
Abstract
Condylar fractures are the most common mandibular fractures, and a variety of open and closed approaches are used for repair, each with its own inherent risks and benefits. A 27-year-old man had a severely displaced and angulated high subcondylar fracture with anterior open bite deformity. The patient underwent open reduction and internal fixation of the condyle via a combined preauricular and intraoral approach as well as maxillomandibular fixation to repair his fracture. This combined approach allows the surgeon to maximize exposure while limiting risks of permanent injury from surgery.
Introduction
The condyle is the most common site of mandibular fractures, making up approximately 20% of all mandibular fractures. 1 Minimally displaced fractures may be treated non-operatively, although when occlusion is poor, condylar fractures are often treated with a closed approach, that is, with maxillomandibular fixation, which allows for restoration of occlusion without necessarily leading to fracture reduction. 2 However, newer data suggest that in the case of significant displacement, angulation, or ramus shortening, open repair may lead to improved functional results. 3 We present here a case where a combined approach was used for improved access to a high condylar fracture.
Case Report
A 27-year-old male suffered a ground level fall and was found to have a severely displaced subcondylar fracture. The patient had initially presented to an outside hospital emergency department, where imaging was obtained. The initial read was negative for fracture; however, in reviewing the scan, the emergency physician recognized a mandibular fracture. By the time the patient followed up at our hospital system, it had been 10 days since his injury. He was noted to have poor occlusion with an anterior open bite deformity and review of his outside imaging demonstrated significant angulation and displacement of the condylar head, with the condyle completely medially displaced out of the glenoid fossa (Figure 1). Given the severe displacement, it was recommended he undergo surgical repair of his fracture. Good reduction could not be obtained closed; therefore, an open approach was pursued. An intraoral incision was used to gain initial access the mandible and locate the fracture line; however, given the high location of the fracture, an intraoral approach alone was not sufficient to obtain satisfactory exposure. By the time the patient was brought to the operating room, it had been 12 days since his injury and he was outside of the optimal treatment window. Likely secondary to his initial delay in diagnoses, there was significant scarring of the condylar head to the surrounding soft tissues, which made the operation much more challenging. Additionally, the condylar head had been medially displaced completely out of the fossa, and additional exposure was needed to properly reduce it. This could not be achieved with a purely intraoral approach alone, and therefore, a combined approach was used. A preauricular approach via facelift incision was used to better expose the fracture. Since the fracture had been visualized on the intraoral side, a retractor could be placed intraorally at the fracture line so that the preauricular side could be tunneled directly to the fracture to optimize exposure while minimizing risk to the facial nerve. The tunnels were connected high through blunt dissection at the level of the superior crus of the helix to minimize risk of injury to the nerve. Good reduction was achieved, and the fracture was plated with a titanium miniplate (Figure 2). Postoperatively, the patient was noted to have a paresis of the frontalis in the post-anesthesia care unit (PACU). The patient was discharged with a course of steroids to decrease inflammation of the surgical bed. The paresis progressed over the next 24 hours to paralysis of the ipsilateral frontalis and corrugator and a House-Brackmann 4/6 paresis of the lower lid. Due to the progressive nature of the paralysis it was felt that a neuropraxia was the most likely etiology. With a shortened ramus from the severe displacement of the condylar head, the facial nerve trunk was pulled higher with the surrounding soft tissues of the parotid. Reduction required significant inferior displacement of the mandible, likely leading to the overstretch injury to the nerve. Other potential etiologies would include incision, crush, compression and thermal injury. Postoperatively, botulinum toxin was injected into the contralateral frontalis and corrugators to restore facial symmetry while waiting for the ipsilateral nerve to recover. By 3 months postoperatively, facial nerve function was completely restored with House-Brackmann grade 1/6 movement bilaterally and the patient remained in good occlusion with 3 finger breadth mouth opening.
