
Abstract
Purpose:
Endoscopic sinus surgery (ESS) is the standard treatment strategy for chronic rhinosinusitis (CRS) resistant to medical treatment, and it is known to have postoperative complications and recurrences, which in turn result in suboptimal outcomes. Several methods are used to prevent postoperative scarring, adhesions, oedema, infection or recurrences in cavities. The role of steroids in improving postoperative outcomes is well established. They can be administered systemically or locally to enhance drug delivery into paranasal sinuses. In this study, we used triamcinolone irrigation immediately following surgery on one side of the nose, in patients with bilateral disease. The objective of this study was to evaluate the effect of intra-operative triamcinolone irrigation on postoperative outcomes, in patients with bilateral pansinusitis.
Methods:
It was an interventional randomized controlled study, conducted at a tertiary care centre in North India. The analysis of 58 patients with bilateral pansinusitis was done from September 2020 to August 2021. At the conclusion of ESS, each patient was randomized to receive triamcinolone irrigation (4 ml of 40mg/ml solution) once and followed by merocel (polyvinyl acetal) packing on one side, while the contralateral side was packed with merocel soaked with saline. Nasal cavities were evaluated using a Hopkins rod endoscope in the postoperative 1st, 3rd, 8th and 12th weeks to look for the presence of postoperative crusting, oedema, polypoidal changes, and discharge. Perioperative sinus endoscopic scores (POSE) were used for endoscopic staging.
Results:
The most commonly affected age group was 31-45 years accounting for 39.7%. Males were affected more (63.7%) than the female population (36.3%). There was a reduction in the average POSE scores at the treatment site at all follow-up stages with a significant reduction in crusting, oedema, and scarring in the treatment site (P-value <0.001).
Conclusion:
Triamcinolone irrigation effectively improves postoperative outcomes and reduces early postoperative complications in CRS patients.
Introduction
Chronic rhinosinusitis with sino-nasal polyposis is a challenge for the patient as well as the treating surgeon due to its nature of chronicity and tendency to recur. CRS significantly affects the quality of life, and it is pretty comparable to other chronic diseases like diabetes, asthma and COPD (chronic obstructive pulmonary disease). 1 The well-healed sinus cavity is a known determinant of a successful outcome following endoscopic sinus surgery (ESS). Common causes of suboptimal results following endoscopic sinus surgery include recurrent inflammation, polyposis, adhesion/synechiae formation, postoperative crusting, middle turbinate lateralization, stenosis of the surgically enlarged sinus ostia and scarring of the frontal recess area. These can be reduced with adequate postoperative care and frequent nasal douching. 2 It is well established that corticosteroids play a significant role in managing CRS with or without polyps. 3 Various studies have shown beneficial effects of postoperative steroidal irrigation in improving outcomes following ESS. 4 The use of systemic steroids is associated with systemic complications, and there is no strong evidence suggesting that topical steroids in a spray delivery system are beneficial or not due to insufficient concentration being reached at the surgical site. 5 Based on this evidence, this study aims to evaluate the effect of steroids, delivered locally as irrigation in sinus cavities (maxillary, ethmoids, frontal and sphenoid), immediately following ESS, in improving early postoperative wound healing and endoscopic findings. Based on this background, the objectives of the present study were to assess the effect of intra-operative triamcinolone irrigation in cases of bilateral pansinusitis involving all the sinuses, that is, maxillary, ethmoids, sphenoid and frontal, on postoperative oedema, crusting, secretion, scarring/ synechiae and polypoidal mucosal change 6 immediately following endoscopic sinus surgery on one side in comparison with the other side having similar disease pattern with no postoperative triamcinolone irrigation.
Methodology
Study Design
It was a single-centre matched-pair randomized controlled trial conducted between September 2020 and August 2021.
Study Settings
The study was conducted at a tertiary care hospital in North India. Subsequently, the assessment was performed in all cases who underwent bilateral FESS with intra-operative use of triamcinolone irrigation unilaterally, and clinical outcomes were evaluated. Information was collected from the patient records regarding the patient's age, gender, comorbidities and disease severity based on preoperative computed tomography (CT) scan, intra-operative findings and endoscopic findings on follow-up visits.
