
Abstract
An innovative and noninvasive technique for closure of persistent tracheoesophageal fistula after total laryngectomy is described. In our preliminary study, two patients were included. No clinical and radiological signs of locoregional recurrence prior to treatment were diagnosed. We performed local injections of autologous platelet-rich plasma (PRP) according to our protocol. Complete closure of the fistula was observed in both patients who were able to take normal feeding. No side effects associated with the procedure were observed. These preliminary results are encouraging to consider PRP injection before more invasive surgical techniques in the treatment of persistent tracheoesophageal fistulas after total laryngectomy.
Introduction
Persistent tracheoesophageal fistulas (TEF) after total laryngectomy are difficult to treat. A TEF generally results from the enlargement of a tracheoesophageal puncture made for the placement of a voice prosthesis. Actually, many factors that predispose to the development of TEF are described: preoperative or postoperative radiotherapy, preoperative nutritional insufficiency, gastroesophageal reflux, advanced nodal status (>N2), locoregional recurrence, and tumor localization. 1
Nowadays, closure of the fistula may be favored by several conservative techniques such primary wound closure and injection of expansive materials (hyaluronic acid, autologous fat, etc). If conservative treatment is insufficient or ineffective, then surgical management using flaps. 2 But if surgery is not successful, few therapeutic options existed.
In our preliminary study, an innovative and noninvasive technique applied into two patients seems to be promising to obtain a complete closure of tracheoesophageal fistula.
Methods
Participants
The participants were patients treated and followed in the Head and Neck surgery Department of Saint-Pierre Hospital in Brussels. These patients had persistent tracheoesophageal fistula after total laryngectomy. Two patients with no signs of recurrence were included in the study and received the protocol injection.
The study was approved by the Ethics Committee of CHU Saint Pierre.
Informed consent was submitted to the patients.
Therapeutic Protocol
Platelet-rich plasma was obtained based on the protocol GS3-PURE II Protocol A (Emcyte, ft Myers, Florida). The procedure is as follows: 3 milliliters of sterile sodium citrate 4% was collected in a 20 mL syringe. The same syringe was used to draw 10 mL of blood from the patient. The blood was centrifuged at 2200 r/min during 8 min (using Tabletop Low Speed Centrifuge). The platelet plasma suspension supernatant was aspirated and re-centrifuged during 5 min at 4000 r/min. The platelet poor plasma supernatant was then discarded and the remaining 2 mL of PRP was drawn up for injection.
After decanulation of the patient, the injection site was carefully cleaned and disinfected. Using No. 11 scalpel blade, fistula edges were carefully excised. Approximately 2 mL of PRP was injected in 4 quadrants of the fistula. The total duration of the protocol from drawing blood to the injection of PRP lasted approximately 25 min.
The further need of more PRP treatments was determined upon local healing of the fistula. A minimum of 5 days and a maximum of 14 days were held between 2 treatments.
Case Reports
Case 1, From February to April 2019, a 64-year-old male was treated by concomitant radiochemotherapy for a hypopharyngeal squamous cell carcinoma (T4aN2cM0). In March 2020, the patient developed very severe laryngeal dysfunction requiring a functional pharyngo-laryngectomy with reconstruction using the right pectoralis major flap. During the procedure, tracheoesophageal puncture was performed, and a voice prosthesis was placed. Necrosis of the tracheoesophageal wall occurred during hospital stay with development of a large TEF (>2 cm) confirmed by a barium swallow test (Figure 1). One year after the treatment, surgical debridement and a left pedicled supra-clavicular flap was performed without success. Barium swallow test, the dotted circle indicates the fistula.
