
Abstract
Desmoplastic fibroblastoma (DF) is primarily a sporadic, rare, benign, soft-tissue tumor with an excellent prognosis and no reported recurrence to date. DF presents as a painless, slow-growing mass with symptoms due to its mass effect. We report a case of a middle-aged man presenting with a right supraclavicular mass and numbness of the right arm, eventually diagnosed as DF. After confirming the diagnosis with imaging and biopsy studies, the tumor was successfully excised using a transcervical approach with no complication or recurrence detected during the 2-year follow-up after surgery. A review of the relevant literature is presented regarding the presentation, diagnosis, and outcomes of published case reports of DF coinciding with those of our discussed case. This case report adds to the pool of uncommon DF cases mainly for its unique symptoms and location. It also highlights the necessity of health education related to painless masses that might be attributed as trivial in the community.
Keywords
Introduction
Desmoplastic fibroblastoma (DF), or collagenous fibroma, is a rare, fibrous soft-tissue tumor that typically arises in the subcutaneous tissue of the upper extremities. According to the WHO 2020 classification, DF belongs to the fibroblastic/myofibroblastic tumor group. 1
Desmoplastic fibroblastoma has a benign course, and its etiology remains unknown; however, preceding trauma may be a contributing factor. 2 Morphologically, DF resembles soft-tissue desmoid tumors, commonly seen in the abdominal wall.3,4 It is more common in men, with a peak incidence in the fifth through seventh decades of life. 5 DF generally manifests as a firm, slow-growing, and painless subcutaneous mass with a broad anatomic distribution. 6 Its incidence in the head and neck area, however, is uncommon, with DF in the supraclavicular region being the rarest and most challenging to treat. 4 This is primarily owing to the surrounding vital structures being confided in a relatively small space. Complete surgical excision is the recommended treatment.
