
Abstract
Augmentation rhinoplasty using alloplastic materials is a relatively standard procedure in Asian patients. Expanded polytetrafluoroethylene (ePTFE) is one of the commonly used alloplastic materials because it has a high biocompatibility and is easy to handle. Recently, a patient who had previously undergone augmentation rhinoplasty using ePTFE as the implant material visited our clinic. She had the implant material surgically removed after three years and visited our clinic with a nasal dorsal hump. The patient underwent revision rhinoplasty at our institution. Unexpectedly, we found some ePTFE material that was not identified on the preoperative X-rays. After removing the ePTFE material, the nasal dorsal hump was corrected, and we did not need to perform a nasal dorsal hump reduction.
Introduction
Compared with Caucasians, augmentation rhinoplasty using alloplastic materials is one of the most common procedures in Asian patients. 1 Several types of alloplastic materials have been introduced, such as silicone, expanded polytetrafluoroethylene (ePTFE), and MEDPOR. 2 Among them, ePTFE has been commonly used for dorsal augmentation due to its high biocompatibility and easy manipulation. 3 Recently, we had a patient who underwent augmentation rhinoplasty using ePTFE as the implant material and had the implant material removed 5 years ago. The patient told us that all the implant material that was previously inserted was removed. However, we found part of the previously inserted ePTFE that was not identified in the preoperative X-rays, resulting in a nasal dorsal hump-like appearance. This report describes our experience and shares the lessons we learned from this case.
Case presentation
A 36-year-old woman visited our clinic with dissatisfaction with their external nasal contour. The patient, eight years previously, had undergone augmentation rhinoplasty using ePTFE as the implant material, septal extension graft using septal cartilage, lateral osteotomy, and alar reduction using an open approach. The patient told us that the ePTFE implant material was removed five years ago because the implant material had translocated. The patient did not have any medical or trauma history. During the physical examination, we identified asymmetry of the nostrils, columella deviation, a short nose, and a dorsal hump. The patient told us that she had visited other clinics prior to visiting our clinic and was told that she needed a nasal dorsal jump reduction. On the lateral X-ray, a dorsal hump-like lesion was observed (Figure 1). On lateral view of X-ray, no definite implant material is identified.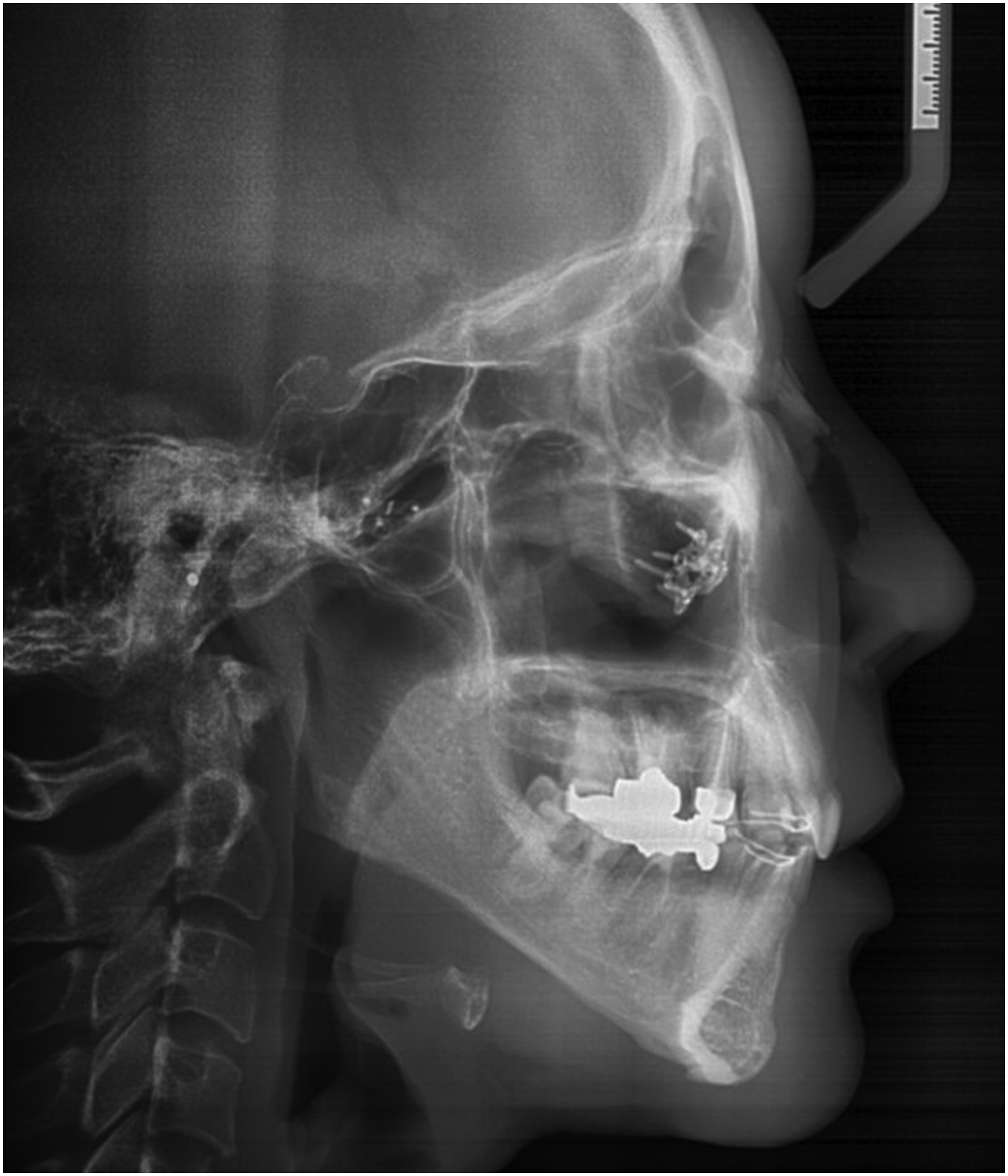
