
Abstract
Mediastinal emphysema is an extremely rare and potentially fatal complication of endoscopic sinus surgery. The case presented involves a 73-year-old man who developed mediastinal emphysema following endoscopic sinus surgery for severe sinonasal polyposis. We describe the multiple etiologies that may have contributed to his condition including possible microtrauma at the time of intubation or during intubation, microfracture of the orbital wall/lamina papyracea, and severe hiccups.
Introduction
Functional endoscopic sinus surgery (FESS) is a very common, minimally invasive procedure performed routinely performed to restore normal sinus ventilation and function.1,2 Emphysema is an uncommon complication of FESS, and when present, is frequently periorbital and less often mediastinal. 3 The development of post-operative subcutaneous emphysema is most commonly related to tracheal/ laryngeal trauma at the time of intubation or manipulation of the head and neck at any point during the procedure while the patient is still intubated. 4 Mediastinal emphysema, specifically, may lead to a dangerous sequalae that may result in mediastinitis, septicemia, and even death. 5 Because of this, its prompt recognition and treatment is necessary to reduce patient morbidity and mortality.
Case Report
The case involved a 73-year-old male who presented at the tertiary center outpatient’s clinic with a long-term history of chronic rhinosinusitis, severe sinonasal polyposis, and nasal obstruction with anosmia. Preoperative images showed complete opacification of all sinuses and a deviated septum. Nasal endoscopy confirmed massive polyposis. The patient subsequently underwent FESS and septoplasty. The intubation, surgery, and extubation were uneventful, and the patient was discharged home on the same day. On post-operative day one, he developed persistent hiccups which lasted for 48 hours. On post-operative day three, the patient reached out to the office and was promptly seen. At the