
Abstract
Objective
To determine age-related risk factors for chronic rhinosinusitis (CRS) with asthma.
Methods
Data were obtained from a national survey of non-hospitalized civilians conducted by the Korean Center for Disease Control and Prevention. CRS diagnosis was based on the guidelines of the European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Asthma was judged based on whether the patient had been diagnosed with asthma in the past. Of the 45,811 survey participants, 26,335 were included in the cross-sectional study. Participants included in the study were divided into the control, CRS, and CRS with asthma groups. Age-related risk factors were analyzed in patients aged < 60 or > 60 years. Univariate logistic analyses were performed to evaluate the relationship between groups. Risk factors included age, sex, household income, residence, education level, occupation, and body mass index (BMI).
Results
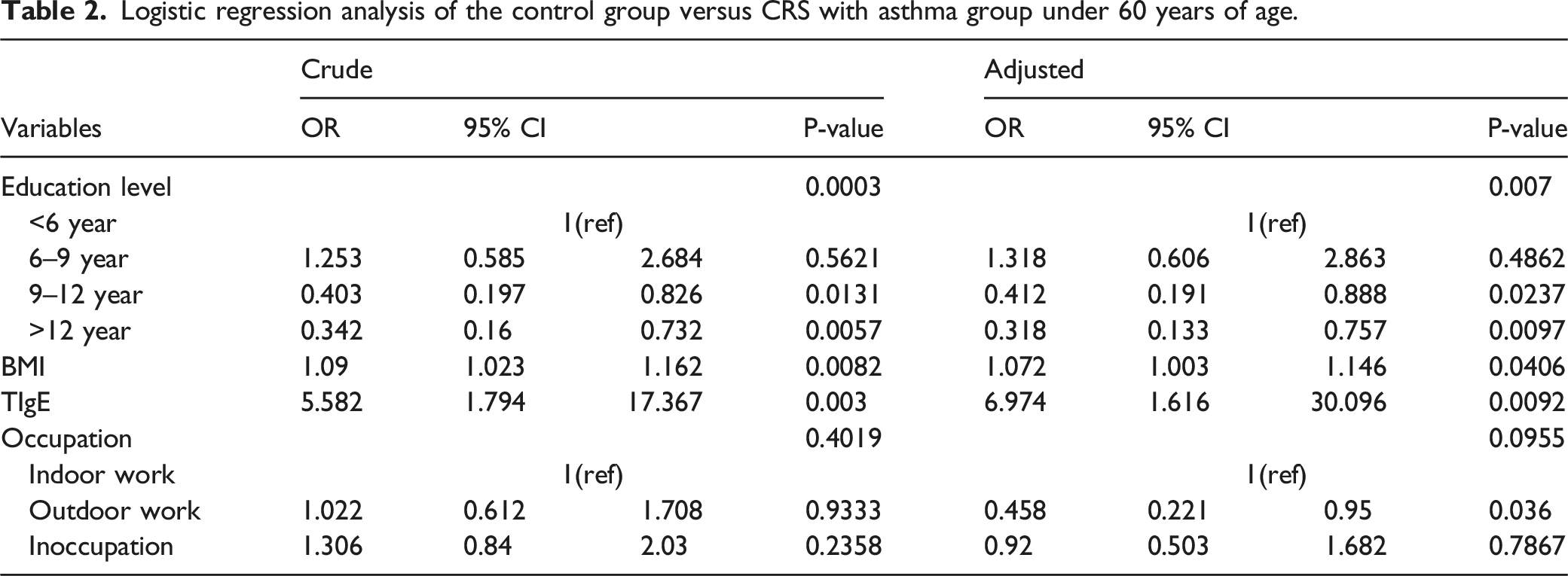
Education level (Odds Ratio [OR]: 0.342, P = .0003), BMI (OR: 1.09, P = .0082), and total IgE (TIgE) levels (OR: 5.582, P = .003) were significantly different between the control and the CRS with asthma group. Education level (OR: 0.478, P = .0016) and TIgE levels (OR: 4, P = .0218) were significantly different between the CRS and CRS with asthma groups under 60 years of age. BMI (OR: 1.087, P = .0443; OR: 1.104, P = .0224) showed a significant difference between all three groups with age > 60 years.
Conclusion
Progression to CRS with asthma is influenced by education level, occupation, and TIgE levels in patients under 60 years of age. BMI was the only influencing factor associated with the progression to CRS with asthma in those aged > 60 years.
