
Abstract
Implant dentistry has become a popularized means of replacing damaged or missing teeth. Although it has become common practice, there are accounts of implants displacing into surrounding structures, commonly the maxillary sinus. We present the case of a 54-year-old man who presented with chronic left sided pain and pressure found to be secondary to a displaced implant obstructing the left maxillary outflow sinus tract. A systematic review was conducted to assess the current management and treatment options for dental implants displaced into the maxillary sinus. Functional endoscopic sinus surgery (FESS) and the lateral window approach were both found to be safe techniques with minimal postoperative complications.
Introduction
Implant dentistry was first introduced 50 years ago, and has since become an effective and reliable treatment option to replace missing teeth.1,2 Recently, the American Academy of Implant Dentistry estimated that 3 million people in the United States currently have dental implants and that this number will increase by 500 000 people annually. 3 Despite the widespread use of dental implants, approximately 5% of patients suffer from dental implant failures.4,5 Implants placed in the maxilla experience higher rates of failure compared to the mandible due to maxillary sinus pneumatization and age-related bone resorption.6,7 Some patients undergo maxillary sinus elevation and grafting prior to implant placement. 8 Still, a small proportion of patients experience a rare complication of the dental implant displaced into the maxillary sinus. 9
Although implants may be displaced immediately into the maxillary sinus during implantation, they may also migrate into the sinus in a delayed fashion. Low bone density, impaired osseointegration, sinus membrane perforation, and poor surgical planning or technique may increase the risk of delayed displacement. 