
Abstract
Kaposi sarcoma (KS) is a rare vascular neoplasm that most commonly arises in the setting of immunosuppression, in areas with high prevalence of Human Herpesvirus-8 infection, and when both situations coexist. Most cases affect the skin, isolated involvement of the upper respiratory tract without skin involvement is extremely rare with only a few cases reported in the literature. We present a case of isolated nasopharyngeal KS in an immunocompetent patient who achieved remission after multimodality therapy. Recent advances in KS-therapy are discussed.
Introduction
First described by the Hungarian dermatologist Dr. Moritz Kaposi in 1872, Kaposi Sarcoma (KS) is a low-grade vascular sarcoma associated with human herpesvirus-8 (HHV8) infection. 1 KS affects immunocompromised individuals in the context of AIDS or iatrogenic immunosuppression, and in the form of endemic disease in regions with high prevalence of HHV8 infection. 2 KS typically affects the skin; however, extracutaneous and/or systemic involvement may occur in children and severely immunocompromised individuals. Isolated involvement of the upper respiratory system in immunocompetent patients is extremely rare, and information regarding biologic behavior and optimal treatment in this subset of patients is scarce.3-6 We report a case of an incidentally identified nasopharyngeal KS in an immunocompetent 41-year-old man and compiled similar cases from the literature.
Case presentation
A previously healthy 41-year-old man born and raised in Mongolia, who went to college in Turkey and then moved to the US, was referred for evaluation of a medium-sized, midline nasopharyngeal mass incidentally found during esophagogastroduodenoscopy for reflux symptoms (Figure 1A). On review of symptoms, the patient described nasal itching, congestion, ear ringing, and blood-tinged mucus. Magnetic resonance imaging (MRI) and computerized tomography (CT) scans showed a 2.6 cm, well