Study Participants’ Inclusion and Exclusion criteria
Eligible patients with Age: >15 years, from both the genders, diagnosed with bilateral CRS with pansinusitis, refractory to medical treatment and requiring bilateral ESS 6 (CRS with or without nasal polyposis having the same pattern of disease on both sides and requiring similar surgical procedures) were included in our study. While patients with any history of intolerance to triamcinolone, having allergic mucin, AFRS (allergic fungal rhinosinusitis), diseases like invasive fungal sinusitis, suspected malignancy, unilateral rhinosinusitis, with any history of previous nasal surgery, uncontrolled hypertension, diabetes or other systemic illness, unwilling or unable to comply with regular postoperative visits and the patients who developed surgical complications after surgery and those with fungal sinusitis diagnosed postoperatively with histopathology examination were excluded from our study.
All cases which met inclusion criteria during the study were included. The total number of patients identified was 58 (Figure 1). Informed consent was taken from all the patients. Baseline clinical and endoscopic examination along with radiological investigations in the form of computed tomography of paranasal sinuses was done. Symptomatic patients with chronic rhinosinusitis, refractory to medical management with or without polyposis, were taken up for surgery and functional endoscopic sinus surgery was done in general anaesthesia in all cases. Participants flow diagram.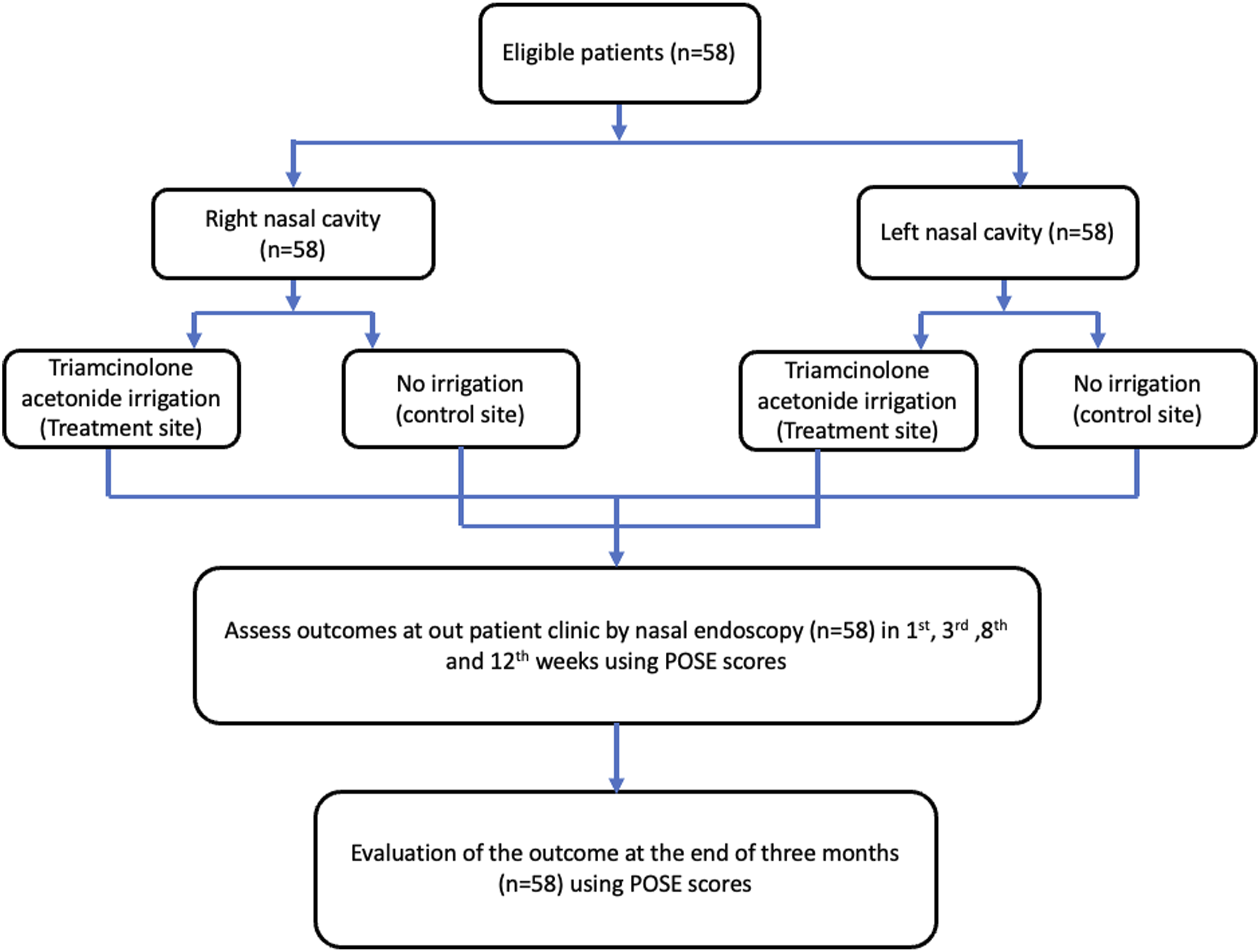
Pre-operatively, nasal cavities of all the patients were packed with cotton wicks soaked in 5 ml of 4% lignocaine and 5 ml of 1: 200000 adrenaline solution. Packs were removed before starting the surgery and nasal cavities were infiltrated with 5 ml of 2% lignocaine and 5 ml of 1: 200000 adrenaline solution. Cases with septal deviation obscuring the field of surgery also underwent endoscopic septoplasty to improve access to the sinuses. The Messerklinger technique was used as the main operative technique in all cases. Uncinectomy followed by frontal sinusotomy, middle meatal antrostomy, anterior and posterior ethmoidectomy were done