
Abstract

Keywords
Significance Statement
We have demonstrated a very rare case of undiagnosed/untreated primary cutaneous cryptococcosis (PCC) causing extensive destruction of left nasal ala in a patient with human immunodeficiency virus infection. Identification of the histological features of gelatinous type cutaneous cryptococcosis with appropriate clinical work-up shown in this case, is the key for making the correct diagnosis.
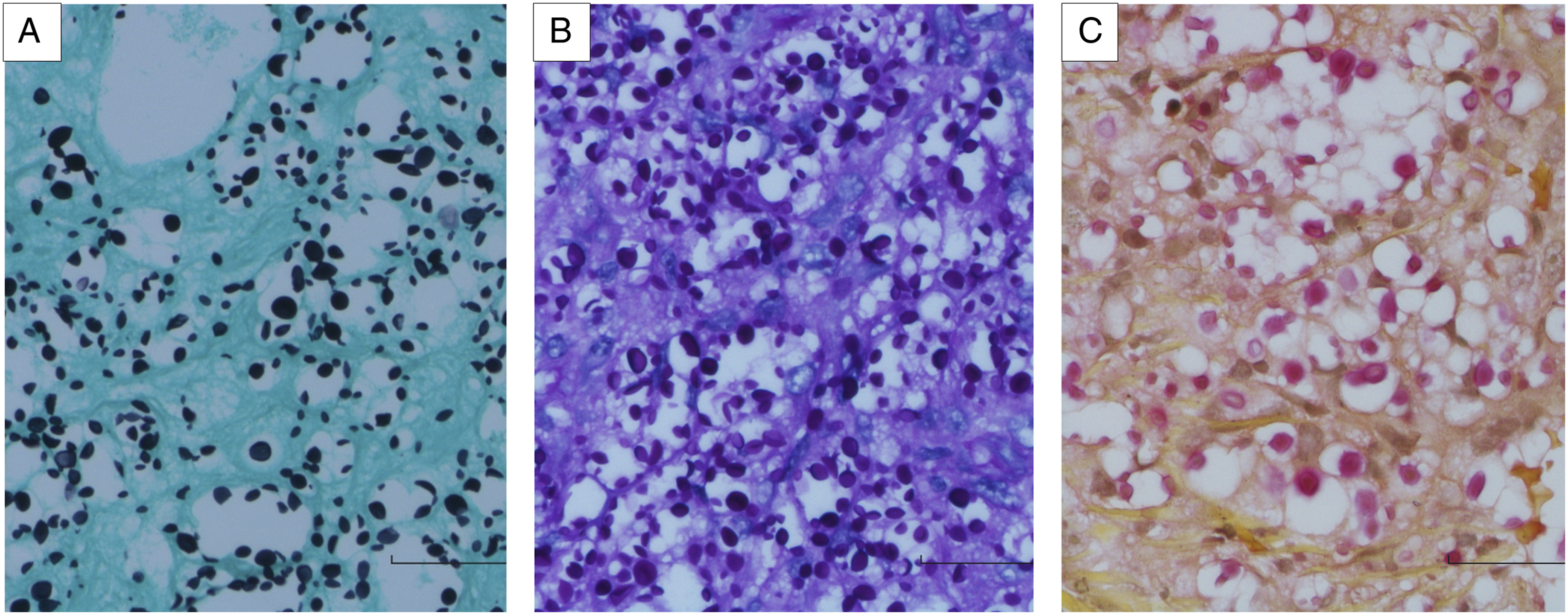
A 43-year-old male, with past medical history of human immunodeficiency virus (HIV) infection 17 years ago and lung Pneumocystis jirovecii infection three years ago, presented with shortness of breath, non-productive cough, and complaint of his nose slowly “being eaten away” over the past 5 years after a bike accident. Imaging and labs were consistent with Pneumocystis jirovecci pneumonia in the setting of long history of noncompliance with highly active antiretroviral therapy (HAART) and a low CD4 count of 45. The patient was started on treatment for Pneumocystis pneumonia and achieved the clinical and radiological improvement. Lab work also showed serum positive crytococcus antigen with a titer of 1:20. Physical examination of head and neck showed most of the left nasal ala was completely destroyed, with visualizable nasal septum (Figure 1A). The punch biopsy of the left nasal ala showed skin with foamy dermis at low power (Figure 1B). The dermis stroma had variable sized clear spaces filled with yeast-form microorganisms in the background of scant fibrous cells and thin walled vessels, with little inflammatory cell infiltrate, under intermediate power (Figure 1C). High power view demonstrated numerous yeasts with marked variation in size and shape (Figure 1D). Grocott methenamine silver (GMS) and Periodic Acid-Schiff with diastase (PAS-D) special stains highlighted the yeasts with narrow based budding (Figures 2A and B). The mucin in the capsules of the yeasts was demonstrated by Mucicarmine special stain (Figure 2C). The diagnosis of cutaneous cryptococcosis, gelatinous type, was rendered. Culture for Cryptococcus neoformans on the nasal lesion was positive, which confirmed the diagnosis. Cerebrospinal fluid (CSF) obtained by lumbar