10 The displaced implant may be asymptomatic, but often causes acute or chronic sinusitis and may be associated with oroantral fistulas. Multiple treatment options have been used to remove the displaced implant, including both intraoral approaches and endoscopic sinus surgery. 9 The purpose of this study is to describe a case of a dental implant migrated into the maxillary sinus and to perform a systematic review of the treatment modalities of this rare complication.
Case Reports
A 54-year-old man presented with greater than 3 months of left sided facial pain and pressure. Approximately 3 years prior to presentation, he had 6 dental implants placed when serving as a volunteer at a dental training course. The implants had loosened, and he had removed 4 of them himself and one implant had broken at the gingiva during attempted removal. A CT was obtained, and a portion of the final implant was found in the left maxillary sinus outflow tract (Figure 1). A and B: Pre-operative Coronal CT scan showing partial dental implant lodged in the maxillary sinus outflow tract.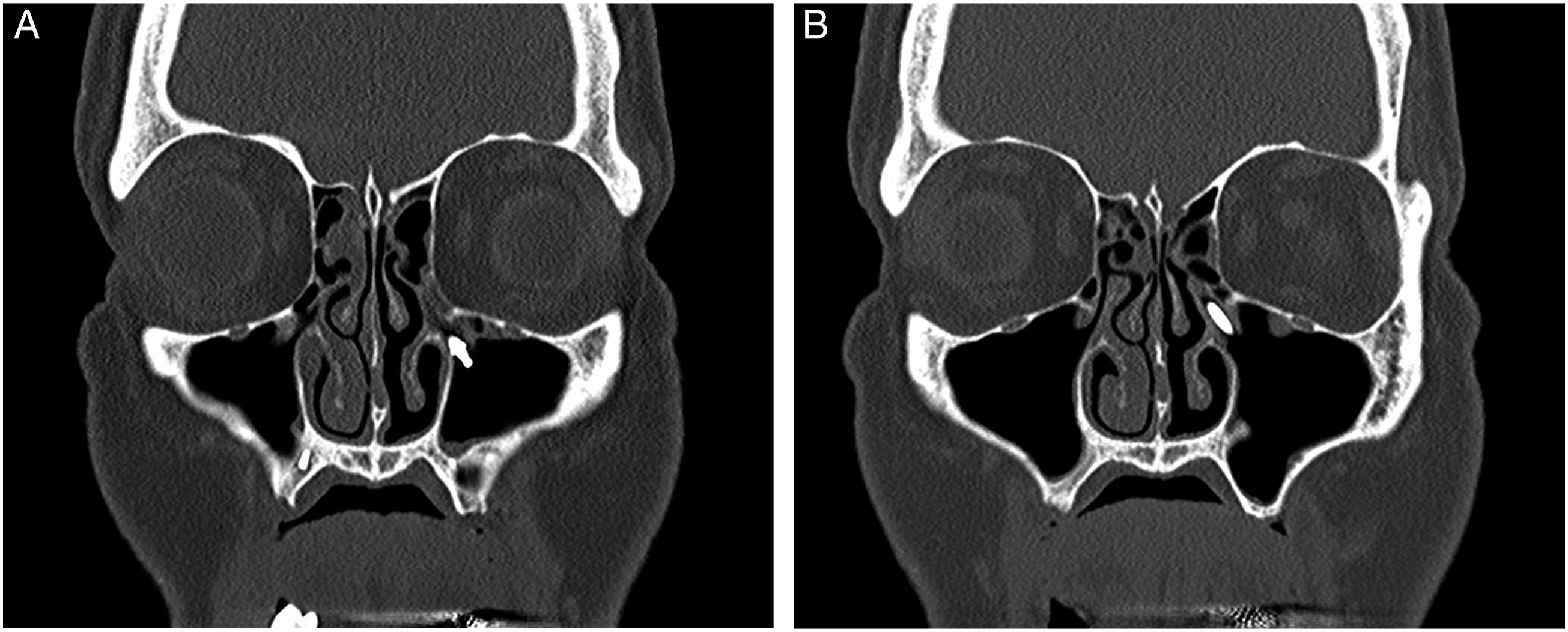
The decision was made to perform an endoscopic retrieval. A standard endoscopic maxillary antrostomy was performed but the implant could not be visualized. The antrostomy was widened inferiorly to a mega antrostomy but the implant was not visible with either angled rigid or a flexible scope. The sinus was filled with saline but the implant was not dislodged. An x-ray was performed and the implant could still be clearly visualized. Therefore, the decision was made to perform an endoscopic anterior maxillotomy to reach the implant which was presumed to be imbedded in the mucosa of the anterior maxillary sinus.
11
An incision was made along the piriform aperture and the tissue of the anterior maxilla was raised using a suction freer, taking care to not injure the infraorbital nerve. The foramen of the infraorbital nerve was visualized, and an maxillotomy was created inferior to the foramen using a 15 degree suction irrigating drill. A zero degree endoscope was placed through