Here, we report the first case of supraclavicular DF from Saudi Arabia, aiming to contribute to the data pool of this rare tumor by emphasizing its presentation, diagnosis, treatment, and outcome. As a result, this case report will aid in facilitating future guidelines for diagnostic and treatment approaches. We also reviewed pertinent literature concerning this rare tumor, focusing on those tumors that occur in the supraclavicular region and cephalad.
Case Report
A 45-year-old man with no significant medical or family history was referred to our center with a 6-month history of a neglected right neck mass. Initially, the patient was asymptomatic; with time, the mass started to cause bothersome numbness in the right arm, for which he sought physical therapy. The physiotherapist incidentally noticed the mass and instructed the patient to seek medical attention. Further questioning revealed no history of trauma or any other sensory deficit. Physical examination of the neck showed a supraclavicular mass that is firm, immobile, and non-tender to palpation. It measured around 4 × 3 cm. Apart from the patient’s complaint, the neurological examination was intact.
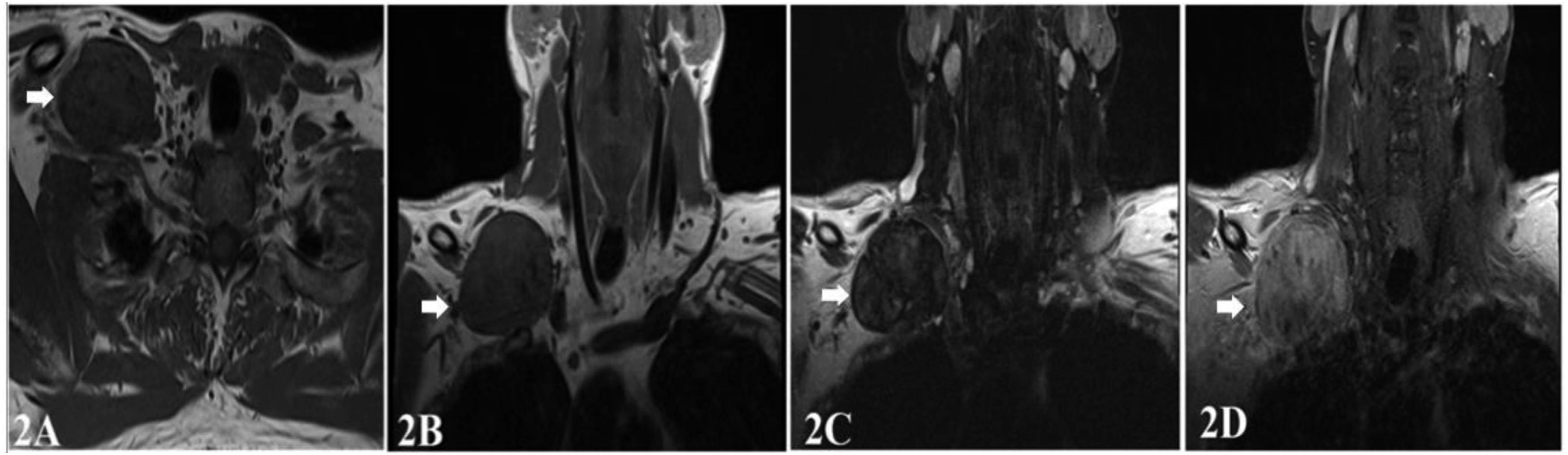
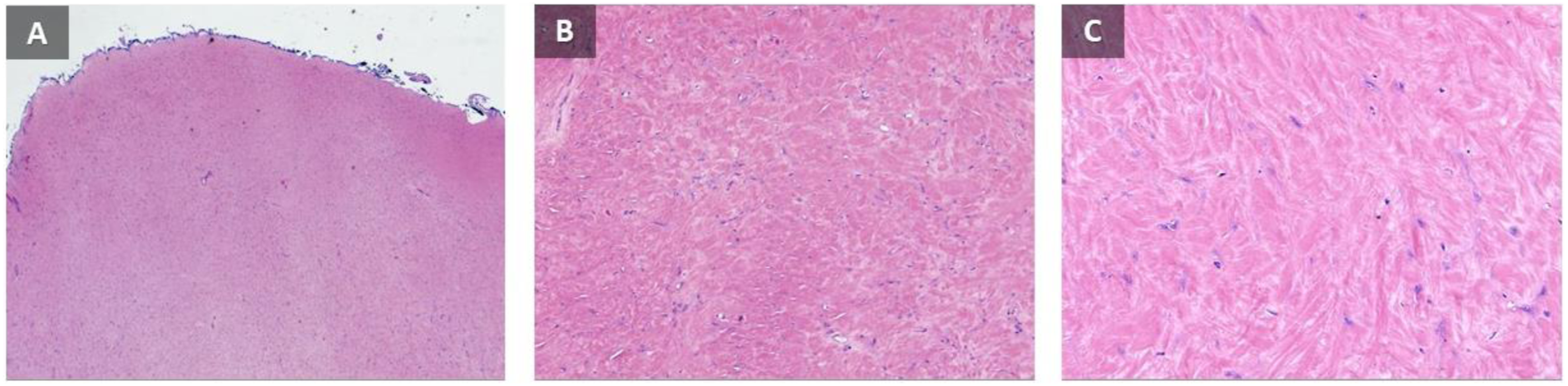
Computed tomography (CT) with contrast showed a well-defined, 5.4 × 3.5 × 5.4-cm mass in the right supraclavicular region. The mass was isodense to the surrounding muscles with poor heterogeneous enhancement. It was compressing the surrounding vessels and nerves without any signs of invasion (Figure 1A‐1B). On contrast