A last surgical treatment was performed 1 month after, using a left pedicled fascio-cutaneous flap resulting in an even larger necrosis of the tracheoesophageal wall. However, the last intervention allowed a closure of approximately 1.5 cm of diameter after 2 weeks but remained stable afterward. A cervicothoracic CT-scan confirmed the persistent fistula (Figure 2). A: the dotted circle indicates the fistula before injection B: complete closure.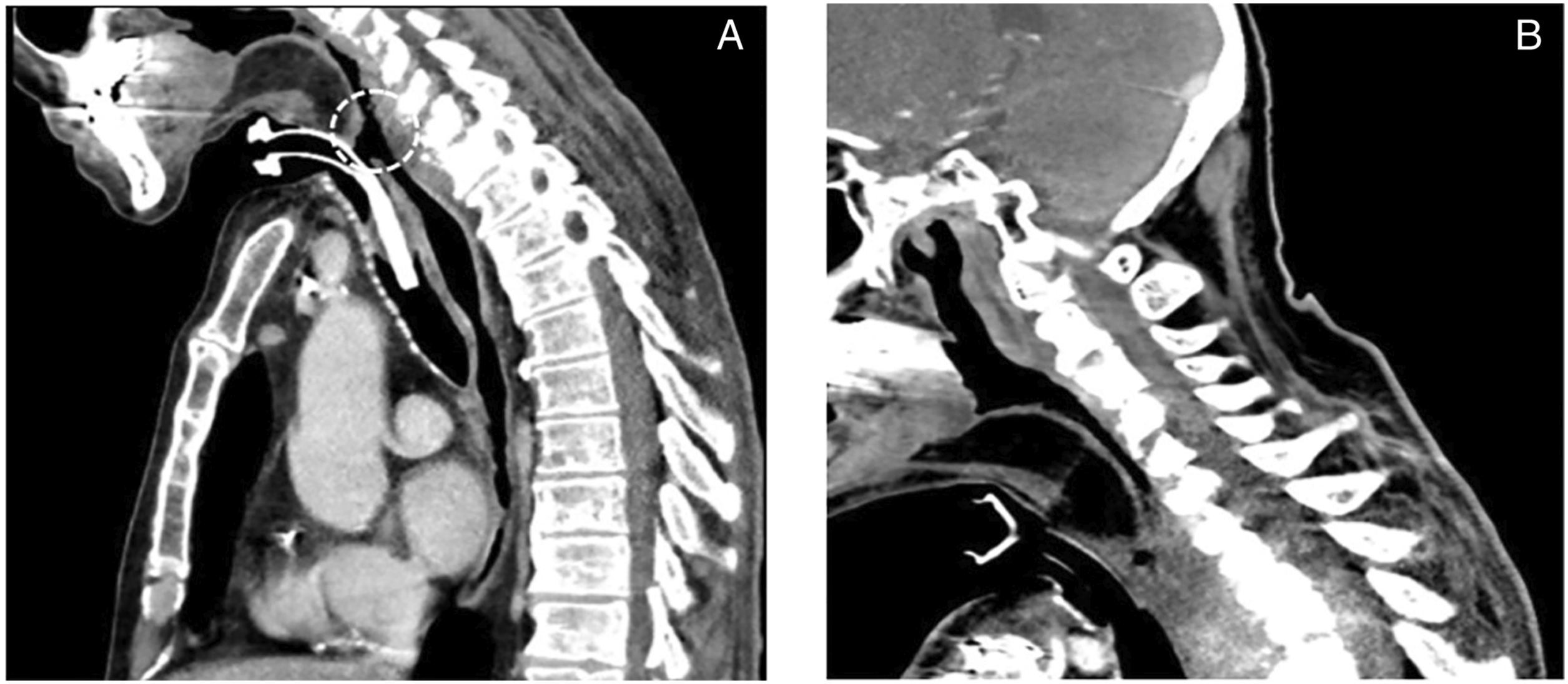
Because the small size of the TEF and in order to limit the morbidity of a new surgical treatment, we decide to apply PRP injection to close the TEF. One month after the last surgery, the first PRP treatment was performed on non-inflammatory tissue during the same hospital stay. A second treatment was performed 5 days later and two weeks after the last injection, a methylene blue dye test confirmed the complete closure of the fistula which permitted the patient to start an oral diet.