the maxillotomy and the implant was visualized embedded in the soft tissue. It was dissected free, then held in place with a suction. Using a 30 degree endoscope and a blakesley forcep through the nasal cavity, the implant was retrieved (Figure 2). At his postoperative visit, the patient had no paresthesias and complete resolution of his prior facial pain. A and B: (A) Suction through anterior maxillotomy with endoscope and blakesley forcep through nasal cavity to extract implant (B) Purple showing medial maxillary and red showing anterior maxillary approaches to remove implant.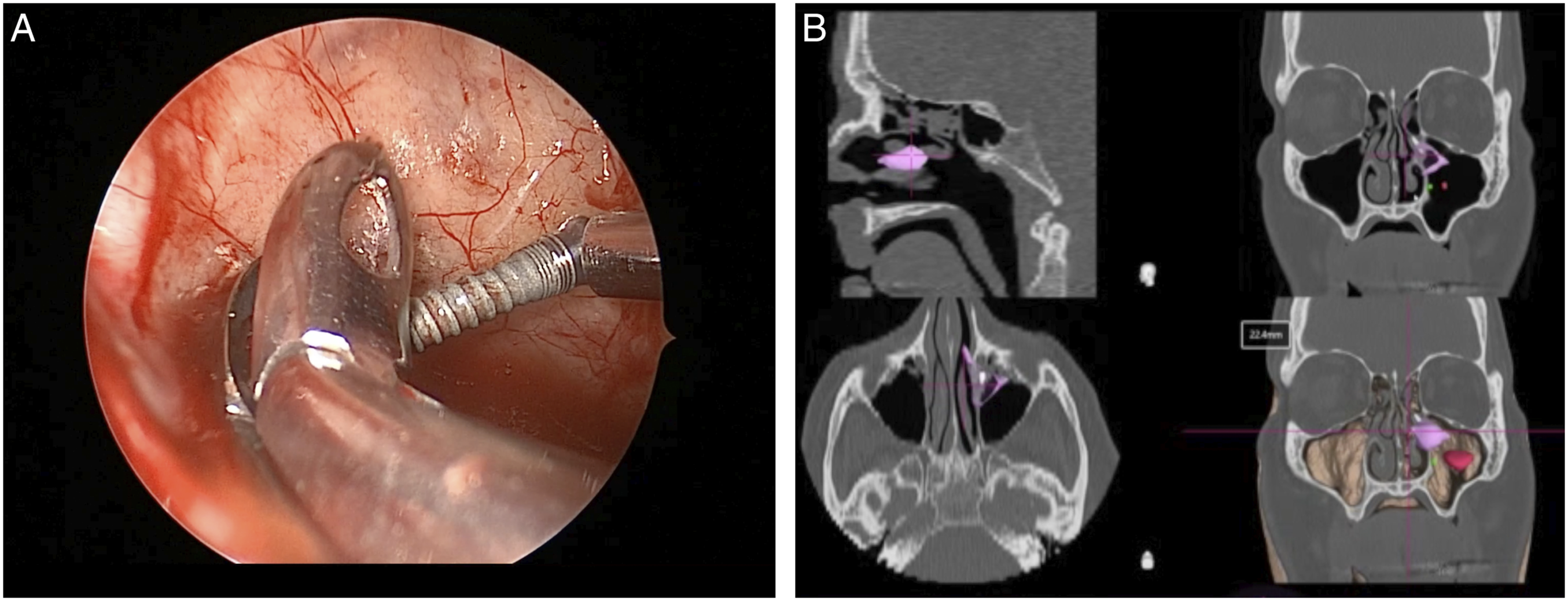
Methods
A systematic review of published literature was performed to assess the current management techniques for removal of dental implants displaced into the maxillary sinus. The study was reviewed by the Keck School of Medicine of the University of Southern California Institutional Review Board and was determined to be exempt.
Search Strategy
A literature search was conducted on 3 databases (PubMed, Embase, and Cochrane Library) using the keywords (“implant” OR “implants” [Title] or Abstract) AND (“sinus” OR “sinuses” OR “sinusitis” [Title]) AND (“dislodged” OR “displaced” OR “migrated” OR “removed” OR “retrieved” [All Fields]). Articles were reviewed for relevance by 2 authors (D.H.L. and S.S.J.) using Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 12
Data Collection
A standardized data form was used by 2 authors (D.H.L. and S.S.J.) to independently extract raw data from the selected studies. Inclusion criteria included all patients undergoing removal of a dental implant displaced into the maxillary sinus. Patients were excluded if they were under the age of 18. Variables included study design and sample size, implant extraction technique, presence of sinonasal symptoms, presence of oroantral fistula, and duration of follow-up.
Outcome Measures
