
Abstract
A man with a history of neurofibromatosis presented to our hospital with a soft palate mass. Since the patient had neurofibromatosis, we diagnosed the mass as a neurofibroma and planned annual regular follow-up without any treatment. Five months later, the patient visited our emergency department because of uncontrolled epistaxis, and the mass was enlarged to the extent of the airway obstruction. Endoscopic resection was performed and the tumor was confirmed to be a leiomyosarcoma. The malignant potential of the new lesion in a neurofibromatosis patient should be actively evaluated and treated, if required.
Significance statement
A 62-year-old man with a 40-year history of neurofibromatosis presented to our hospital with a soft palate mass. Since the patient had neurofibromatosis, we diagnosed the mass as a neurofibroma and planned annual regular follow-up without any treatment. He had been diagnosed with prostate cancer 2 months earlier and was scheduled for radiation therapy of prostate. Five months later, the patient visited our emergency department because of uncontrolled epistaxis. Hb was 12.1 mg/dL. Nasal endoscopy revealed a lobulated round mass in both the nasopharynx and soft palate (Figure 1(a)). Computed tomography (CT) and magnetic resonance imaging (MRI) demonstrated that an approximately 3 x 3 x 4.8 cm sized well-defined, round lobulated mass was located in the soft palate and extended to the nasopharynx (Saadoun et al., 2022) (Figure 1(b) and (c)). Endoscopic resection was performed under general anesthesia. A mucosal incision was made at the posterior end of the soft palate using electrocautery. The tumor was dissected preserving the palatopharyngeus and palatoglossus muscles, and completely removed by electrocautery (Figure 1(d)). On the final pathological examination (Katre et al., 2017), the tumor was confirmed to be a leiomyosarcoma (Figure 1(e) and (f)). Recurrence was not observed during the follow-up period. Although it appears to be a benign tumor, because it may be malignant in patients with neurofibromatosis, pathological examination or surgery should not be delayed to remain within an appropriate treatment period. In the treatment of patients with neurofibromatosis, the development of a mass is generally initially diagnosed as a neurofibroma; however, the malignant potential of the mass should be actively evaluated and treated, if required (Onoe et al., 2009). (a) Nasal endoscopy revealed a dark bluish-colored mass in the right nasopharynx and a reddish-colored mass in the left nasopharynx. The mass had pushed the soft palate anteriorly. (b) A computed tomography (CT) scan showed an irregularly shaped, heterogeneously enhanced mass in the soft palate. (c) MRI revealed an irregularly shaped mass with a heterogeneous high signal on the T2-weighted image. (d) A 3 x 3 x 4.8 cm sized mass was excised by en-bloc resection. (e) The tumor consisted of hypercellular spindle cells with marked nuclear atypia and mitosis (Zhang et al., 2019), x200. (f) Actin positivity of tumor cells, x200.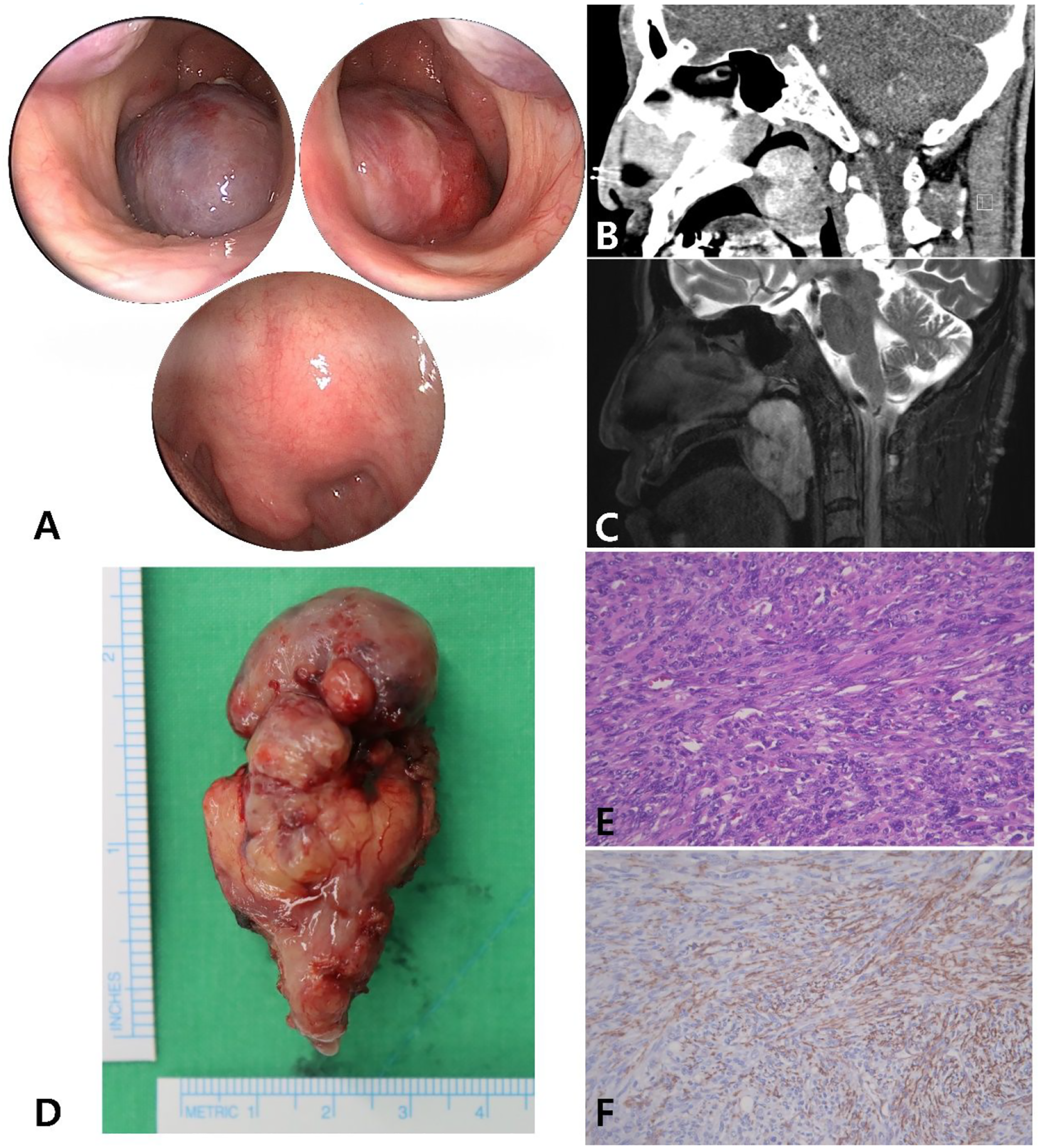
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NRF grant funded by the Korean Government (MSIT) (No. 2021R1G1A1094681) and by the project for Industry-Academic Cooperation Based Platform R&D funded by the Korea Ministry of Small and Medium Enterprises (SMEs) and Startups in 2021 (No. S3017921). This research was supported by a Young Medical Scientist Research Grant through the Seokchunnanum Foundation (SCY2113P) and by the fund of the Biomedical Research Institute, Jeonbuk National University Hospital. This work was supported by the Ministry of Health & Welfare, Republic of Korea (grant number: HI22C1124).