Introduction
Chronic rhinosinusitis (CRS) is a common chronic disease with nasal congestion or discharge as the main symptom. 1 The CRS phenotype can be broadly defined as CRS with or without nasal polyps. Its sub-phenotypes include allergic fungal sinusitis and CRS-related respiratory diseases aggravated by aspirin. 2 CRS might be associated with many diseases, such as asthma, otitis media with effusion, acute myocardial infarction, stroke, and anxiety.3,4 Asthma is considered to be an important factor in the pathogenesis and development of CRS. 5 Studies have shown that CRS and asthma often occur in the same patient.6,7 Nearly 25% of patients with CRS have asthma, while the average prevalence of asthma in adults is only 5%. 8 When CRS presents with asthma, the chances of relapse and its treatment difficulty increase. The prevalence of CRS and asthma increase with age, especially after the age of 40. 9 The number of elderly patients with CRS is four times that of young patients with CRS, and the number of elderly patients with asthma is also significantly higher than that of young patients with asthma. 10
The united airway disease hypothesis states that upper and lower airway diseases manifest as a single inflammatory process in the respiratory tract. The upper airway associated with CRS and the lower airway associated with asthma have continuous airway anatomy, cellular and humoral immunity, and exposure to similar risk factors. 11 In addition, nasal irritant allergens can induce bronchitis. Conversely, bronchial provocation can induce allergic inflammation in the nose, providing evidence that the upper and lower airways are united.12,13 Thus, CRS and asthma are interrelated in the concept of a unified airway. 14 So far, studies on the relationship between age and CRS with asthma have not been reported. Therefore, the objective of this study was to determine the age–related risk factors for CRS with asthma.
Patients and methods
Survey used for data collection
The Korean National Health and Nutrition Examination Survey (KNHANES) is a national survey conducted among non-institutionalized civilians by the Korea Centers for Disease Control and Prevention, which monitors trends in health risk factors and the prevalence of major chronic diseases. It aims to assess the health and nutritional status of Koreans through health interviews, nutrition assessments, and health examinations. Study participants were selected by household unit sampling and allocated in a stratified, multistage, probability–based proportional manner according to the household register with the aim that the survey population represents the entire Korean population to the greatest extent.
Study population
The diagnosis of CRS was based on the guideline of European position paper on rhinosinusitis and nasal polyps 2020 (EPOS2020).
15