The primary outcomes included surgical success, acute postoperative complications, and late complications. Surgical success was defined as the successful removal of the displaced implant. Acute postoperative complications included surgical site infections, hemorrhage, persistent sinusitis, or other sequelae of surgery requiring additional treatment within 30 days. Late complications were defined as occurring more than 30 days after the initial surgery and included recurrent episodes of sinusitis requiring additional surgery, numbness in the infraorbital region, or numbness of the maxillary teeth. Statistical analysis was performed in R (version 4.0.0).
Results
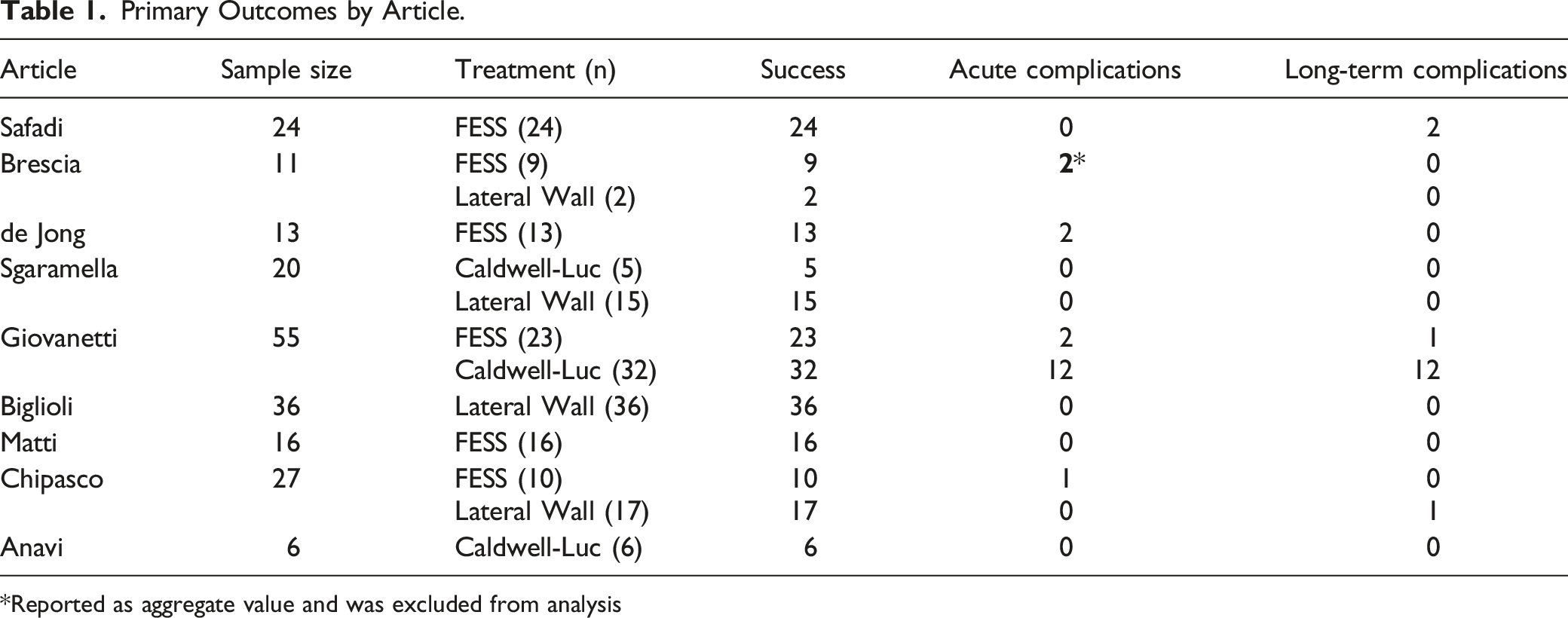
The initial literature search returned 439 records after removing duplicate records. Titles and abstracts were then used to screen articles for relevance. The full texts of the remaining 25 articles were then used to determine final eligibility for inclusion. Twelve studies were initially included in the analysis,7,9,10,13-21 but 3 studies included aggregate outcomes for multiple surgical techniques and were thus excluded from the meta-analysis (Figure 3).10,14,20 From the 9 included articles, a total of 208 patients (mean age 56 years, range 28–88 years) were included in the final data analysis, including 103 females (50.9%). Outcomes for individual studies are reported in Table 1. Systematic review results and PRISMA flowsheet. Primary Outcomes by Article. Reported as aggregate value and was excluded from analysis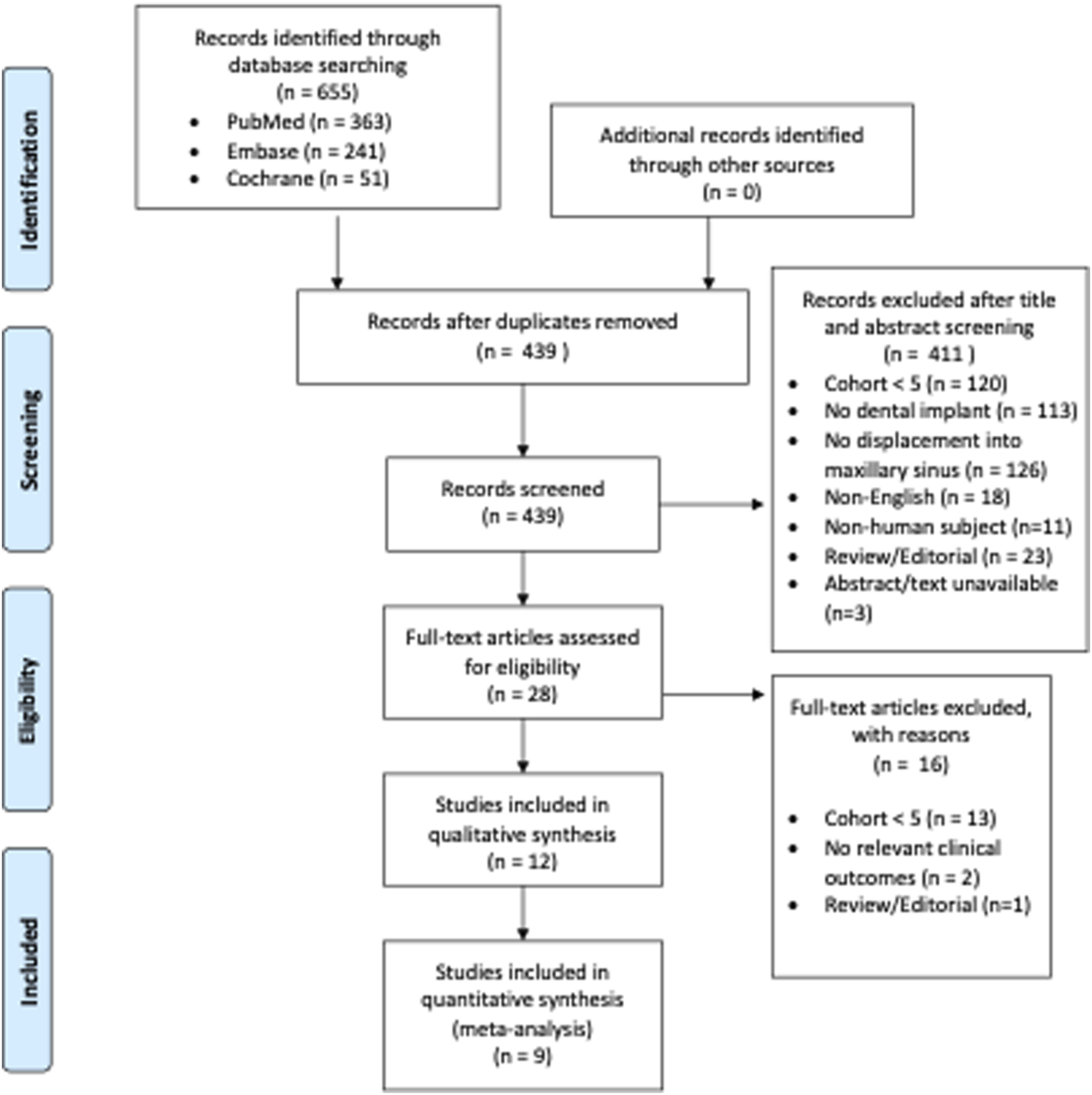
Surgery typically involved one of 3 techniques for implant removal: 95 patients (45.7%) underwent functional endoscopic sinus surgery (FESS) with 14 of those patients (6.7%) undergoing simultaneous intraoral closure of OAF, 43 patients (20.7%) underwent Caldwell-Luc, and 70 patients (33.7%) underwent a lateral window approach. The decision regarding surgical technique was typically guided by the patient’s presenting symptoms, with authors generally preferring FESS to address sinonasal symptoms. Oral approaches, that is, lateral