circumscribed, lobular, avidly enhancing mass filling the nasopharynx (Figures 1B and 1C). The biopsy of the lesion showed intersecting bundles of relatively bland spindle cells separated by slit-like pseudovascular spaces containing lymphocytes and leukocytes. Hyaline intracellular globules were focally present (Figures 1D and 1E). Immunohistochemical stains showed that the lesion was positive for the vascular markers CD34 and ERG and for HHV8 confirming the diagnosis of KS (Figure 1, lower right). Testing for human immunodeficiency virus and hematologic evaluation for immunodeficiency were negative. The patient was treated with endoscopic resection followed by fractionated intensity-modulated radiation therapy (IMRT) with a total dose of 30 grays (Gy). A full dose was given to the nasopharynx, 19 Gy to the brain stem, 15 Gy to the spinal canal, 9–15 Gy to the left and right inner canals, respectively, and 7–10 Gy to the left and right parotid areas, respectively. The patient remains in remission, asymptomatic and without post-therapy complications after a follow-up period of 1 year. During this interval he has been followed regularly with MRI and a multidisciplinary head and neck team. Nasopharyngeal mass. Upper panel: Gross and radiologic images: (A). Endoscopy, (B). Axial MRI, (C). Sagittal CT scan. Lower panel: Histologic images: (D). At low power the mass consists of intersecting bundles of spindle cells. (H&E, 100X magnification) (E). At higher power, bland spindle cells with occasional intracellular hyaline globules (arrowheads) separated by slit-like vascular spaces containing red cells and scattered leukocytes are apparent. (H&E, 400X magnification). The nuclei of the tumor cells are uniformly positive for the vascular marker ERG and human herpesvirus 8 immunostains. (200X magnification).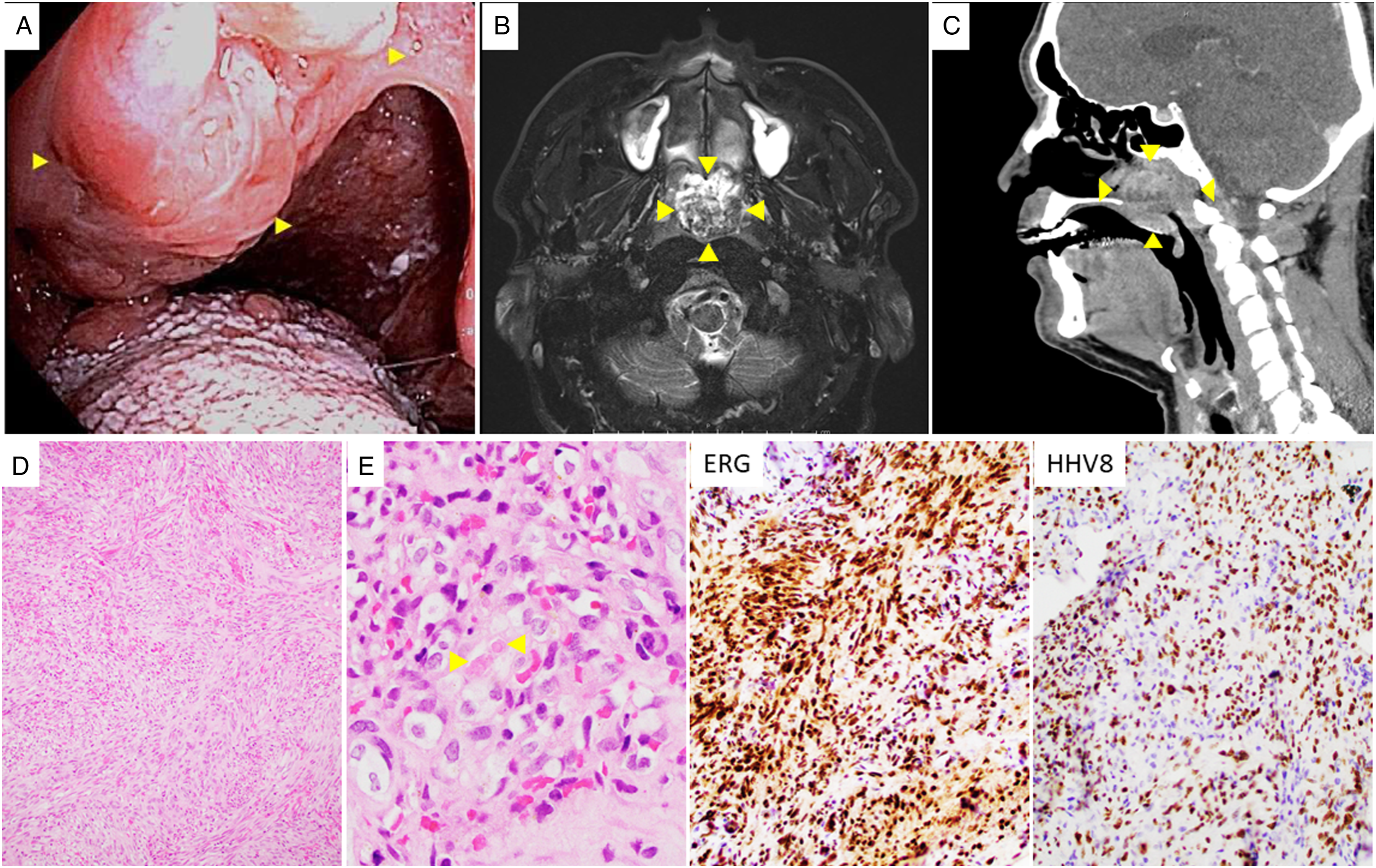
Discussion
Isolated Kaposi sarcoma in the upper aerodigestive system in immunocompetent patients.