Questions related to CRS addressed the following four symptoms persisting for at least 12 weeks: anterior/posterior nasal drip, nasal obstruction, facial pain or pressure, and olfactory dysfunction. CRS was diagnosed when more than two of these symptoms with at least one of either anterior/posterior nasal drip or nasal obstruction were present, and if endoscopic findings showed nasal polyps and/or mucopurulent discharge with or without edema/mucosal obstruction primarily from the middle meatus. Asthma was diagnosed based on a doctor's inquiry: “Have you ever been diagnosed with asthma by a doctor in the past?” A positive answer to this question was defined as having asthma. All study participants underwent nasal endoscopy unless they disagreed or had contraindications. The endoscopy was performed by trained otorhinolaryngology residents, and the images recorded by the camera were further reviewed by otorhinolaryngology experts. However, the Lund–Kennedy score was not analyzed, which is a limitation of this study. 45,811 survey participants representing the Korean population were selected for this cross-sectional study, of which 26,335 were included in this study after excluding 11,141 participants who were <19 years old, 4,647 with missing data, 3,232 with no endoscopic examination, and 456 with null or unknown responses (Figure 1). The included participants were divided into the control, CRS, and CRS with asthma groups. Age-related risk factors were analyzed in patients aged < 60 or > 60 years. Flowchart of the study population.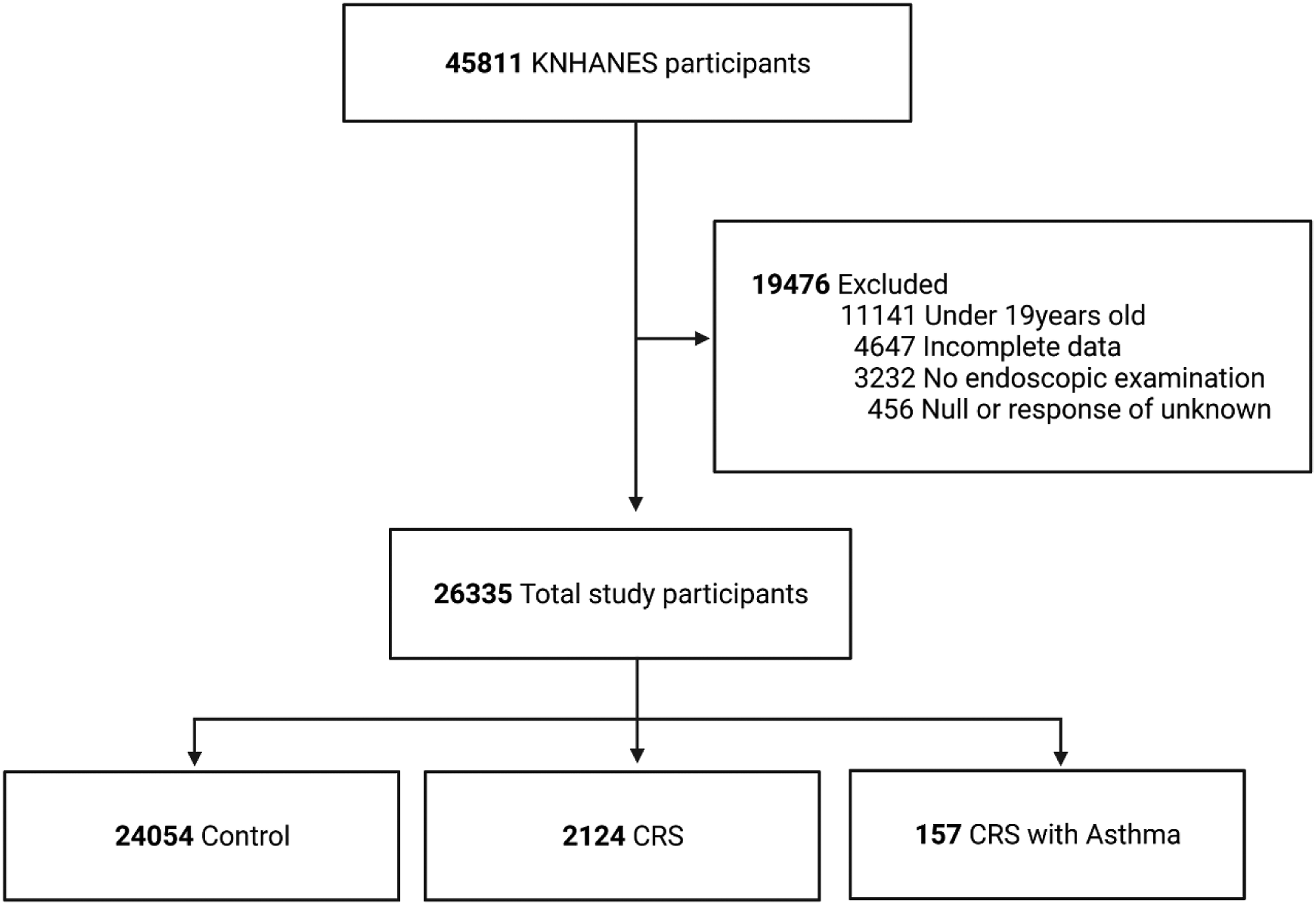
Assessment of variables
Demographic data of the participants, such as age, sex, alcohol consumption and smoking, body mass index (BMI), education level, occupation, residency, and household income were collected. These data were classified as follows. Education level was categorized as less than 6 years, 6-9 years, 9-12 years, and more than 12 years of education groups. Occupation was divided into three groups: indoor working, outdoor working, and non-working. Smoking history was categorized as either smoking or nonsmoking. Drinking history was divided into three groups: no drinking, more than 4 times a week, and less than 4 times a week. The family income was divided into four groups. The residential areas were divided into urban and rural areas. Immunocap 100 was used to measure serum total IgE (TIgE) levels and specific IgE levels of common indoor allergens.
Statistical analysis
SPSS version 20.0 was used for all data analyses. Logistic regression analysis was performed to analyze the association between the control, CRS, and CRS with asthma groups. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. For multivariate analysis, confounding factors for adjustment included sex, household income, residency, education level, BMI, smoking, alcohol consumption, TIgE levels, and occupation. Statistical significance was set at P < 0.05.