window and Caldwell-Luc, were typically used for patients without sinonasal symptoms, or to simultaneously address oroantral fistula. As a result, a higher proportion of patients undergoing FESS presented with sinonasal symptoms (62.5%). Conversely, patients undergoing a lateral window approach typically did not have sinonasal symptoms (14.0%) but had higher rates of oroantral fistula (24.3% vs 13.0% of patients undergoing FESS).
All surgeries successfully removed the displaced implant, and thus the technical success rate for all techniques was 100%. However, rates of acute postoperative complications differed significantly by technique, with 27.9% of patients undergoing Caldwell-Luc experiencing a postoperative complication. In comparison, 5.8% of patients undergoing FESS experienced a postoperative complication, and no patients undergoing lateral window experienced a postoperative complication. This difference in postoperative complication rate was statistically significant (Chi-Square test, P = <0.001). Postoperative complications following FESS were mostly cases of persistent sinusitis, but also included one case of hemorrhage and one infection of the oral fistulectomy site. None of these complications required additional surgery. In addition to persistent sinusitis, complications following Caldwell-Luc included fistula persistence, maxillary paresthesia, and suture dehiscence, and a majority of these complications required additional surgery.
Delayed complications occurred in 16 patients. Twelve of these were observed in a single study, demonstrating recurrence of sinonasal symptoms following Caldwell-Luc. Two delayed complications occurred in patients who underwent FESS, with one patient experiencing maxillary pain 2 months after surgery and a second experiencing intranasal synechia. One patient who underwent lateral window approach presented 2 years after their surgery with recurrent sinusitis and oroantral fistula and was treated with FESS and intraoral fistulectomy.