magnetic resonance imaging (MRI), the mass was isointense to hypointense to the surrounding muscles on both T1 and T2 imaging with minimal enhancement (Figure 2A–2D). The decision of core needle biopsy was made, and histopathology revealed spindle-cell fibroblastic proliferation on a myxoid/collagenized background with no evidence of significant mitotic activity or tumor necrosis compatible with DF (Figure 3). Computed tomography of the neck (A; axial and B; coronal views) showing a right supraclavicular well-defined large mass (arrows) that is isodense to surrounding muscles with poor heterogeneous enhancement. Magnetic resonance imaging of the neck (A; T1, axial view, B; T1, coronal view, C; T2 coronal view, D; T1 coronal view with contrast) showing a supraclavicular mass (arrows) isointense to surrounding muscles on T1, with heterogeneous enhancement on the contrasted image. Low power (A), intermediate power (B), and high power (C) magnification depicting stellate and spindle neoplastic cells with prominent collagen in the background with bland spindle fibroblastic cells with no significant nuclear pleomorphism, mitotic activity, and necrosis.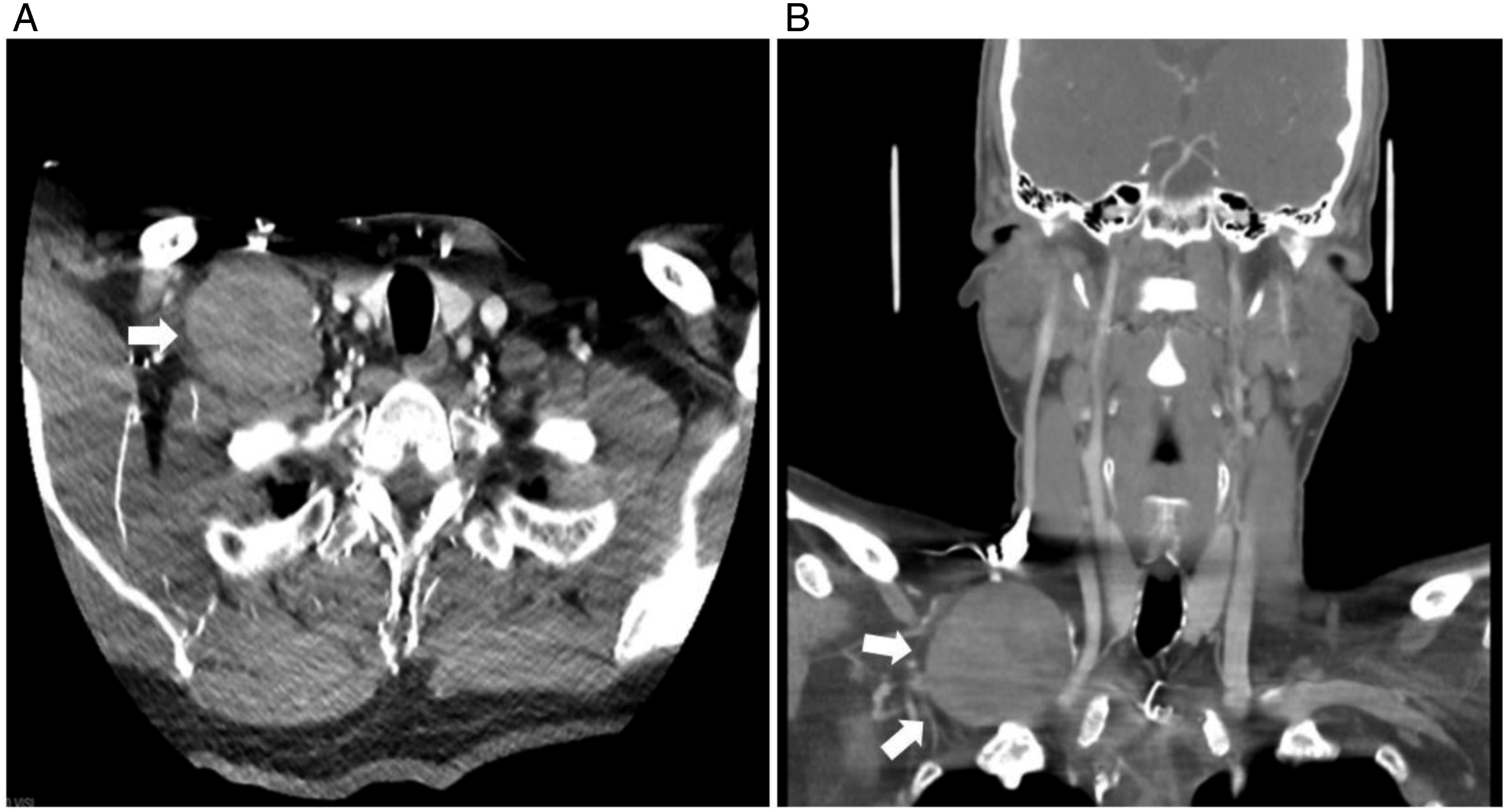
Subsequently, surgical excision of the mass under general anesthesia was recommended. The tumor was excised using a transcervical approach after dissecting it off from the clavicle and surrounding major vessels and nerves. Finally, the drain was placed along the incision line, and closure was done in two layers. The patient was sent for recovery without complications, and the drain was removed on postoperative day 1, with marked improvement in his neurological symptoms. The patient was discharged with no complaints. During 2 years of regular follow-up, numbness disappeared without signs of recurrent or residual disease.