Results
Prevalence
The prevalence of CRS and asthma slowly decreased with age. Subsequently, it increased slowly. The prevalence of the diseases tended to be the same at ≥60 years of age (Figure 2). Prevalence of diseases in different age groups.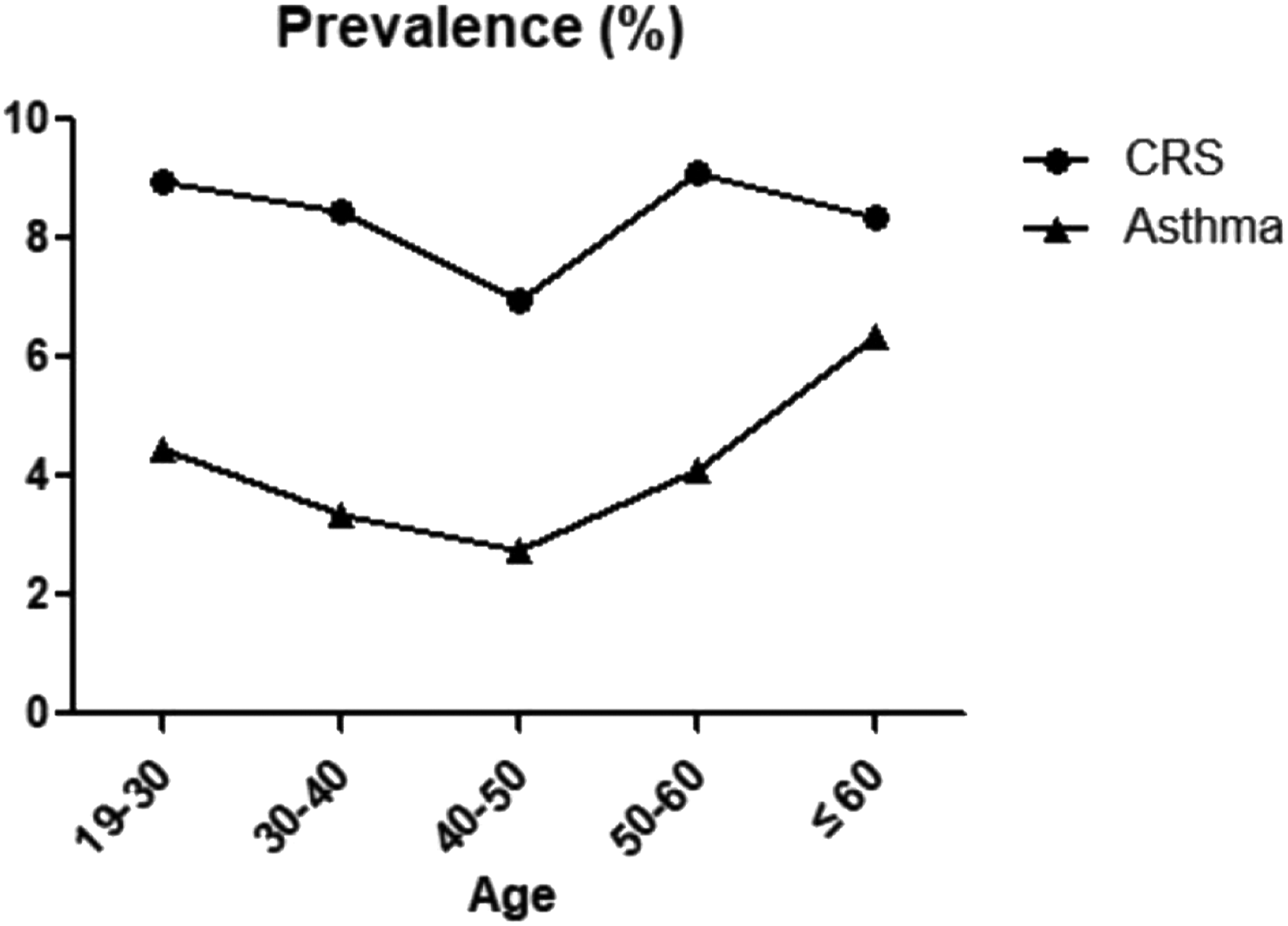
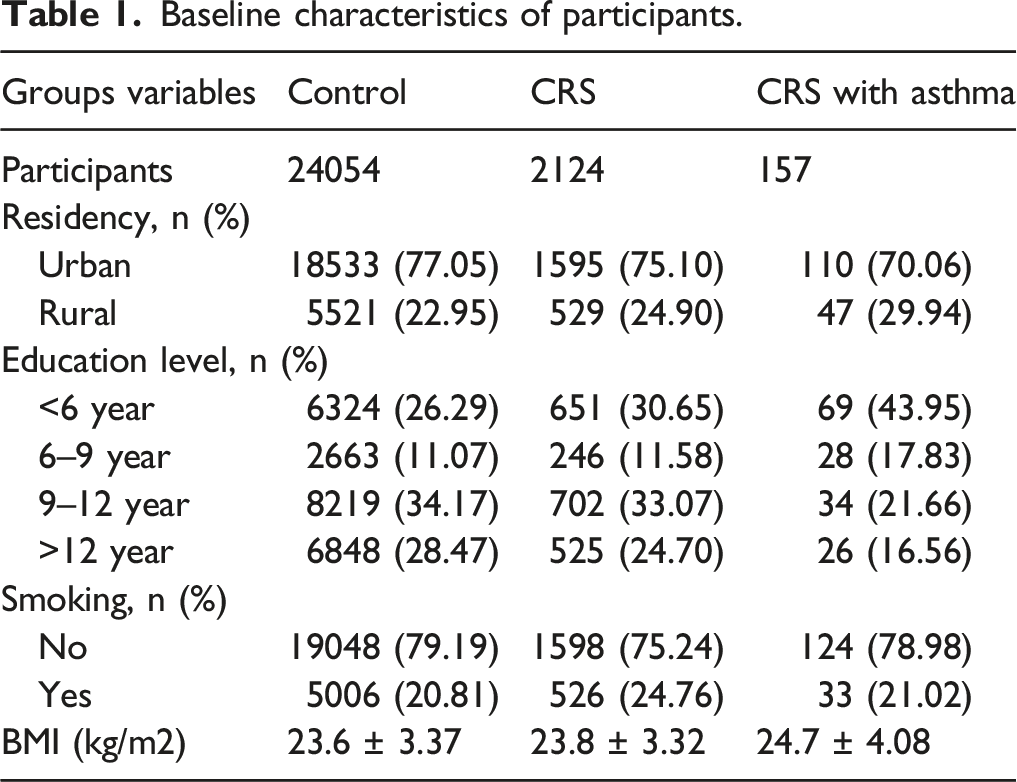
Baseline characteristics
Baseline characteristics of participants.