time of evaluation, his hiccups had spontaneously resolved. Additionally, he was afebrile and tolerating a regular diet since the day of surgery. On examination, the patient was found to have significant edema over the lower right eyelid (Figure 1a). He was also noted to have evidence of periorbital subcutaneous emphysema with crepitus extending downward and symmetrically to the face, neck and supraclavicular regions. His vision and extraocular movements were intact bilaterally. Three-day post-op photo (right) and 2-week post-op photo (left).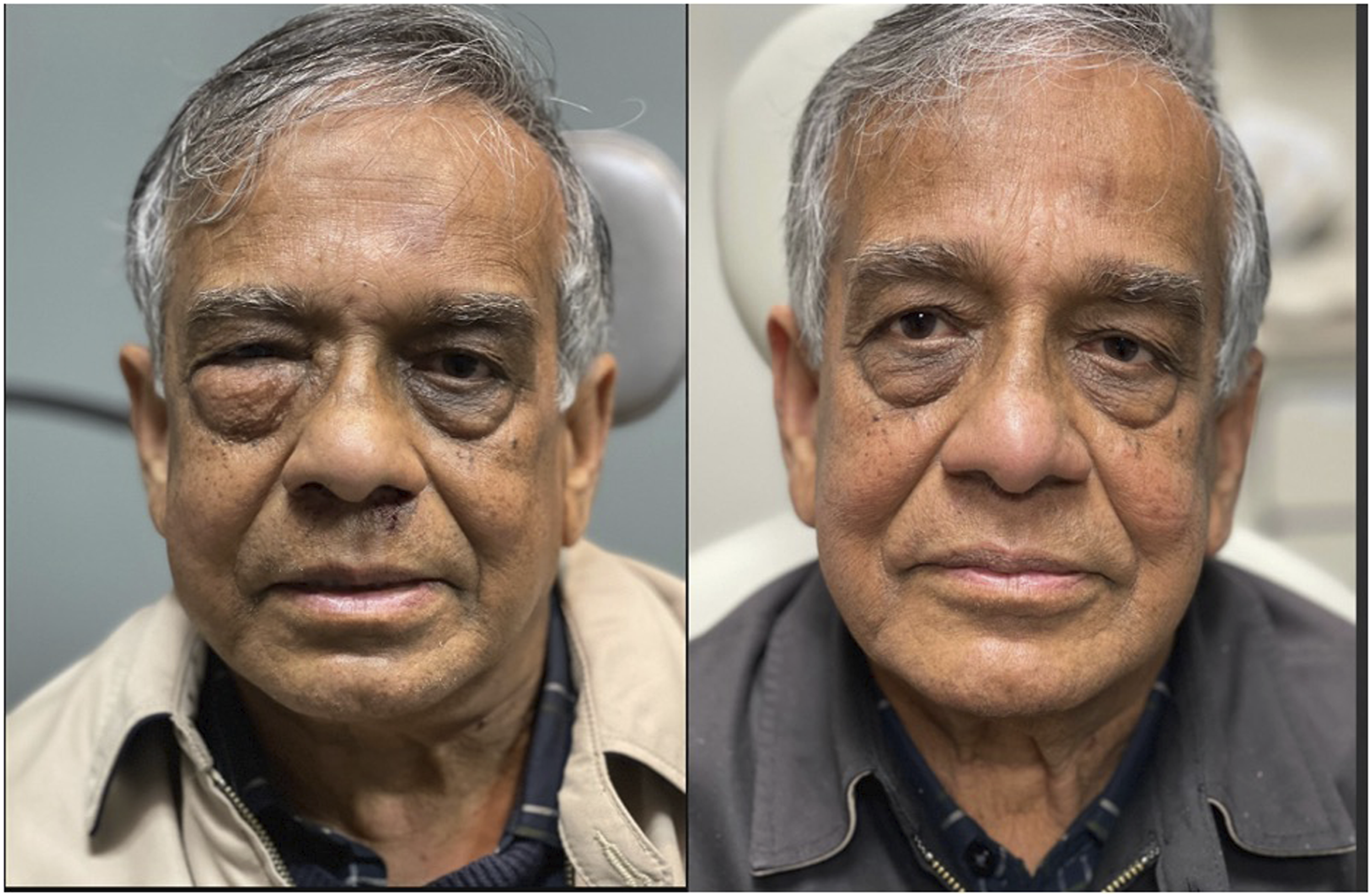
The patient was admitted for further diagnostic workup and observation. CT scan of his sinuses showed periorbital air and subcutaneous emphysema tracking to bilateral face and neck soft tissue (Figure 2). CT of the neck and chest showed bilateral subcutaneous emphysema in soft tissue of the neck and anterior mediastinum without evidence of esophageal or tracheal perforation. The patient was examined with flexible endoscopy which visualized a normal oropharynx, as well as normal supraglottic and glottic structures without any evidence of trauma or perforation. Post-op CT sinus without contrast showing emphysematous changes on the right.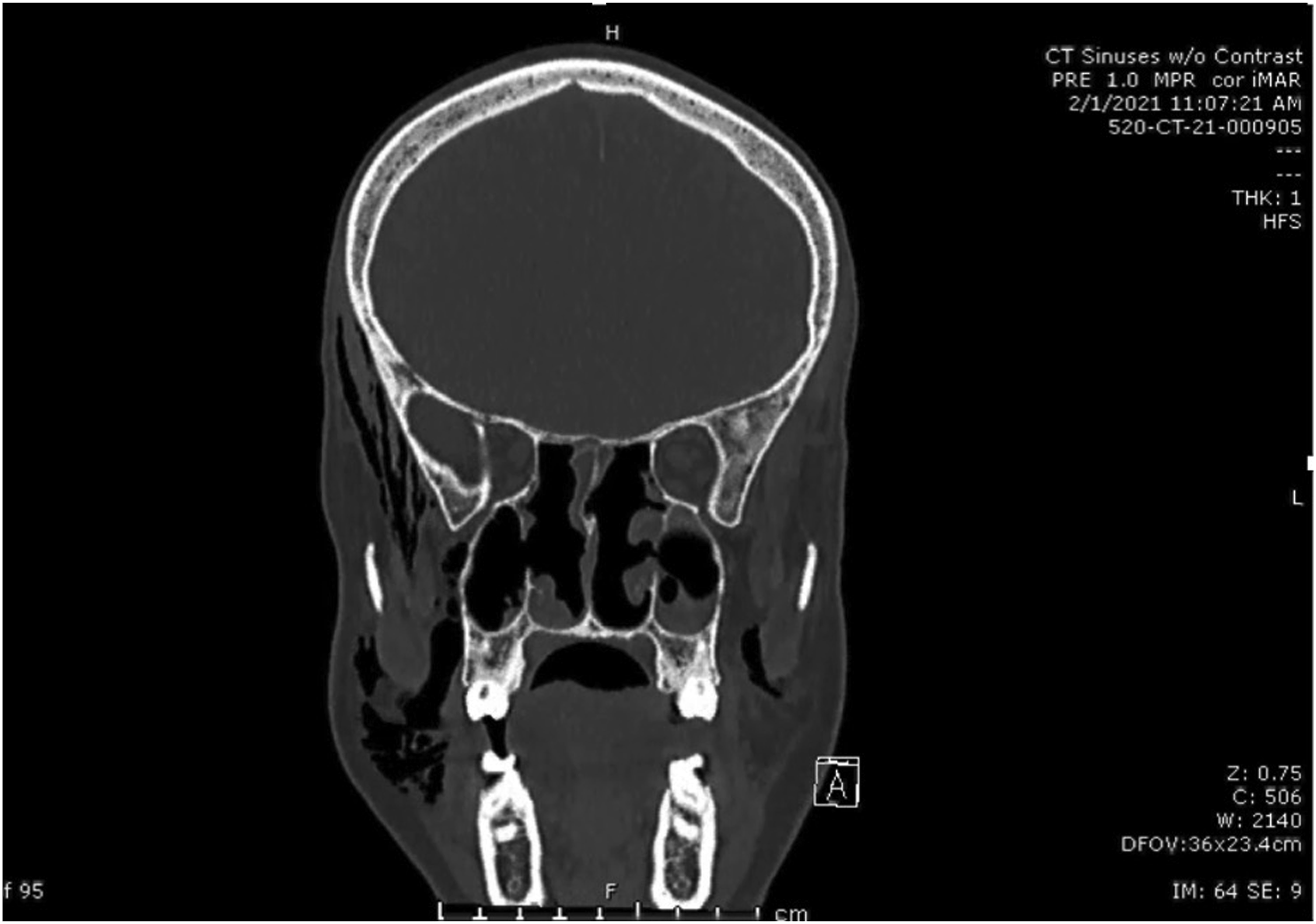
He remained afebrile with no of leukocytosis on blood work. He was subsequently observed for two days, and after an unremarkable hospital course, he was discharged home on oral antibiotics. Two weeks later, his symptoms spontaneously resolved. The patient was asymptomatic with an unremarkable physical exam (Figure 1b). Repeat CT imaging confirmed that the emphysema had resolved.
Discussion
The development of mediastinal emphysema following FESS remains as a very rare complication of this type of surgery with only few cases reported in the literature. The etiology is most often found to be trauma secondary to intubation and anesthesia, or trauma to the lamina papyracea.5-7 In the case presented in this report, the negative