puncture to rule out disseminated cryptococcosis was negative for Cryptococcus by culture. Primary cutaneous cryptococcosis (PCC) was considered based on no disseminated disease found, positive serum Cryptococcus antigen with low titer (1:20), positive culture for Cryptococcus neoformans, and the history of nasal skin injury. The patient received appropriate systemic antifungal treatment for PCC. The left nasal ala lesion and the biopsy findings (H&E Stain). (A). The left nasal ala is completely destroyed. (B). The skin punch biopsy shows superficial and deep dermis with foamy stroma (20X). (C). The dermis displays foamy stroma with minimal inflammatory cell infiltrate (100X). (D). There are numerous yeasts identified under high power (400X). Various sized cryptococci highlighted by multiple special stains (400X). There are numerous yeasts with narrow based budding highlighted by GMS (A) and PAS-D (B) stains. The mucin in the capsules of the yeasts was demonstrated by Mucicarmine stain (C).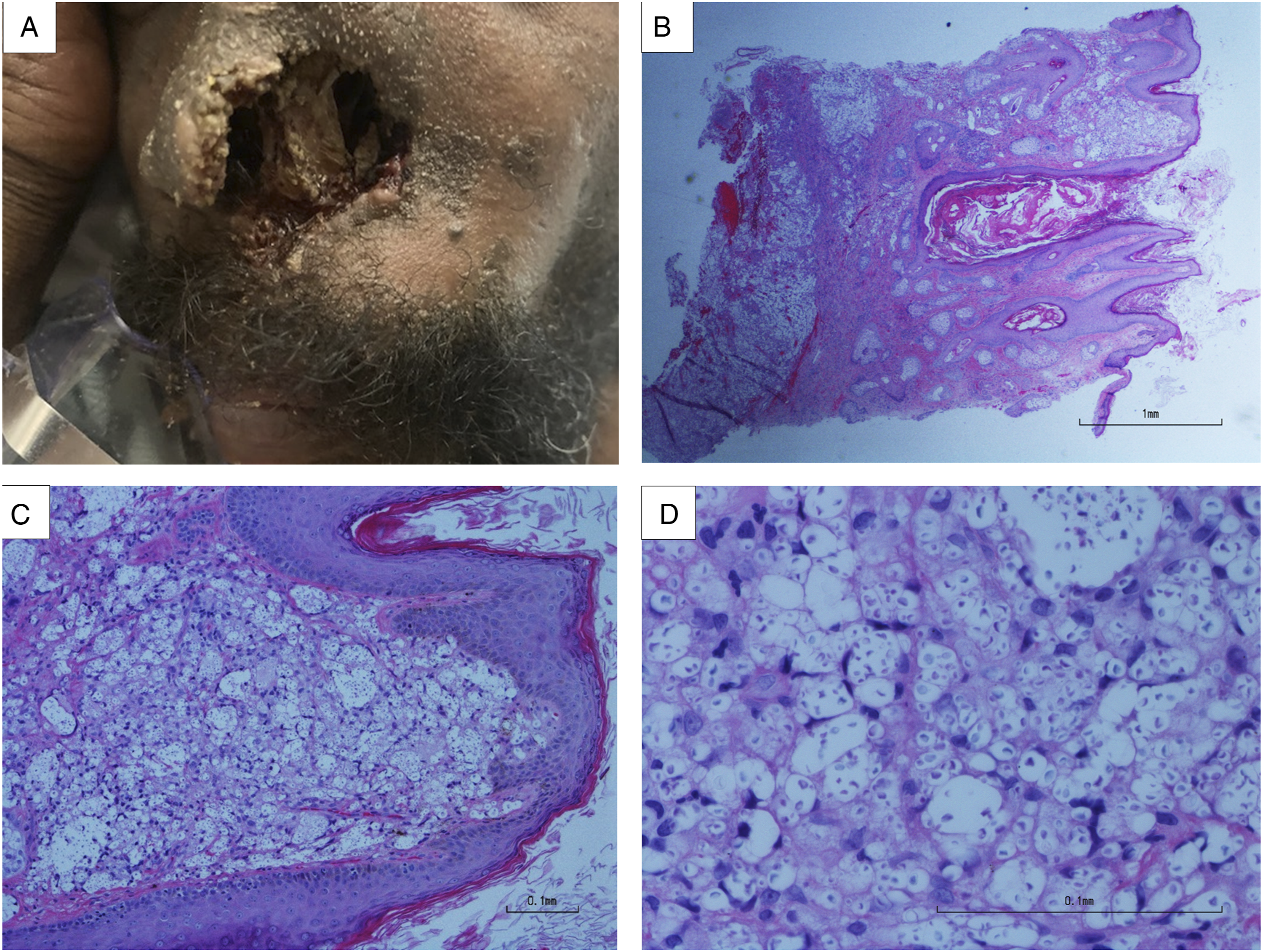
Discussion
Primary cutaneous cryptococcosis has been defined as skin lesion(s) confined to a circumscribed body region, positive skin culture for Cryptococcus neoformans, and no sign of simultaneous dissemination (a regional lymphadenopathy not considered dissemination). 1 A large-scale retrospectively study of PCC in France demonstrates the results of the investigation of total 1974 cases of cryptococcosis. The analysis indicates 108 cases with positive skin culture results. Among the 108 cases, there are 28 patients (16 males, 12 females) considered to have PCC. Subsequent analysis of the 28 patients has showed the risk factors predisposing to cryptococcosis in 14 patients, including HIV in 3 patients, cancer in 6 patients, history of solid-organ transplant in 2 patients, rheumatoid arthritis in one patient, sarcoidosis in one patient, and idiopathic CD4 lymphopenia in one patient. The study also shows 14 patients lived in rural areas, and 23 patients with a main occupation or hobby predisposing to skin injury. 6 The risk factors in our patient are history of HIV infection and skin injury. The process of PCC causing extensive damage of the left nasal ala in our case is in five years.