Association between the control and CRS with asthma groups under 60 years of age
Logistic regression analysis of the control group versus CRS with asthma group under 60 years of age.
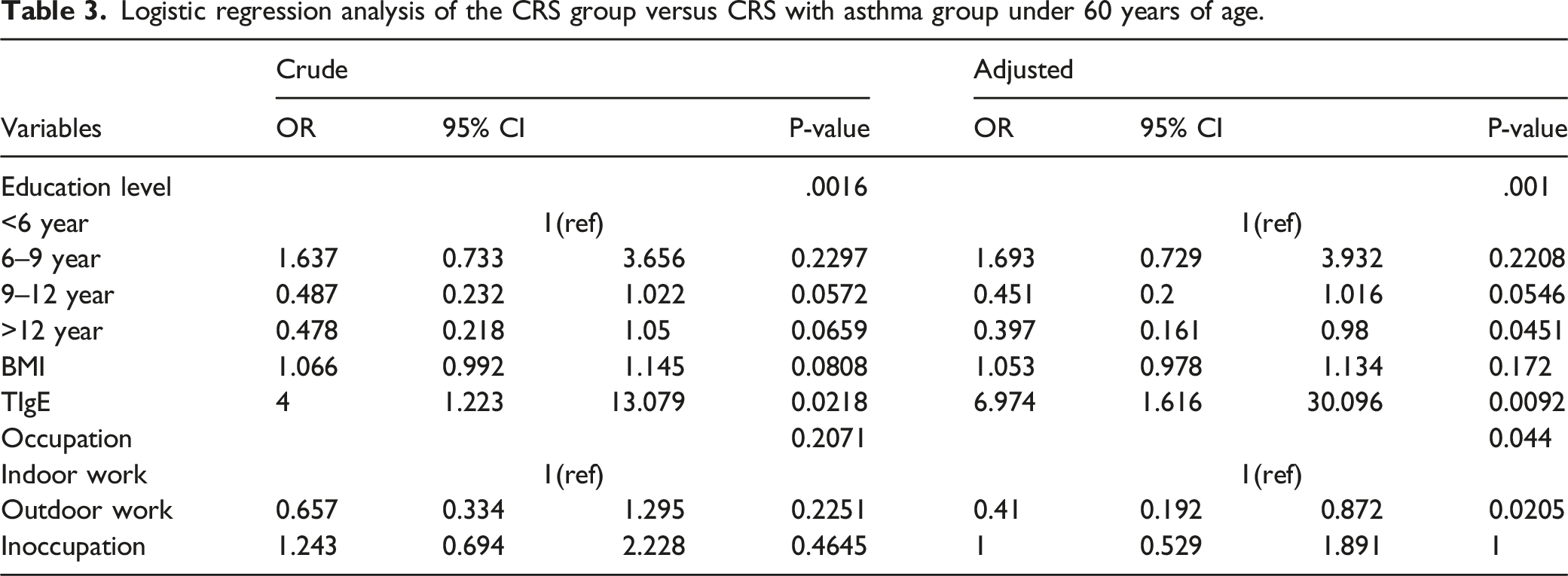
Association between the CRS and CRS with asthma groups under 60 years of age
Logistic regression analysis of the CRS group versus CRS with asthma group under 60 years of age.