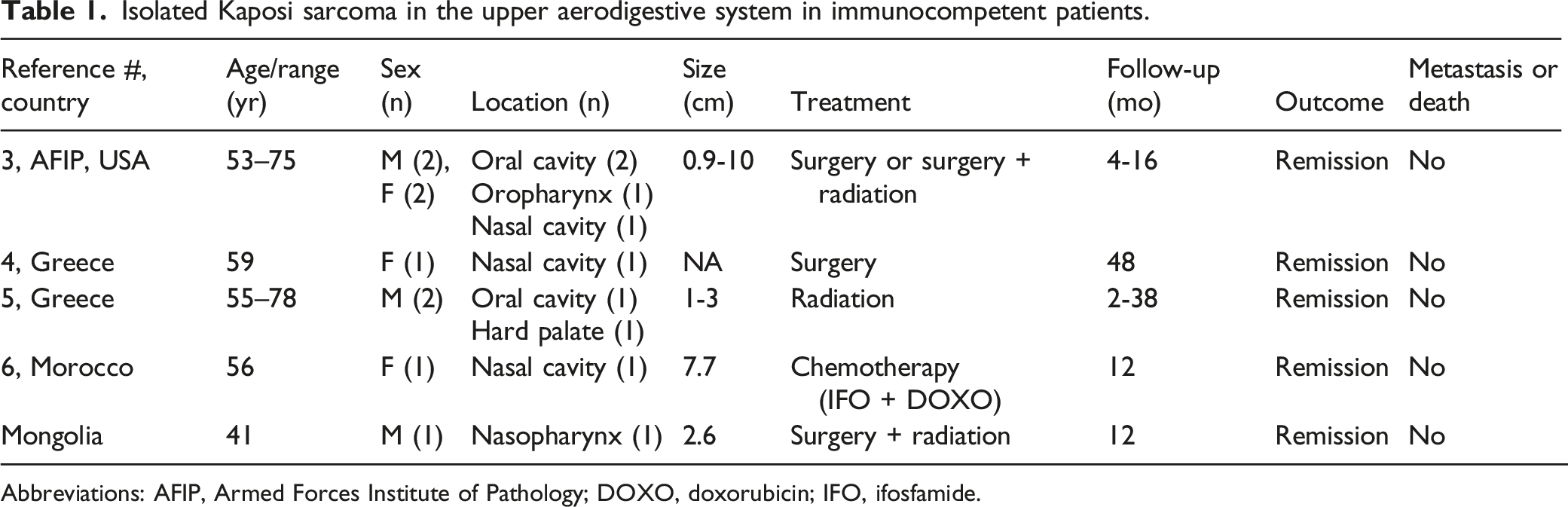
Abbreviations: AFIP, Armed Forces Institute of Pathology; DOXO, doxorubicin; IFO, ifosfamide.
There are no standardized treatment guidelines for Kaposi sarcoma. Therapy is usually guided by the tumor stage, symptoms, immune status, and comorbidities. 9 Treatment of immunocompromised patients is primarily geared towards immune restoration whenever possible. Regardless of immune status, non or minimally symptomatic, stable disease, usually does not require intervention, just follow-up. Progressing or symptomatic mucocutaneous lesions can be treated with topical agents such as alitretinoin or imiquimod, intralesional vinblastine, cryotherapy, and photodynamic therapy. Symptomatic, mass-forming, extracutaneous localized disease is usually treated with surgical excision, with adjuvant radiotherapy for unclear, close, or positive margins, as was done in our case. Disseminated and/or symptomatic irresectable disease is usually treated with single agent chemotherapy with or without radiotherapy. Commonly used agents include pegylated liposomal anthracyclines and paclitaxel. 11
Advances in the understating of the oncogenic effects of HHV8 on endothelial cells have led to the identification of several potential targeted therapies, which at the time of the publication of this article have not been approved for clinical use.
Targeted therapies
Conclusions
Isolated involvement of the upper aerodigestive tract by KS in immunocompetent patients is exceedingly rare. The limited number of cases reported to date have shown an indolent biologic behavior and were successfully treated with surgery, radiation, chemotherapy, and combination surgery/radiation without significant complications; however, follow-up is limited. Several reports of successful treatment of advanced KS with targeted therapies suggest that this neoplasm is amenable to be treated with non-invasive, less morbid therapeutic modalities. Adoption of these newer therapies will likely be delayed by the effectiveness of existing conventional therapies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Indiana University School of Medicine, Indianapolis IN.
Ethics approval and consent to participate
Per institutional guidelines only patient’s consent is required, ethics committee approval is not needed.
Consent for publication
A standard consent form authorizing the use of surgical specimens for research and/or education provided the information is deidentified has been signed by the patient.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated during the current study.