
Abstract
Condylar neck fractures are common injuries that occur in the facial and mandibular regions. The proximity of this area to the vital neurovasculature creates the increased importance of proper surgical intervention to limit damage to the underlying structures. Here, we report a case of a condylar neck fracture that resulted in temporary paresis of the facial nerve. In addition, a review of the literature regarding condylar fracture treatment and its complications was conducted.
Introduction
Condylar neck fractures are common injuries that occur and require mandibular reconstruction by maxillofacial surgeons. The location of these fractures can expose vital structures to injury during the trauma or the reconstructive repair. Thus, it is important to consider these sensitive structures when considering treatment modalities. We now report a case of a 39-year-old female who developed temporary facial paresis after mandibular reconstruction surgery. In addition, a review of the literature regarding condylar repair treatments and their complications was performed.
Case Report
A 39-year-old female presented with bilateral condylar, parasymphaseal, and nasal bone fractures that occurred from a fall due to her poorly controlled seizure disorder. The patient had a history of alcohol abuse and was an active cigarette smoker.
CT imaging revealed an acute comminuted fracture of the left parasymphaseal mandible with bilateral condylar neck fractures and dislocated TMJs (Figure 1). The patient had a significant open bite deformity with dysphagia. After discussion with the patient and consideration of her comorbidities, the initial repair was performed by plating the parasymphaseal fracture, with