Association between the control and CRS groups versus CRS with asthma group over 60 years of age
Logistic regression analysis of the control group and CRS group versus CRS with asthma group over 60 years of age.

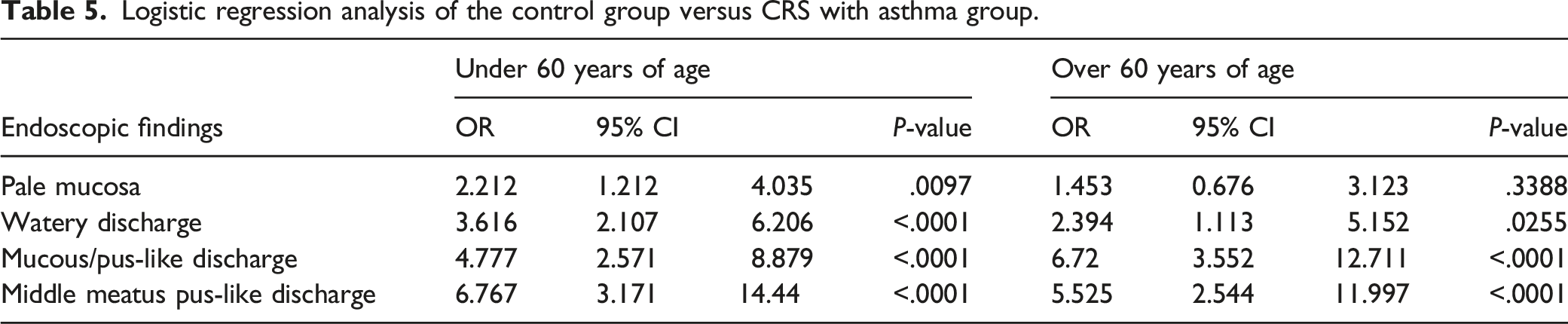
Differences in nasal endoscopic findings between the control and the CRS with asthma groups
Logistic regression analysis of the control group versus CRS with asthma group.
Discussion
In this study, we found little difference in risk factors between the control and CRS groups when they developed CRS with asthma in people under 60 years of age. BMI was found to be an important factor affecting the development of CRS with asthma in people over 60 years of age. It has been reported that high BMI is a pathogenic factor for CRS 16 and also the main risk factor for asthma in children and adults. 17 Based on more than 26,000 samples from KNHANES, this study found that the average prevalence of CRS was 8.36%, roughly consistent with the CRS prevalence of 6.95% in a 2011 study in Korea. 18 Interestingly, the prevalence of CRS and asthma tend to be consistent at the age of 60 years and stable after 60 years, which is the same as the global definition of people over 60 years old as the elderly, which is consistent with survey results of more than 73,000 samples from Canada. 19 These results observed in relation to patients with asthma over the age of 60 years were similar to those reported by Braman et al. 20 based on the cut-off point of 60 years of age. Therefore, we analyzed the factors influencing CRS with asthma in different groups of people under and over 60 years of age to reveal possible factors affecting the occurrence of the disease.