Discussion
Migration of a dental implant into the maxillary sinus is a rare but significant complication with limited evidence regarding its management. A review of the literature yielded numerous case reports but few cohort studies. Of these, most report the outcomes for a single technique for implant removal. Therefore, this study represents, to our knowledge, the first systematic review of techniques for the management of dental implants displaced into the maxillary sinus. In addition, we report the novel application of an endoscopic anterior maxillotomy approach as a solution to a challenging retrieval case.
Approximately 10% of sinusitis cases are odontogenic in etiology, although other reports cite proportions as high as 40%. 22 The common causes of odontogenic sinusitis vary and include OAFs, inflammatory cysts, odontogenic cysts, peri-implantitis, and foreign bodies. Since its development and widespread adoption, endoscopic sinus surgery has been used to safely and effectively treat chronic maxillary sinusitis of dental origin.23,24 In addition to successful removal of foreign bodies, endoscopic sinus surgery relieves obstruction of the osteomeatal complex (OMC). 25 The maxillary sinus is typically accessed through the middle meatus, termed a maxillary antrostomy. Cases with severe inflammation or cases of difficult foreign bodies which require extended access may be approached by combining a maxillary antrostomy with an inferior antrostomy through the inferior meatus, also referred to as mega antrostomy. 26 Additionally, the opening can be further widened by removing the anterior and inferior lateral nasal wall, termed an endoscopic medial maxillectomy. 27 While the endoscopic transnasal approach is effective at treating sinus pathology, it has limited ability to treat oral pathologies such as OAFs.
The Caldwell-Luc approach was historically used as an intraoral approach to the maxillary sinus. The procedure accesses the anterior maxillary wall through a gingivolabial incision superior to the canine tooth, but was associated with a high rate of complications.28-30 In its place, some oral surgeons have favored a lateral window approach, which involves the creation of a bone flap on the anterolateral maxillary wall.31,32 Although the lateral window approach has significantly lower complication rates, neither intraoral approach addresses a chronically inflamed OMC. 18
In our meta-analysis, we found that all methods were uniformly successful at retrieving the migrated dental implant. However, the complication rate varied significantly, with more than a quarter of patients undergoing Caldwell-Luc experiencing a complication. Complications after FESS were rare and mostly involved persistent sinusitis, whereas no complications were observed after a lateral window approach. Of note, a much higher proportion of patients undergoing endoscopic sinus surgery presented with sinonasal symptoms compared to patients undergoing a lateral wall approach, reflecting a tendency to refer for FESS if sinonasal symptoms are present. Chiapasco et al. 9 have similarly proposed a treatment algorithm, where patients with sinonasal symptoms undergo FESS, combined with an oral approach for closure of an oroantral fistula if present. If no sinonasal symptoms are present, Chiapasco’s algorithm suggests a lateral window approach, which may be performed with only local anesthesia. Our systematic review found that FESS and a lateral window approach are equally safe and effective, which would support the use of this treatment selection algorithm.
Our case represents a particularly challenging implant retrieval. In our review, a number of studies reported converting an insufficient medial antrostomy into a mega antrostomy, although none reported additional difficulty visualizing or retrieving the implant from an endoscopic anterior approach. In our case, the implant was displaced into the anterior maxillary sinus, which remains a challenge to visualize endoscopically. Rather than a transoral approach, we elected for an endoscopic endonasal anterior maxillotomy, which uses a vertical incision along the pyriform aperture to gain access similar to the sublabial Caldwell-Luc procedure. However, avoiding a sublabial incision likely avoids damaging the anterosuperior alveolar nerve, which may prevent the infraorbital numbness often associated with the Caldwell-Luc procedure. Further, reducing contamination by oral flora may improve rates of post-operative infection and oroantral fistulas.
Conclusion
Multiple techniques exist for the removal of a dental implant migrated into the maxillary sinus. Our systematic review supports the use of endoscopic sinus surgery for any patients presenting with associated sinonasal symptoms, whereas a lateral window approach is similarly safe and effective for asymptomatic patients. The Caldwell-Luc procedure is associated with higher rates of complications. Alternative options, such as endoscopic endonasal anterior maxillotomy, may be viable options for challenging removals of anteriorly displaced implants.
Footnotes
Author’s Note
Meeting: Cedar Sinai Eerie ENT, Los Angeles, CA October 2021.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.