Discussion
DF is an uncommon benign soft-tissue tumor first introduced by Evans. 7 Nielsen et al. 8 renamed it as “collagenous fibroma” for a better description of its histological features and reflection of its favorable prognosis. DF may develop without any history of trauma or inciting event, 9 as was the case of our patient. This, in part, lends credence to the hypothesis that this tumor is indeed the result of a neoplastic process. 9
DF mostly affect adult men with manifestations depending on the tumor size and location. 10 It may be asymptomatic or have nonspecific symptoms 11 like local pain and tingling, as was the case of our patient.
Diagnosing DF often requires multiple diagnostic modalities such as radiology (both CT and MRI) and biopsy with histopathology. Radiological investigations allow characterization of the mass and provide information about its location, dimensions, and adjacent vital structures and help rule out invasion. Radiology also helps during treatment planning. MRI is superior to CT with regard to characterization and extent definition of DF, with MRI revealing a well-defined mass surrounded by condensed connective tissue and a notable low-signal intensity on all pulse sequences.6,12 To suspect DF on radiological investigations, one must become familiar with its key imaging features. Nakayama et al. 6 suggested that the enhancement pattern on contrast-enhanced MRI and the presence of a low-signal-intensity band may be employed as distinguishable features similar to those found in our case (Figure 2D). The radiological findings of DF are nonspecific and may yield only a presumptive diagnosis. Radiological differential diagnoses of DF include desmoid tumor, neurofibroma, fibromatosis, and elastofibroma. Histopathological examination of tissue obtained through incisional biopsy is a valuable method to differentiate DF from other soft-tissue tumors, mainly desmoid-type fibromatosis (which requires more intensive treatment).2,6 DF presents histologically as a hypocellular lesion consisting of spindle to stellate-shaped cells embedded in a dense collagenous or myxocollagenous stroma. 6 Nevertheless, with this many differentials at hand, a diagnostic dilemma might arise. Therefore, the addition of immunohistochemistry and cytogenetics to the workup can mitigate the similarity between DF and other mimics. FOSL1 immunostaining and a t(2;11)(q31;q12) translocation are both features that have been shown to be helpful in the diagnosis of DF. 6
Review of All Reported Cases of Desmoplastic Fibroblastoma in the Supraclavicular Region and Cephalad Have Been Published in English Between 2012 and 2022.