maxillomandibular fixation (MMF) with elastics for her bilateral condylar fractures, due to concern for her active seizure disorder. The patient did not tolerate the MMF with elastics, and self- removed her arch bars. Consequently, the potential options for the patient included observation, revision MMF with elastics, or open reduction internal fixation with or without MMF. The patient elected for open reduction internal fixation. CT scan with a 3D reconstruction of an acute comminuted fracture of the left parasymphyseal mandible with bilateral condylar neck fractures and dislocated TMJs.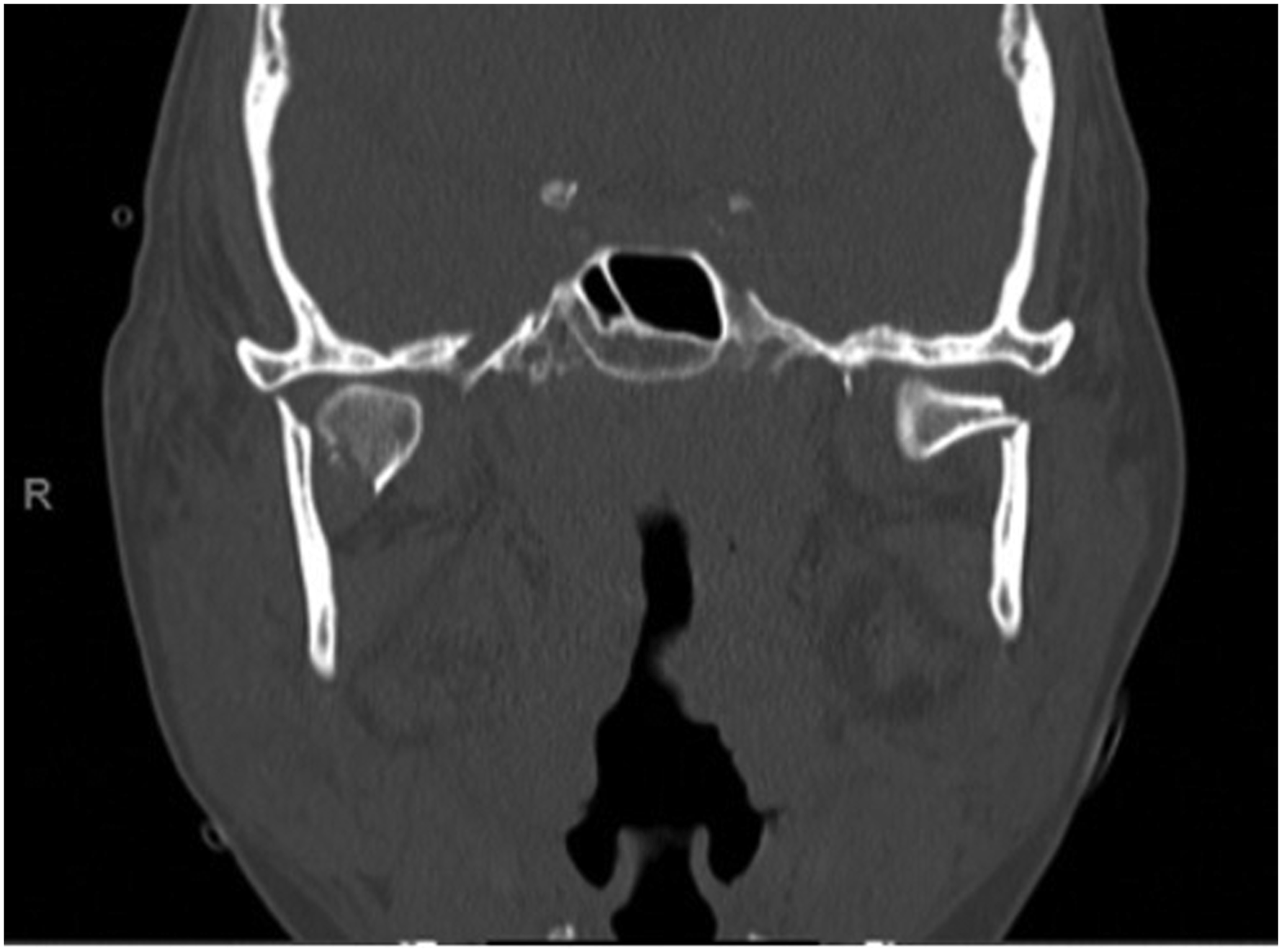
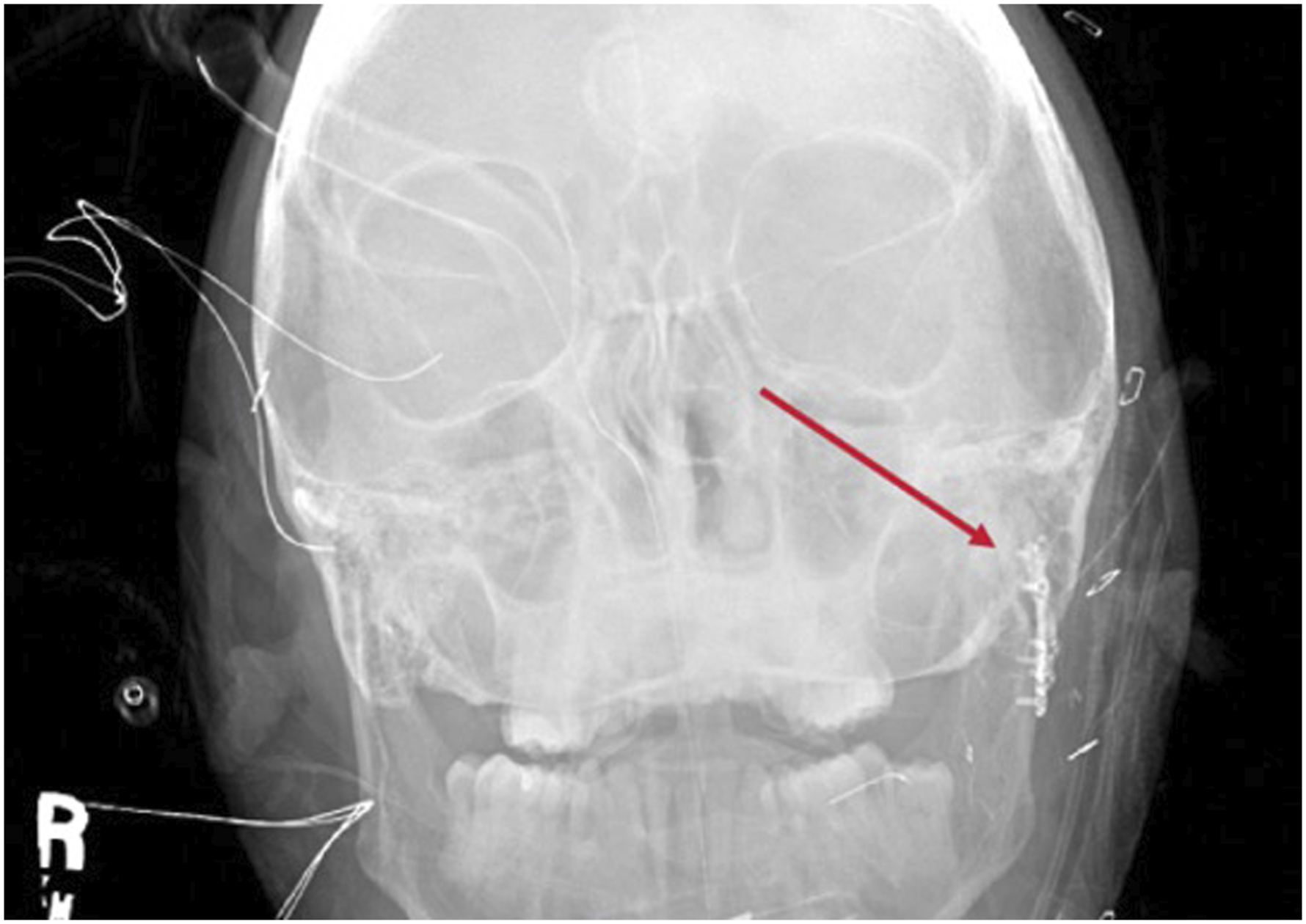
During the surgery, no long-acting paralysis was used, and facial nerve monitoring was performed. A modified Blair approach was designed, and the lower division of the facial nerve was identified and traced proximally. The pterygomasseteric sling was incised, the masseter muscle was released, and the external carotid was ligated distally for more exposure. Once the fracture was exposed, the patient was paralyzed to help with reduction, and a 2-plate fixation was done in the sub-condylar region (Figures 2 and 3). The pterygoid muscles in the region were pulling on the condylar head medially, requiring a significant reduction force in the area. 2-plate fixation in the sub-condylar region. Reduction and 2-plate fixation in the sub-condylar region.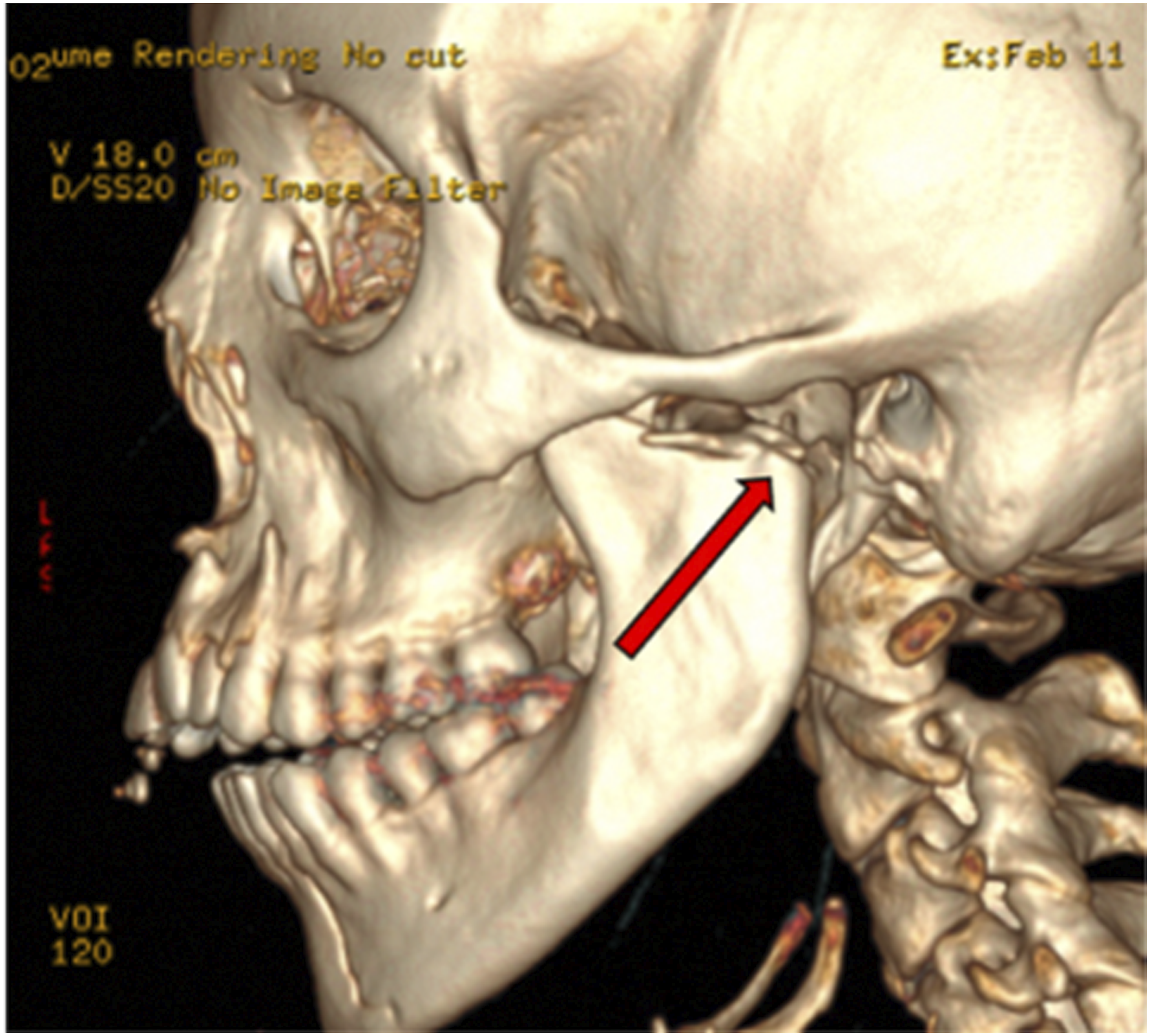