in all the cases. At the conclusion of surgery, each patient received triamcinolone acetonide irrigation in all the sinus cavities (4 ml of 40mg/ml solution) on one of the randomly selected nasal sides, followed by 8 cm of polyvinyl acetal, that is, merocel (Medtronic, United States of America) nasal packing in the middle meatus. In contrast, the contralateral nasal cavity was not irrigated and the middle meatus was packed with merocel (polyvinyl acetal, 8 cm) directly, which served as control. Intra-operative irrigation allowed more contact time in the frontal sinus and sphenoid sinus facilitating better absorption by mucosa (Figures 2A and 2B). Nasal packs were removed on the third postoperative day. Patients were discharged with a prescription for systemic antibiotics (cephalosporins for 14 days postoperatively in all the patients); oral steroids (prednisolone 1 mg/kg/day in tapering dosage for 14 days postoperatively) were also prescribed to all the patients. At the time of discharge, instructions to the patients were given for alkaline nasal douching (taking 250 ml of plain water, cooled after boiling and dissolving half a teaspoon of table salt and quarter teaspoon of sodium bicarbonate) 4–5 times a day. Steroid nasal sprays (fluticasone furoate) were prescribed after the fourth postoperative week (POW). Patients’ follow-up endoscopic findings were reviewed on the 1st, 3rd, 8th week. (A) and (b): Triamcinolone acetonide irrigation in frontal sinus(*F) and sphenoid sinus(**S), respectively.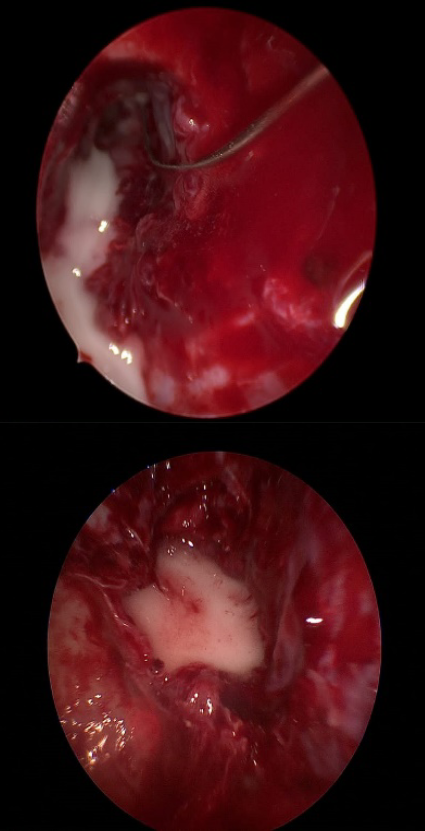
Symptom assessment was done in the third month of follow-up. Patients were examined using a Hopkins rod endoscope in Out-Patient Department by a single person to avoid observer bias. Endoscopic scoring was done during each visit as per perioperative sinus endoscopy (POSE) score, which assessed 1. Crusting (absent 0, mild 1 and severe 2), 2. oedema (absent 0, mild 1 and severe 2), 3. polypoidal change (absent 0, mild 1 and severe 2), 4. discharge (absent 0, thin/clear, that is, mild 1 and thick/purulent, that is, severe 2), 5. synechiae or scarring (absent 0, only in the middle meatus 1 and beyond middle meatus 2) and 6. stenosis or ostial patency.