Multivariate logistic analysis showed that when controls and patients with CRS developed CRS with asthma, they were equally affected by factors such as education, occupation, and TIgE levels. However, in contrast to the control group, when patients with CRS progressed to CRS with asthma, they were not affected by BMI. This may be because BMI is a pathogenic factor that does not play a role in the development of CRS with asthma in patients with CRS. Our results showed that lower level of education presented more likelihood towards the development of CRS with asthma, which is similar to the results of Hetlevik et al. 21 Their statistical results showed that more than 70% of asthmatic patients had received only basic education. We could also assume that a low level of education could lead to low income, resulting in poor housing and medical conditions. Researchers have reported that people are easily exposed to indoor biological pollutants in urban environments. 22 The main risk factors for asthma include indoor dust mites and animal dander, which may explain the higher asthma incidence rate in urban areas than in rural areas. This could also explain why outdoor workers were less likely to develop CRS with asthma in our study. Among participants over 60 years of age, BMI was the only factor that led to CRS with asthma. This might be because with increasing age, immunosenescence could lead to low immune function. 23 Most experimental data on immune changes in aging individuals compared with those in young healthy individuals showed that immune parameters of many older people decreased by varying degrees. 24 This may explain the reason for only one influencing factor that could lead to the development of CRS with asthma in the elderly group. Many studies have pointed out that metabolic syndromes can lead to diseases such as CRS and asthma, and that BMI is the most important factor that can directly lead to CRS and asthma in metabolic syndromes,25,26 whether BMI indirectly affects the development of other diseases in metabolic syndromes, such as hypertension, into CRS or asthma requires further research.
By analyzing the endoscopic results, it was evident that most factors, including age <60 years, affected the development of CRS with asthma in the control group, and the only factor affecting people >60 years of age, but not those <60 years of age, was pale nasal mucosa. This may be explained by immunosenescence because a pale nasal mucosa is the result of immune response activities. No factors affected the development of CRS with asthma in patients with CRS, regardless of age (over or under 60 years). This might indicate that the endoscopic results could not draw a different conclusion between patients with CRS and those with CRS and asthma.