Case 2, a 58-year-old male was treated by concomitant radiochemotherapy for a squamous cell carcinoma localized at the left part of the hypopharynx (T3N2cM0) from February to March 2016. A tracheotomy was performed in June 2016 for dyspnea followed by a functional pharyngo-laryngectomy with reconstruction using left pectoralis major flap 4 months after the treatment. A tracheoesophageal puncture was performed, and a voice prosthesis was placed. Few months after, the patient suffered from repeated right peri-prosthesis leakages. Multiple types of prosthesis were attempted but leakage was followed a maximum of 3 months systematically with a right lateral shift of the prosthesis. The voice prosthesis was then removed, revealing a small (<2 cm) right TEF. No spontaneous closure was obtained. After 2 months, a first attempt at closing with per primam suture was performed without success. A new leakage appeared after 1 year and a small TEF was confirmed by a methylene blue dye test. A first PRP treatment was proposed and performed in February 2021. Two weeks later, a second treatment was conducted after a methylene blue dye test showed a very minimal leakage. A third and last injection of PRP took place after 1 week resulting in complete closure of the fistula.
Discussion
Tracheoesophageal fistula is a non-rare complication after total laryngectomy and may delay resumption of feeding and cause a longer hospital stay. The fistula usually appears at the site of the voice prosthesis by a progressive enlargement of puncture. Many factors can be involved: radiotherapy, malnutrition, local infections, traumatic factors, gastroesophageal reflux, etc. Once the prosthesis is removed, the TEF spontaneously closes in the majority of cases. In patients with persistent leakage, conservative techniques are described to promote fistula closure before considering a more invasive surgical management. 2 In our study, Neither spontaneous closure or closure after invasive surgery were achieved in both patients. Therefore, a new therapeutic approach has been chosen: a local injection of autologous platelet-rich plasma.
Platelet-rich plasma is a preparation of autologous human plasma with an increased platelet concentration produced by centrifugation.
The process of creating PRP is based on the different settling velocity of components of whole blood, called plasmapheresis. The initial centrifugation separates the plasma and platelets from the red and white cells. The resulting plasma supernatant is also centrifuged to separate plasma into platelet-poor plasma and platelet-rich plasma PRP. In vitro studies have demonstrated that PRP significantly increase levels of growth factors and suppress inflammation process by a specific enzymatic cascade. 3 Some of these growth factors have important chemotactic, mitogenic, and anabolic properties. Platelet-rich plasma also is an important source of EGF, VEGF, and FGF-b involved in the formation of new blood capillaries in healing. 4 Thus, PRP delivers significant amounts of growth factors, which are essential to wound healing and regeneration. 5
Actually, the efficiency of PRP treatments in healing process have been proved in many medical conditions such as musculoskeletal injuries, esthetic surgery, dermatology, dental, and maxillofacial surgery.
Recently, PRP have showed interesting results in the management of tracheobronchic fistulas (TBF). A local auto-PRP injection was performed in 3 patients with tracheobronchic fistula with a variable injection protocol. All the TBF were completely closed within a range of 15 to 18 weeks. 6
In our first patient, after failure of both flaps, we decided to perform the auto-PRP injection 1 month after the last surgery, during hospital stay. The second patient presented a chronic leakage through a TEF. The PRP injection was proposed 2 years after prosthesis removal. The TEF were completely closed approximately 3 weeks after PRP treatment and made possible normal oral feeding.
These promising results encourage auto-PRP injection as a therapeutic alternative before more invasive surgical techniques, both in acute and chronic leakage through small TEF (<2 cm).
To the best of our knowledge, we believe this is the first study that investigate the effect of PRP for the management of TEF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patient gave his consent for this publication.
Data Availability
All data concerning this case report are available at the corresponding author