Each parameter carries a minimum score of 0 and a maximum score of 2). 7 Both the patients and the person performing the endoscopic examination were blinded regarding the site receiving triamcinolone acetonide irrigation. In the immediate postoperative period, scarring or synechiae formation was the primary variable for assessing the surgical outcome, while reduction of crusting, oedema, discharge, polypoidal changes and maintenance of ostial patency or absence of stenosis were secondary variables. Statistical analysis was done using paired t-test, and a P-value of <0.05 was considered significant.
Results
In this study, 58 patients were recruited for the study who underwent bilateral endoscopic sinus surgery and intra-operative triamcinolone irrigation on one side after completion of surgery but before nasal packing. Although our inclusion criteria included cases of CRS with or without polyposis, most (86%) of the patients enrolled in our study had bilateral sino-nasal polyposis. The average length of follow-up from initial ESS to the last documented clinical visit was 12 weeks. Out of the 58 patients, 37 were male and 21 were female. The age range at the time of FESS was from 15 to 66 years of age. The majority of patients fell in the 30–45 years age group. Common symptoms and signs at the time of presentation were purulent nasal discharge (82%), postnasal discharge (94%), nasal obstruction (88%) and nasal polyposis (86%), headache (56%) and hyposmia (32%). Diagnostic nasal endoscopy findings included polyps (82%), middle meatal discharge (34.6%) and congested nasal mucosa (18%). Preoperative comorbidities like allergy (66%), asthma (24%) and other chronic diseases were managed in collaboration with respective clinical specialities. Preoperative CT findings showed the severity of the disease, and all our patients had severe disease, that is, bilateral pansinusitis.
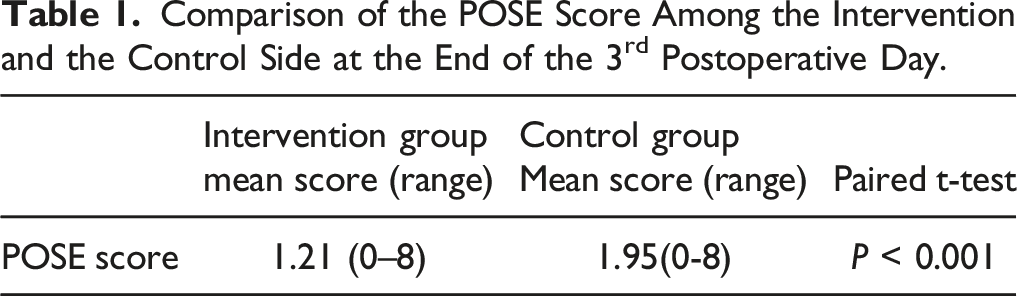
Comparison of the POSE Score Among the Intervention and the Control Side at the End of the 3rd Postoperative Day.