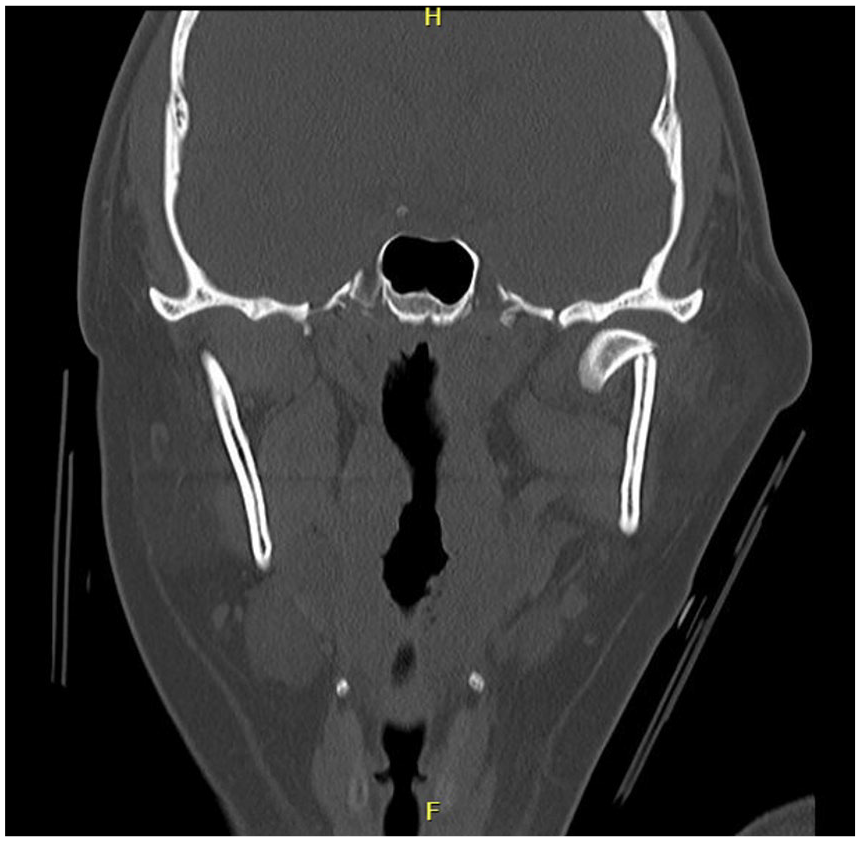
Preoperative coronal view of computed tomography scan of the mandible demonstrating condylar fracture with severe displacement and angulation.
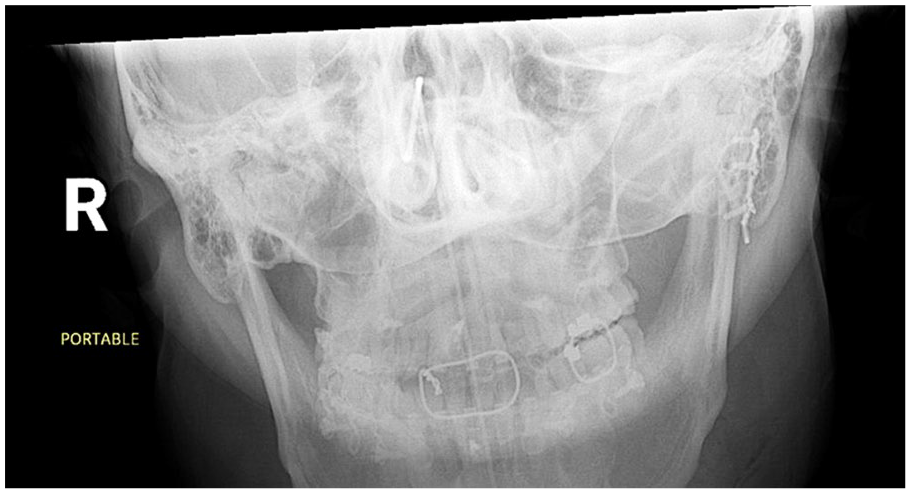
Postoperative X-ray of the mandible demonstrating reduction of the condylar segment with good dental occlusion.
Discussion
Historically, the indications for open reduction and internal fixation (ORIF) include displacement of the condyle into the middle cranial fossa, lateral displacement of the condyle, foreign body, or failure of closed reduction to achieve good occlusion. 4 However, as data have emerged suggesting that open repair may lead to improved occlusion, decreased trismus, and even improved quality of life, 3 ORIF has become more common in treating condylar fractures. When open repair is performed, there are various surgical approaches to the condyle. An intraoral approach avoids visible scars and the risk of damage to the facial nerve, but access to high condylar fractures may be difficult or impossible. An endoscopic-assisted intraoral approach may be used to improve visibility but accessibility to higher fractures remains difficult, and specialized equipment is needed. Extraoral approaches, including preauricular, retromandibular, and submandibular approaches, may improve exposure but risk damage to the facial nerve and visible scarring. In general, these approaches are selected based on the location of the fracture. A preauricular approach would typically be chosen for higher fractures, for example, of the condylar head or upper neck, a retromandibular approach can be considered for condylar neck and base fractures, and the submandibular approach may be used for lower condylar fractures. 5 As in this case, if an intraoral approach alone is unable to adequately expose the fracture, a combined intraoral and extraoral approach may be selected. This may be especially advantageous in cases such as these with significant scarring or severe displacement, when achieving good reduction would be challenging or impossible without enhanced exposure of the fracture. In addition, localizing the fracture line on the intraoral side and then tunneling directly to the known location of the fracture limits the amount of dissection that must be done through the parotid and, therefore, decreases the likelihood of complications like facial nerve palsy or sialocele. Those cases with significant loss of ramus height may be particularly at risk for facial nerve injury due to the uncertain location of the facial nerve trunk in setting where the surrounding soft tissues have been cephalically translocated. In the case of a high condylar fracture, a combined intraoral and preauricular approach may be used to more quickly and safely access the upper condyle while optimizing exposure.
Footnotes
Acknowledgements
Not applicable.
Consent to Participate
Written informed consent was obtained from the patient for the publication of this work.
Consent for Publication
Written informed consent was obtained from the patient for the publication of anonymized data and any accompanying images.
Data Availability Statement
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.