This study had some limitations. First, owing to our cross-sectional study design, it was difficult to demonstrate disease progression and clearly define the causal relationship between various factors and the prevalence of CRS with asthma. In addition, because the survey only provided sensitization data for indoor allergens without outdoor allergen data, it was challenging to accurately evaluate the effects of allergens on indoor and outdoor workers. However, this is the first study to analyze the correlation between various factors and the incidence rate of CRS with asthma using nationwide survey data. Moreover, endoscopic diagnoses made by specialists and serum allergen tests provided strong objective support for the results. Although deeper longitudinal studies are necessary to clarify causality, this national study provides several useful pointers for otorhinolaryngology clinicians to diagnose patients with CRS and asthma. This study, using nationwide large sample data, showed that the prevalence rates of CRS and asthma were same for those aged ≥60 years. When controls and patients with CRS aged <60 years progressed to CRS with asthma, their prevalence was majorly influenced by education level, occupation, and TIgE levels. BMI was the only influencing factor for patients >60 years of age with progression to CRS complicated by asthma. This emphasizes the importance of preventing various diseases that may occur due to high BMI with increasing age. Endoscopic findings also showed minimal differences in the control group <60 years of age and those >60 years of age who developed CRS with asthma. Regardless of the age group, it was reasonable to assume that the development of CRS with asthma in the CRS group was not affected by endoscopic findings (Figure 3). Factors influencing the development of CRS with asthma in the control and CRS groups under or over 60 years of age.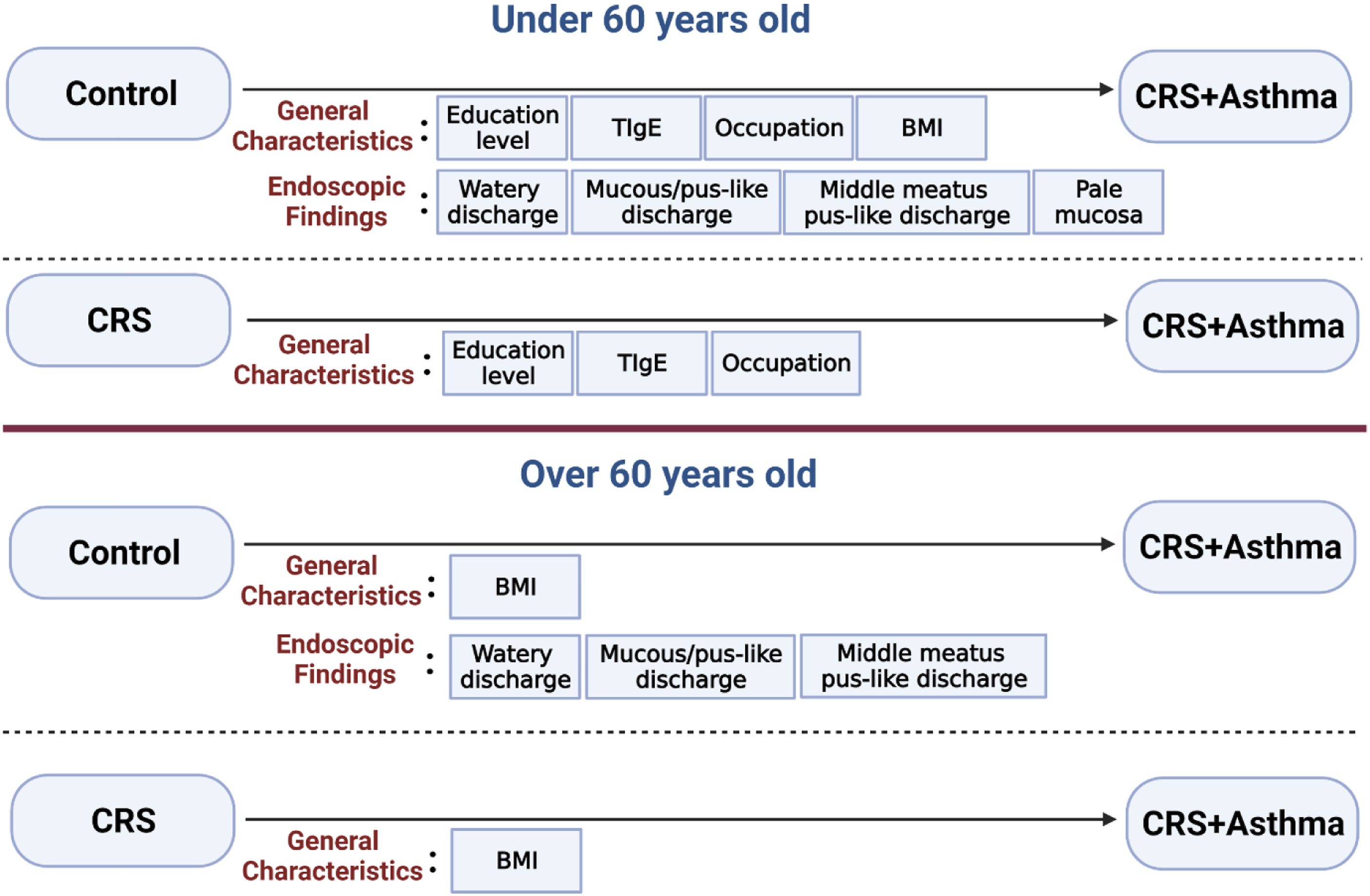
Footnotes
Acknowledgment
We thank the 150 residents of the Otorhinolaryngology Departments of 47 training hospitals in South Korea for participating in this survey and members of the Division of Chronic Disease Surveillance of the Korea Centers for Disease Control & Prevention for their dedicated work. This research was also supported by the Statistical Support Project for Writing Medical Papers using the Korea National Health and Nutrition Examination Survey (KNHANES).
Author contributions
Writing—original draft preparation: Junhu Tai, data collection: Yujin Jeong and Jaehyung Park, literature search: Kijeong Lee and Munsoo Han, review and editing: Tae Hoon Kim, Supervision: Tae Hoon Kim. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
All participants provided written informed consent and the survey protocol was approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (2010-02CON-21-C, 2011-02CON-06-C, and 2012-01EXP-01-2C).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Basic Science Research Program, National Research Foundation of Korea, funded by the Ministry of Science and Technology and the Ministry of Science, ICT and Future Planning (2017R1A2B2003575 and NRF-2020R1A2C1006398); the Ministry of Science and ICT, Korea, under the ICT Creative Consilience program (IITP-2022-2020-0-01819), supervised by the Institute for Information and Communications Technology Planning and Evaluation (IITP); and the Korea Health Technology R&D Project (HI17C0387, HI22C1302) through Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare. This research was also supported by a Korea University grant and a grant from the Korea University Medical Center and Anam Hospital in Seoul, Republic of Korea.
Informed consent
Written informed consent was obtained for each participant.