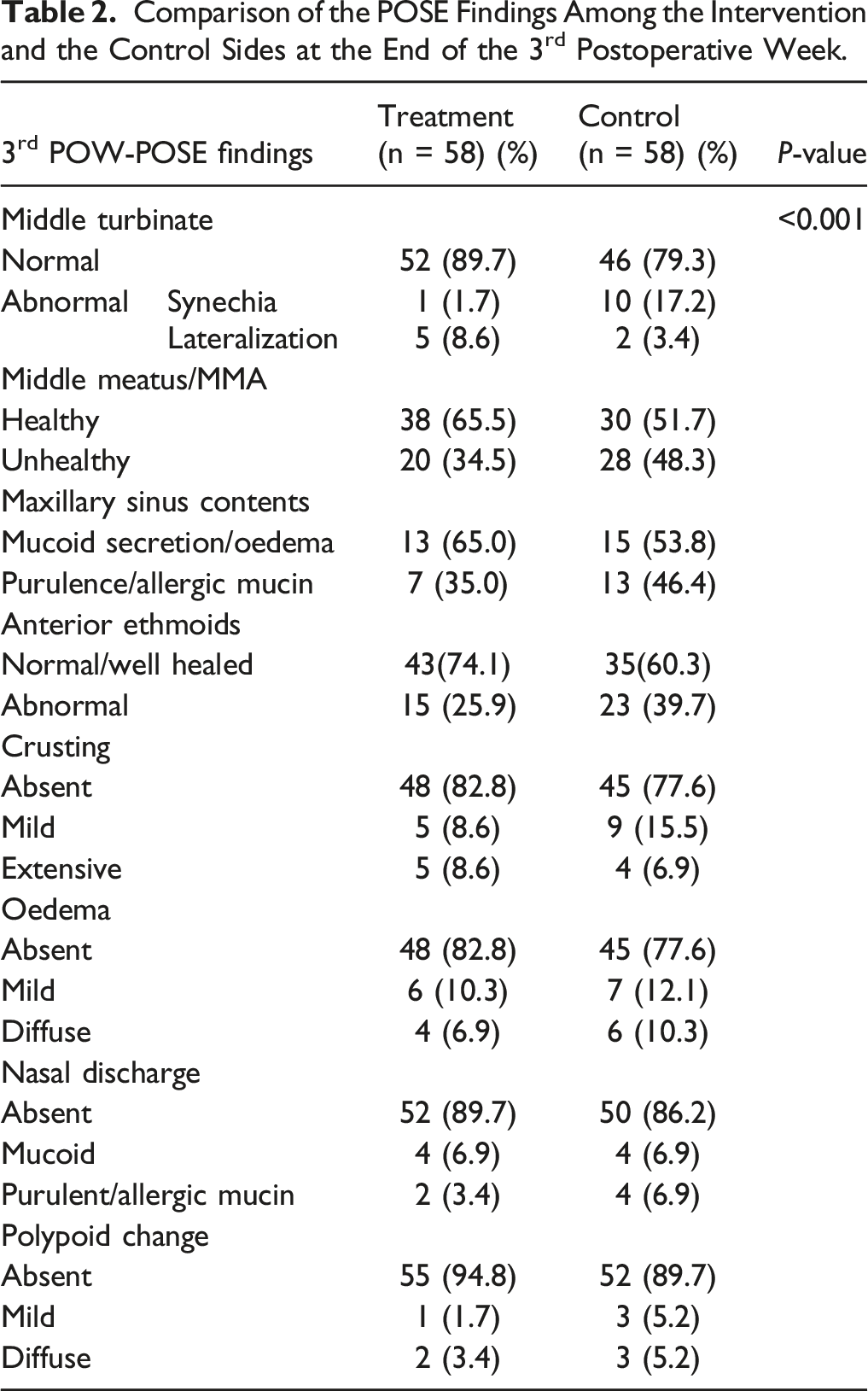
Comparison of the POSE Findings Among the Intervention and the Control Sides at the End of the 3rd Postoperative Week.