We decided to perform a revision rhinoplasty, including derotation to correct the short nose, placing a columella strut using a conchal cartilage graft, and hump removal with dorsal augmentation. After performing bilateral alar marginal and inverted “V” transcolumellar incisions, we unexpectedly found part of the previously inserted ePTFE in the supra-perichondral layer of the upper lateral cartilage (Figure 2A and B). Since it was not only located on the nasal dorsum, we suggested that it had translocated into the level of upper lateral cartilage and induced the hump-like appearance. The removal of the implant material corrected the dorsal hump. The derotation and placement of the columella strut were performed without the nasal dorsal hump reduction. The short nose and dorsal hump-like structure were corrected, and the patient was satisfied with the surgical outcome six months after the surgery. A. After bilateral alar marginal and inverted “V” transcolumellar incisions, the remnant part of previously inserted ePTFE implant was observed on the upper lateral cartilage. B. The removed part of ePTFE implant material.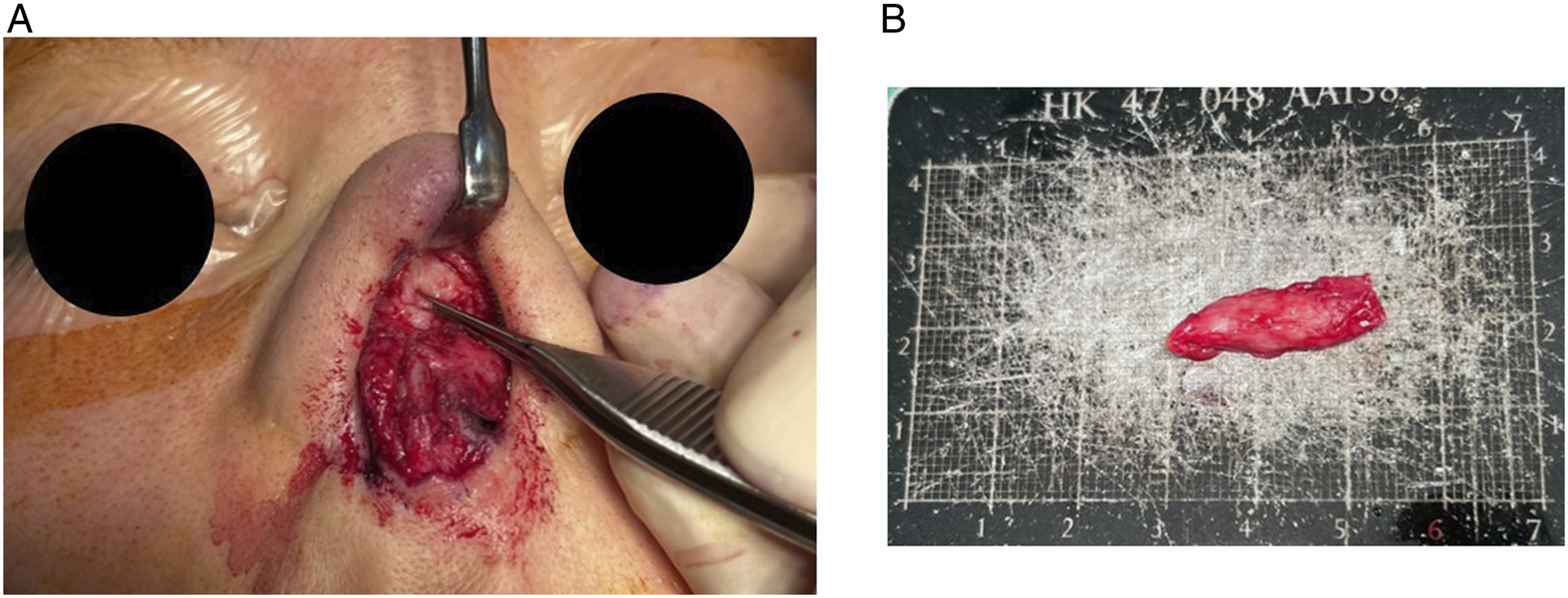
Discussion
The imaging characteristics of ePTFE are known to have a higher attenuation relative to soft tissue but have less attenuation than bone on a computed tomography (CT) and be hypointense compared to fat on a T1-weighted and T2-weighted magnetic resonance images (MRI). 2 ePTFE can present as an elongated hypoechoic halo on ultrasonography (US) images. 4 However, ePTFE cannot be identified on simple X-rays, like in our case. Therefore, we suggest that active imaging studies should be performed on patients who had previously undergone a dorsal augmentation rhinoplasty with ePTFE. If surgeons do not recognize the presence of alloplastic implant materials left in the patient’s nose, it could affect surgical procedures and result in the need for additional autologous or alloplastic material usage.