post-operative CT scans make tracheal or esophageal trauma during intubation unlikely, although a micro laceration of the trachea cannot be definitively excluded. There may have also been a microfracture of the lamina that was not appreciated on post-operative imaging. An additional possibility remains that the patient may have developed the mediastinal emphysema as a result of his severe hiccups. There are few case reports of patients developing pneumomediastinum as a consequence of intractable or severe hiccups.8,9 Such cases have only been reported when the hiccups are defined as intractable (more than one month) or persistent (more than 48 hours).8,9 The patient in this case did not meet criteria as his hiccup episodes spontaneously resolved within 48 hours, but this etiology cannot be completely eliminated either. It is likely that the development of the patient’s symptoms was multifactorial, with anesthesia or surgery related microtrauma (tracheal, esophageal, to the lamina papyracea) with post-operative severe hiccups being the final insult, exacerbating the degree of injury and leading to the development of subcutaneous diffuse emphysema. In the presented patient, his mediastinal emphysema resolved with conservative management but close observation is recommended due to the risk of progression to mediastinitis, septic shock, and potentially death.
Conclusion
Functional endoscopic sinus surgery is a commonly practiced and routinely performed procedure. While it is regarded as relatively safe, it is not without complications. Pneumomediastinum may result in a rare but potentially fatal consequence of FESS. Microtrauma of the airway during intubation and bony trauma to the lamina papyracea during the procedure are established causes of this pathology. Persistent hiccups in the post-operative course can also contribute to emphysematous changes. Prompt recognition is imperative to mitigate patient morbidity and mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.