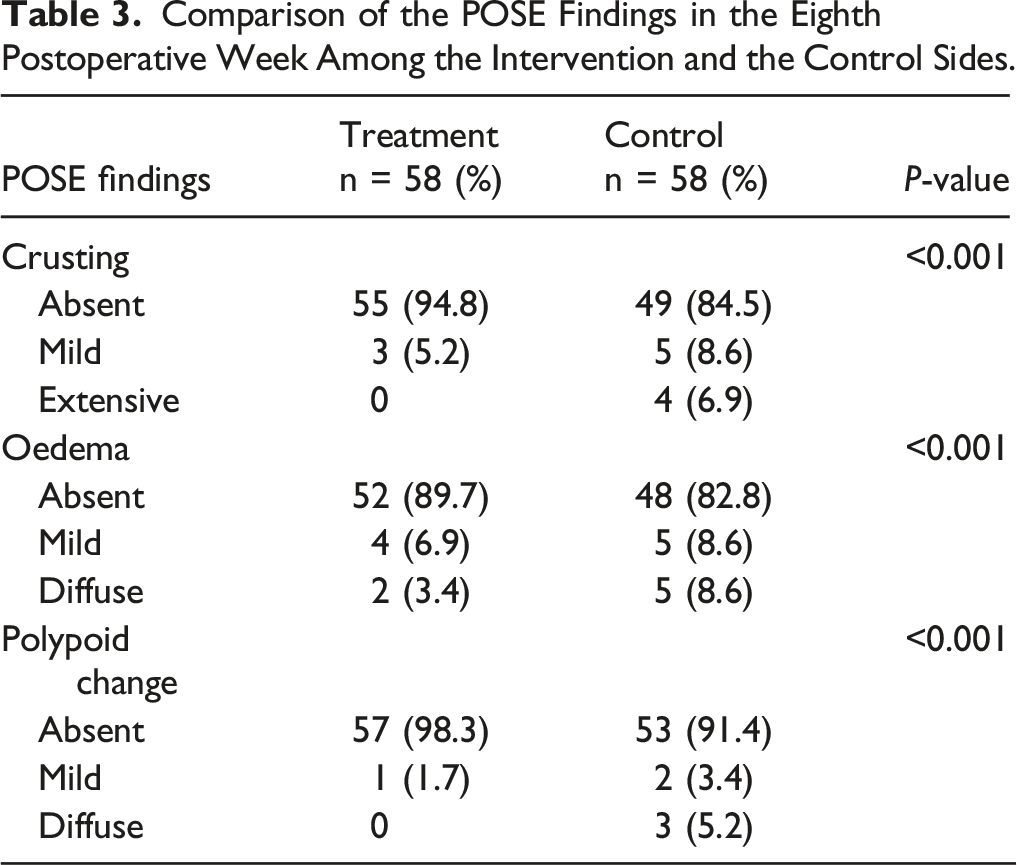
Comparison of the POSE Findings in the Eighth Postoperative Week Among the Intervention and the Control Sides.
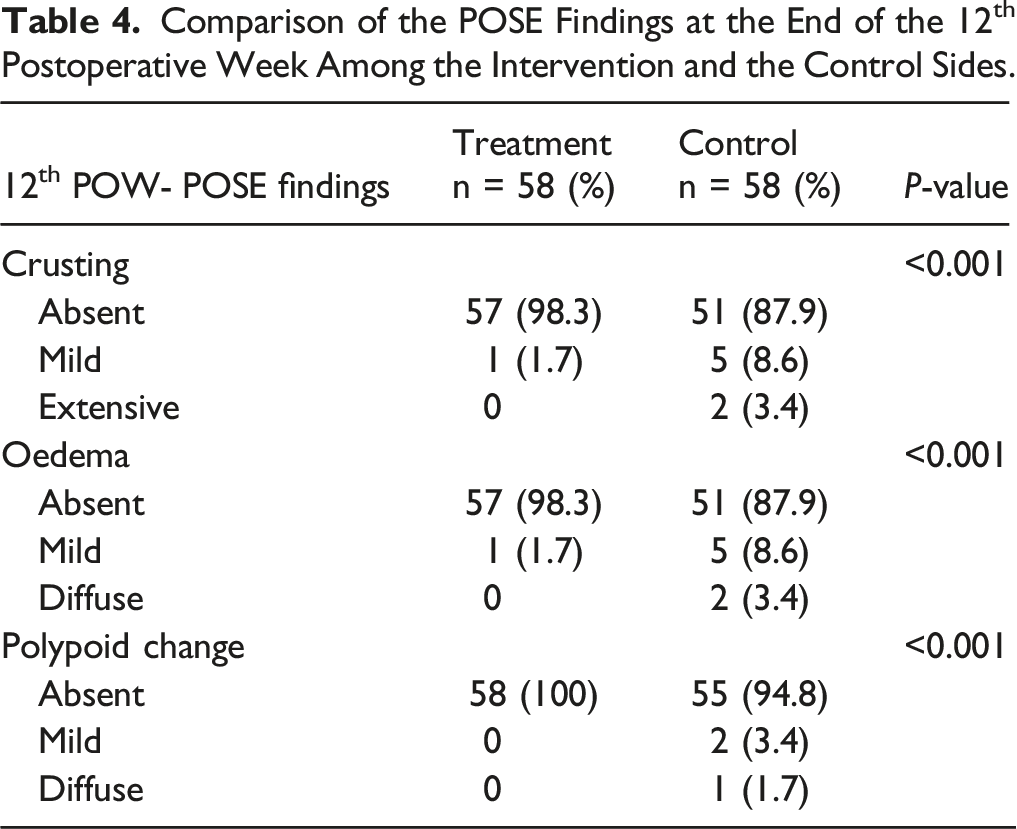
Comparison of the POSE Findings at the End of the 12th Postoperative Week Among the Intervention and the Control Sides.
Discussion
In our study, the most commonly affected age group was 31–45 years accounting for 39.7%, 36.2% aged 15–30 years, 22.4% old 46–60 years and 1.7% aged over 60 years. However, according to an epidemiological analysis of patients with nasal polyposis by Bettega et al., 8 polyposes is more common in the over 50 age group (37.5%) and rarely affect children and young people. The findings of Bettega et al. 8 were followed those of Settipane et al. 9 which showed that sino-nasal polyposis increased with age and peaked in those aged 50 years and older. Further, the male population was affected more (63.7%) in our study, than the female population (36.3%). This can be attributed to the increased prevalence of substance abuse in the male population. However, the epidemiological study by Bettega et al. 8 concluded that the male population had a lower prevalence of disease than females, accounting for 41.66%. Settipane’s 9 review of 211 sino-nasal polyposis patients showed an equal distribution between the male (50.2%) and female (49.8%) population. 9
During the entire follow-up period, we observed a statistically significant reduction in perioperative sinus endoscopy (POSE) scores in the test group compared to the control group. In our study, endoscopic assessment in the third POW, POSE score ranged from 0 to 8 in the treatment site and 0 to 8 in the control site. Our findings were similar to those in the study by Côté et al. 4 where POSE scores ranged from 1 to 8 in the treatment site and 3 to 11 in the control site. However, in the study by Rudmik et al., 10 where dexamethasone eluting spacer was used, endoscopic evaluation in the fifth POW showed no significant difference in score between the treatment and control group, an equivalent range of 2–10.