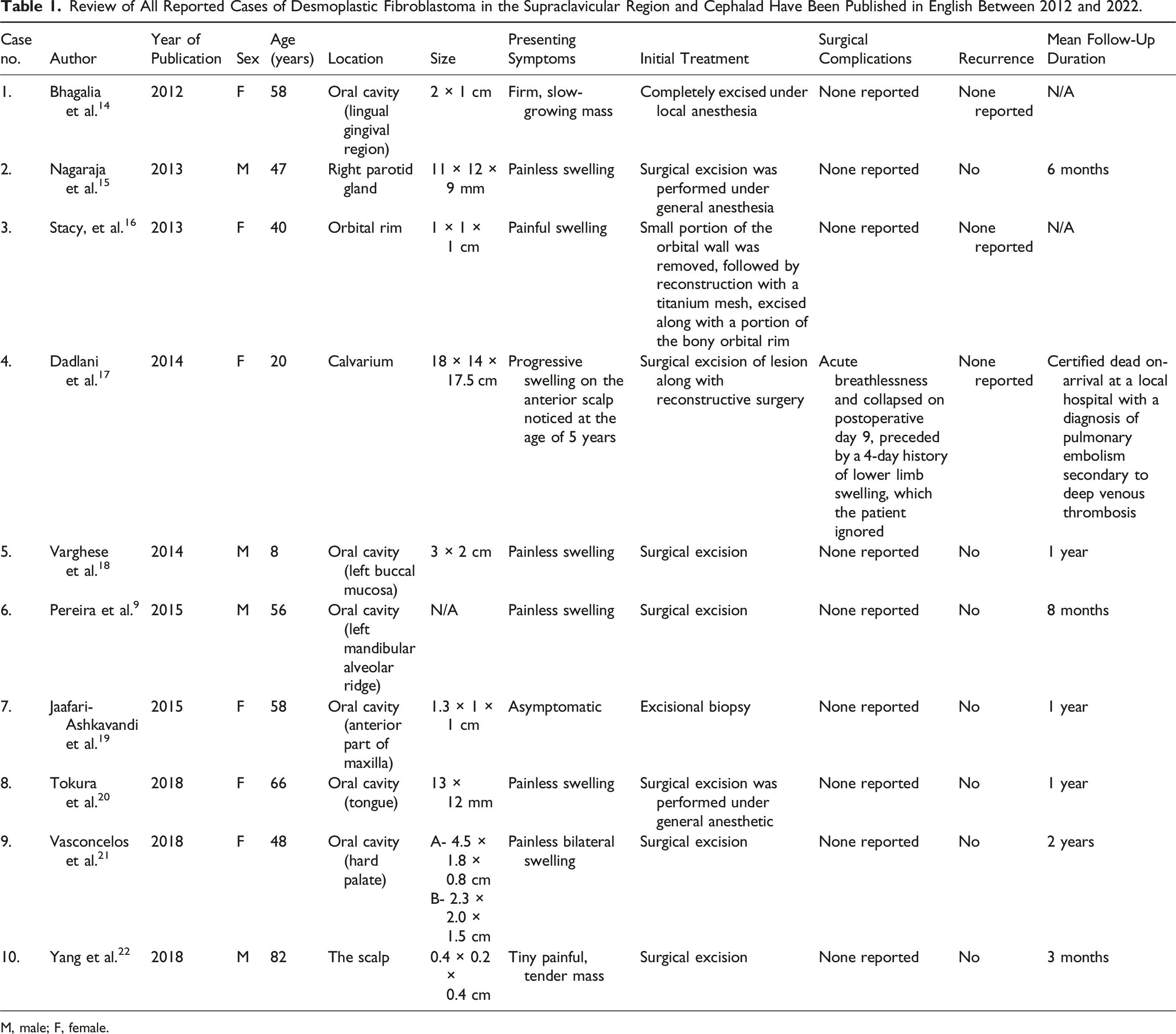
M, male; F, female.
Radiological Findings of Reported Cases of Desmoplastic Fibroblastoma in the Supraclavicular Region and Cephalad.
