a common cause of POMM; therefore, this study reported this along with a literature review.
Footnotes
Acknowledgments
The authors acknowledge the following financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a faculty research grant (No. 2022-52-0054) from Yonsei University Wonju College of Medicine granted to E.J.L. and the Basic Science Research Program through the National Research Foundation of Korea (NRF) grant funded by the Korea government (Ministry of Science and ICT) (NRF-2021R1A2C1010082, granted to E.J.L.).
Ethical approval
Ethical approval to report this case was obtained from ethics review committee of Wonju Severance Christian hospital (CR321352).
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.