In our study, the overall reduction in crusting was noted in the treatment site compared to the control site. At the end of 3 months, there was no crusting in 88%, mild crusting in 10.3% and severe crusting in 1.7% of patients in the treatment site, whereas in the control site, there was no crusting in 62.06%, mild crusting in 25.8% and severe crusting in 12.06% of patients. There is little in the literature regarding the incidence of crusting concerning the use of postoperative topical steroids. We report a statistically significant reduction in oedema in the treatment site compared to the control site. There was no oedema in 79.3%, mild oedema in 12.06% and severe oedema in 8.6% of patients in the treatment site, whereas in the control site, there was no oedema in 62.06%, mild oedema in 22.4% and severe oedema in 15.5% of patients at the end of 3-month follow-up. Our finding was in accordance with the study by Murr et al., 11 where the visual analogue rating of inflammation was statistically and clinically lower in sinuses with a steroid eluting stent from 3 to 6 weeks after surgery. Synechiae formation was the most frequently occurring complication and our primary variable in this study, ranging from 6 to 27%. 7 In our study, the incidence of synechiae was higher in the control site (17.2%) compared to the treatment site (1.72%) at the end of the follow-up period of 3 months. A survey by Côté et al. 4 showed a trend toward fewer synechiae formations in the nasal cavities receiving triamcinolone irrigation. However, Han et al., 12 in their study of 143 patients, showed a statistically significant reduction in the incidence of adhesions in patients receiving postoperative steroid-releasing sinus implants (4.2%) compared to placebo (14.1%). Murr et al. 11 also found similar results in their study of 43 patients, where significant synechiae occurred in 5.3 % of cases in the treatment group receiving postoperative steroid irrigation compared to 21.1% of patients in the control group.