In the postoperative period, the patient had no obvious appreciable movement in both the upper and lower division, with a House-Brackmann score (HB)VI /VI. The decision for clinical observation for 72 hours with nerve testing was made because of her HB VI status and visualization of the facial nerve during surgery. The patient was given a course of decadron, nimodipine, and eye care with an option to reexplore if there was no nerve activity in 72 hours. At the bedside, a maximal nerve stimulation test was conducted with a Hilger monitor, which was positive for facial movement in all branches on the affected side. At that point, the patient was discharged with a moisture chamber and eye care. Due to poor patient compliance and issues with transportation and finances, only one postoperative visit was conducted. At the 2-month follow-up, the patient recovered to an HB II (mid marginal mandibular weakness) and was able to tolerate a soft diet.
Discussion
Condylar fractures are common injuries that account for 11–16% of facial fractures and 30–40% of mandibular fractures. 1 These injuries require careful management due to the proximity of the facial nerve and temporomandibular joint (TMJ). According to the AO, management of condylar fractures can be treated with observation, maxillomandibular fixation (MMF), or 1- or 2-plate open reduction internal fixation (ORIF).
The ORIF allows for direct visualization and anatomic reduction of complex condylar fractures. According to Bayat et al., ORIF has the advantage of showing better functional results in complex fractures by allowing for the immediate movement of the mandible, which lowers the risk of ankylosis. 1 Literature has shown that the ORIF procedure can have potential complications, particularly affecting the facial nerve. The location of the facial nerve within the vulnerable area of the periosteum and superficial fascia makes it highly susceptible to surgical-related damage. 2 According to Asim et al., facial nerve paresis was noted in 31% of cases of condylar fracture repairs, with 69.2% of patients experiencing transient symptoms that resolved within eight weeks of the procedure. 3
During the dissection of the condylar region, a nerve stimulator may be used to identify and protect the facial nerve. Muscle relaxation can interfere with nerve stimulator use, though it may aid in fracture reduction.4,5 To limit the risk of nerve transection, we used the Blair incision to aid in better recognition of the nerve intraoperatively, limiting the risk of transecting the facial nerve since it was identifiable. Contrastingly, a more limited excision may have prompted a return to the operating room immediately for better exploration of the region due to a higher chance of nerve transection. If there is a concern of nerve transection, a nerve conduction study (NCS) can be employed immediately as an initial screening test to check for nerve conduction block and to identify the margins of the damaged nerve segment. 6 Any strong suspicion of nerve transection should be explored operatively immediately. Incomplete nerve injuries can be re-checked with nerve testing 72 hours after the injury to allow for Wallerian degeneration. 7
Conclusion
There are multiple approaches to treating condylar fractures, each with advantages and disadvantages. Choosing the proper treatment modality for condylar fractures is crucial to optimizing patient functional outcomes. The ORIF procedure has been shown to create better functional results and visualization in condylar fractures; however, it increases the potential for injury of the facial nerve.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.