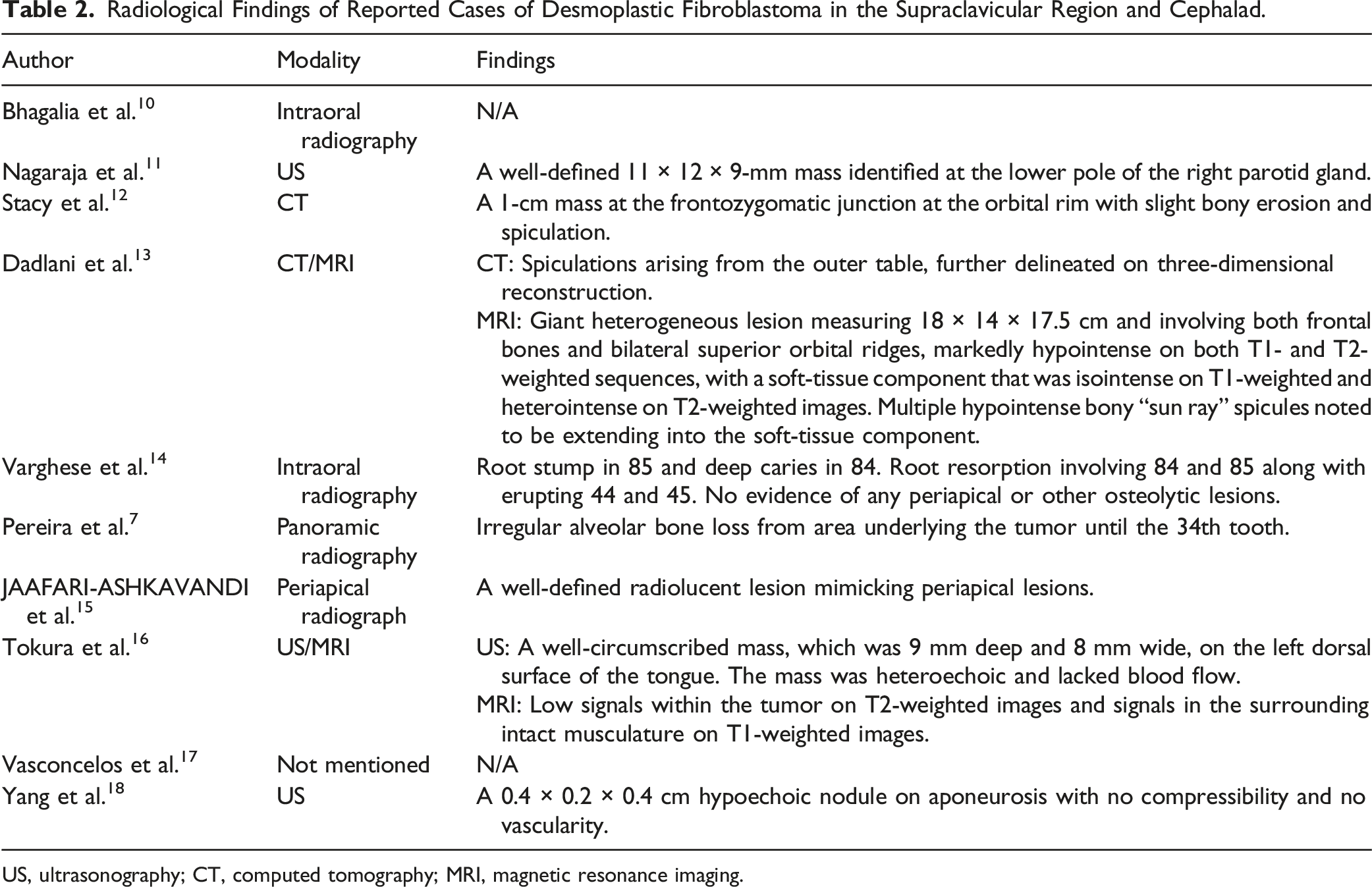
US, ultrasonography; CT, computed tomography; MRI, magnetic resonance imaging.
Total surgical excision remains the definitive and recommended treatment approach, with an excellent prognosis and no reports of local recurrence. 19 These findings highlight the importance of health education in the community to raise awareness about painless masses to facilitate early detection, thereby avoiding possible impediments in providing optimal treatment. Since this tumor’s main manifestation is painless swelling that may be left untended until the emergence of symptoms. It also highlights that a rare disease like DF, with many possible differentials, needs other confirmatory tests, so they are not missed.
Conclusion
DF is a rare, indolent, benign soft-tissue tumor. The diagnosis of DF requires a high level of suspicion owing to its rarity and lack of specificity of clinical and radiological findings. The presented case further braces the clinical and surgical evaluation of DF. Histopathological examination is indispensable for an accurate diagnosis. The definitive treatment is total surgical excision with an excellent prognosis and no reported instances of recurrence. Long-term postoperative monitoring would be prudent while avoiding extensive surgical treatment or radiotherapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Data Availability
The data used to support the findings of this study are included within the article.