As previously reported, the advantages of ePTFE are that it is well tolerated, has lower complication rates, and allows for easy removal if necessary. 5 Our patient had undergone a rhinoplasty using ePTFE eight years prior and had the ePTFE removed five years ago because it had translocated. She had no other complications, such as infection. We found that some of the ePTFE which was previously inserted remained after the removal. Although it has been reported that ePTFE is easy to handle and remove, all surgeons should keep in mind that some implanted material could remain after removal. The risk of implanted materials remaining after the removal and possibilities of subsequent surgeries should be explained to patients before removal. During revision rhinoplasty, the usage of autologous materials is recommended to reduce infections; however, additional options for autologous implant material, such as conchal or rib cartilage, after removing the initial implant material should be evaluated.
ePTFE is a polymer consisting of monomeric units with two carbon atoms doubly bonded, and each monomer has two fluorine moieties. ePTFE is known to be resistant to degradation and dislocation since there are no known human enzymes capable of cleaving the bonds between carbon and fluorine. 4 However, our patient experienced a complication with ePTFE resulting in the dislocation of the implanted material, and this was the reason for the removal of the ePTFE implant before visiting our clinic. The possibility of dislocation should be kept in mind for all types of implant material and proper dissection of the surgical plane, and insertion of the implant material into the proper plane should be performed.
Based on this case, we reviewed the imaging characteristics of ePTFE and suggested that active imaging study, which is more than simple X-ray, should be performed before revision rhinoplasties to identify if any ePTFE material was inserted or remained from previous operations. The possibility of remnant alloplastic material should always be kept in mind even if the medical records state that the previously inserted implant material was removed. Considering the possibility of remnant implant materials in current nasal contours and other augmentation, surgeries should be made prior to surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical/consent statement
Written informed consent was obtained from the patient.
Data availability
The datasets generated or analyzed during this current study are not publicly available due to the patient’s privacy; however, they are available from the corresponding author with a reasonable request.