The clinical manifestations of skin lesion in the 28 patients with PCC in the French study mentioned above include ulceration in 3 patients, whitlow in 7 patients, cellulitis in 4 patients, phlegmon in 10 patients, nodule in 3 patients, and scratch-like appearance in one patient. 1 None of them have extensive tissue destruction as that seen in our case. In addition, there are 26 patients received systemic treatment (17 patients also received surgical resection), and 2 patients with no treatment. Our patient has received systemic antifungal treatment since the diagnosis of PCC rendered.
Histopathology findings characteristic of cutaneous Cryptococcus infection show either a paucireactive pattern or a mixed suppurative pattern. 2 Our case shows the features of paucireactive pattern, mostly seen in immunocompromised patients. In paucireactive pattern, there are densely packed organisms with mucoid gelatinous capsules that cause minimal tissue reaction, typically caused by Cryptococcus neoformans. 2 The mixed suppurative pattern is observed usually in immunocompetent patients. It shows granulomatous inflammation and varying degrees of necrosis. 2 Infection in immunocompetent individuals is more commonly caused by Cryptococcus gattii in the endemic areas like Papua New Guinea and Northern Australia.3,4 In cases of paucireactive pattern, the characteristic carminophilic capsules of Cryptococcus neoformans lead to a diagnosis. 5 The spore of Cryptococcus Neoformans measures 3 to 20 micromillimeters in diameter and stains well with PAS-D and GMS special stains. 5 The mucin in the capsule can be highlighted by Mucicarmine special stain. Differentiating Cryptococcus species from Histoplasma capsulatum, Sporotrichosis schenckii, Paracpccodiodes brasiliensis, and Blastomyces dermatitidis are important when only GMS staining the fungal spores with narrow based budding, but the characteristic capsules of Cryptococcus not revealed in Mucicarmine stain.2,5 In such cases, culture will be important and helpful for the diagnosis. 6 Our case of cutaneous cryptococcosis in an immunocompromised/HIV infected patient demonstrates typical histologic features of paucireactive pattern of cutaneous Cryptococcus, with the diagnosis confirmed by positive culture for Cryptococcus Neoformans.
Primary cutaneous cryptococcosis is usually diagnosed by the biopsy of skin lesion with histological criteria (lesion confined to the skin and subcutis), or culture, in addition to the absence of dissemination. Cryptococcemia or dissemination refers to the involvement of at least two noncontiguous sites or evidence of high fungal burden based on cryptococcal antigen titer ⩾1:512. 7 In our case, the diagnosis of PCC is supported by positive serum Cryptococcus antigen testing showing low titer (1:20) and CSF obtained from lumbar puncture negative for Cryptococcus by culture. The lab results in our patient indicate systemic Cryptococcus infection is unlikely.
Cutaneous lesions can be the only symptom and an early marker of disseminated disease. 8 Even if antigen positivity can indicate severe local infections, it can also be an early indicator of brewing cryptococcal meningitis. 8 The diagnosis of PCC should prompt the analysis of the host's immune status. 8 Misdiagnosis or underdiagnosis could be an alternative explanation of why the incidence of cutaneous Cryptococcus infection seems low. Skin lesions may seem innocuous to persons used to repeated wounds, thereby preventing recording of the diagnosis. 9 Clinicians should be aware that C. neoformans can be responsible for unexplained skin lesions that are unresponsive to antibiotics, even in apparently healthy persons.
In conclusion, we have demonstrated a very rare case of undiagnosed/untreated PCC causing extensive destruction of nasal tissue. Identification of the histological features of cutaneous cryptococcosis with appropriate clinical work-up shown in this case, is the key for making the correct diagnosis of PCC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.