A study by Vento et al., 13 which included 60 patients undergoing ESS receiving triamcinolone aerosol spray postoperatively, concluded that triamcinolone acetonide prevents the regrowth of nasal polyposis after polyp surgery in ASA-tolerant patients. Similarly, a study by Han et al. 12 showed the rate of frank polyposis by day 30 following ESS was 36.9% on control sides compared to 19.8% on treatment sides receiving steroid-releasing sinus implants (P < 0.0001), representing a 46% relative reduction. A study by Matheny et al. 14 showed similar results, where 20 patients receiving steroid eluting sinus implants following ESS in the fourth POW were evaluated for ethmoid sinus inflammation using a visual analogue scale. Mean ethmoid sinus inflammation was reduced from 25.6 at baseline to 22.6 at week 2 and 18.9 at week 4. The reduction in inflammation at week 4 was statistically significant (P = 0.03). There was also a decline in crusting; however, it was statistically insignificant. A study by Forwith et al. 15 also yielded similar results, where 50 patients following ESS received steroid eluting sinus implants and were evaluated for up to 60 days. The mean inflammation scores were minimal at all times, and polypoid tissue formation at day 30 was only 10%. In our study, the incidence of postoperative polypoidal changes on the control side (10.3%) was more than on the treatment side (5.71%). Thus, the rationale of our study was to see whether topical application of steroids via nasal irrigation would improve postoperative outcomes and minimize the systemic adverse effects, which get normalized ten days after operation. 16
The efficacy of intranasal triamcinolone acetonide in seasonal and allergic rhinitis has been evaluated in clinical trials and compared with antihistamines and other intranasal corticosteroids. Intranasal corticosteroids are either equally effective or more effective than comparative drugs. Intranasal corticosteroids are beneficial as they decrease membrane permeability and inhibit both early and late phase reactions to allergens. They minimize the nasal secretory response and reduce the sensitivity of local nasal irritant receptors. A potential benefit of topical application is the flushing action of the nasal mucosa, which may reduce allergens and secretions.17,18 Moreover, in our study, we used triamcinolone irrigation followed by packing rather than using impregnated packs, the rationale behind using intra-operative irrigation was to enhance drug delivery directly to sinuses, especially frontal and sphenoid sinuses where impregnated middle meatal packs do not reach and postoperatively irrigations are complex, this method leads to increased contact period of drug with sinus mucosa thus better absorption. In addition to seasonal and perennial rhinitis, intranasal corticosteroids have additional benefits when used to reduce inflammation in the treatment of sinusitis and may help in decreasing secondary rhinovirus infections. 19
The correction of septal deviation reduced the adverse outcomes such as synechiae on the deviation site, which would otherwise have confounded the results. Although the grading of endoscopic findings was entirely subjective, endoscopic assessment by a single person alleviated the chance of observation bias. Also, the examiner was blinded regarding which side received triamcinolone.
It should be noted that, despite statistical significance, the magnitude of the observed clinical effect was modest. In other words, differences between intervention and control groups at 8 to 12 weeks were on the order of 10%. This is nevertheless meaningful, in that 10 out of 100 patients experienced better outcomes with triamcinolone, which cannot be ignored.
To conclude, triamcinolone irrigation after bilateral endoscopic sinus surgery is an effective method. It provides good outcomes with improvement in healing and a significant reduction in oedema and polypoidal mucosal change in the sinus cavities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was taken from patients.
Ethical Approval
Ethical committee approval was taken from the AIMSR institutional committee of ethics.