
Abstract
Congenital hemifacial hypertrophy, an uncommon developmental disease, is characterized by unilateral overgrowth in at least one body part, which can result in significant asymmetry. Meckel reported the first patient of congenital hemifacial hypertrophy in 1822. Since then, numerous cases have been investigated. This study reports a 2-year-old child diagnosed with hemifacial hypertrophy combined with unilateral tonsillar hypertrophy and parapharyngeal space lipoma. We concentrated on the treatment options as well as the related head and neck symptoms.
Introduction
A 2-year-old girl was admitted to our department due to right face and neck enlargement. The patient exhibited congenital asymmetry, which could have been aggravated with the significant enlargement of right side compared with the left. According to her mother, the right face and neck enlarged progressively, which became apparent lately. In addition, anatomic abnormality in family history was not reported. Without any abnormality in their respective antecedents, the parents (34-/28-year-old) were young, healthy, and non-consanguineous.
The patient was born by normal vaginal delivery at full term, and her birth weight was 3900 g, with no occurrence of perinatal issues. There was no obvious abnormality in the mental or motor development of the patient. She was capable of independently walking when she was 11 months old, and her speech skills were developed in desired time. In addition, there were no obvious abnormalities in her physical performance.
Physical examination revealed gross asymmetry in her facial appearance (Figure 1), with right face enlargement (including mandible and neck). The soft tissue thickness of the right mandibular and neck increased, accompanied by slight prolapse compared with the left side. Both mandible and neck were visibly asymmetric and enlarged in comparison with the other side. Moreover, lymphadenopathy was not observed. Photograph of the patient, aged 2 years, demonstrating facial asymmetry with right-sided facial and neck enlargement.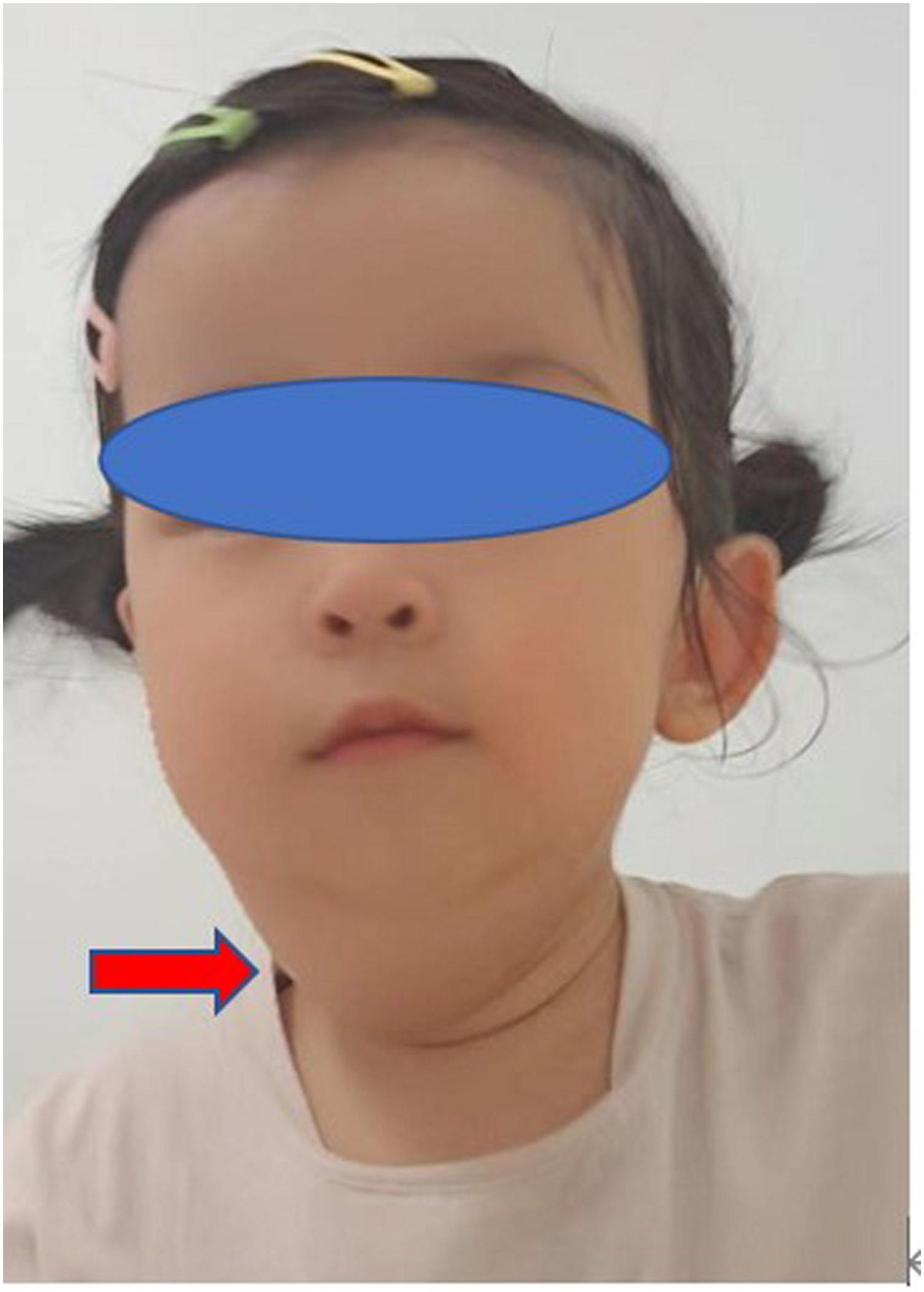
Upon intra-oral examination, the tonsilla was found to be asymmetric, the tonsilla and soft palate on the right side were hypertrophic, and the right palatine tonsil increased by 2–3 folds in size when compared with the left side (Figure 2). Normal shape and size were observed in teeth and tongue, with no additional dysmorphic characteristics. Differences in limb measurements were not significant between both sides. In addition, other physical examinations detected no obvious abnormalities. Photograph during surgery, showing that the right palatine tonsil was 2 to 3 times larger than the left one.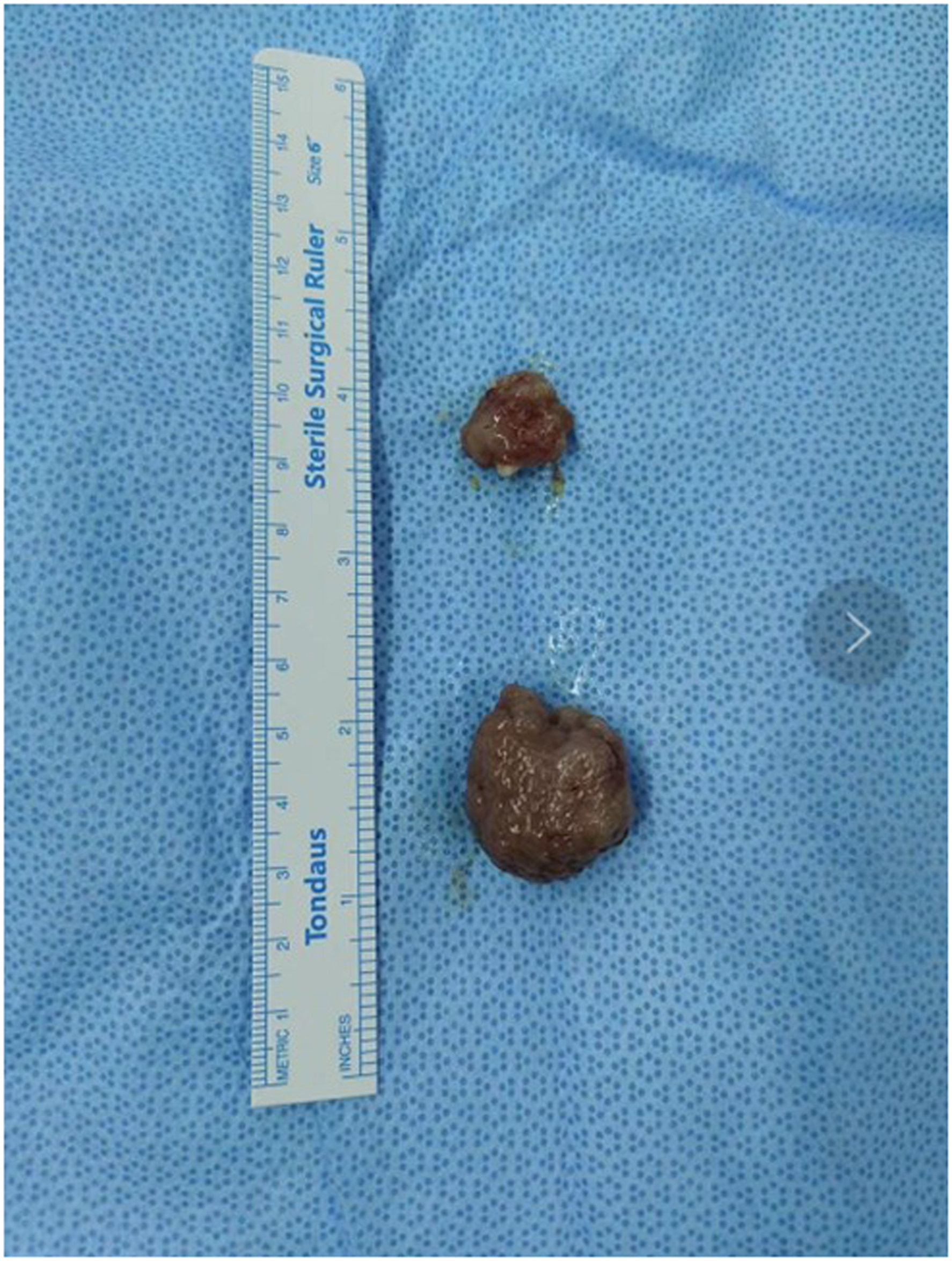
MRI examination displayed diffuse hypertrophy or protrusion due to subcutaneous lipids within the parapharyngeal space and neck (Figure 3). CT examination indicated that orbital bones, maxilla, and mandible were not enlarged. (A) Series of images from T2-weighted sequence and (B) T1-weighted sequence. Images were acquired following contrast injection of 15 ml gadolinium chelate (5-mm axial slices). Isolated hypertrophy on the right combined with unilateral tonsillar hypertrophy and parapharyngeal space lipoma is clearly visible.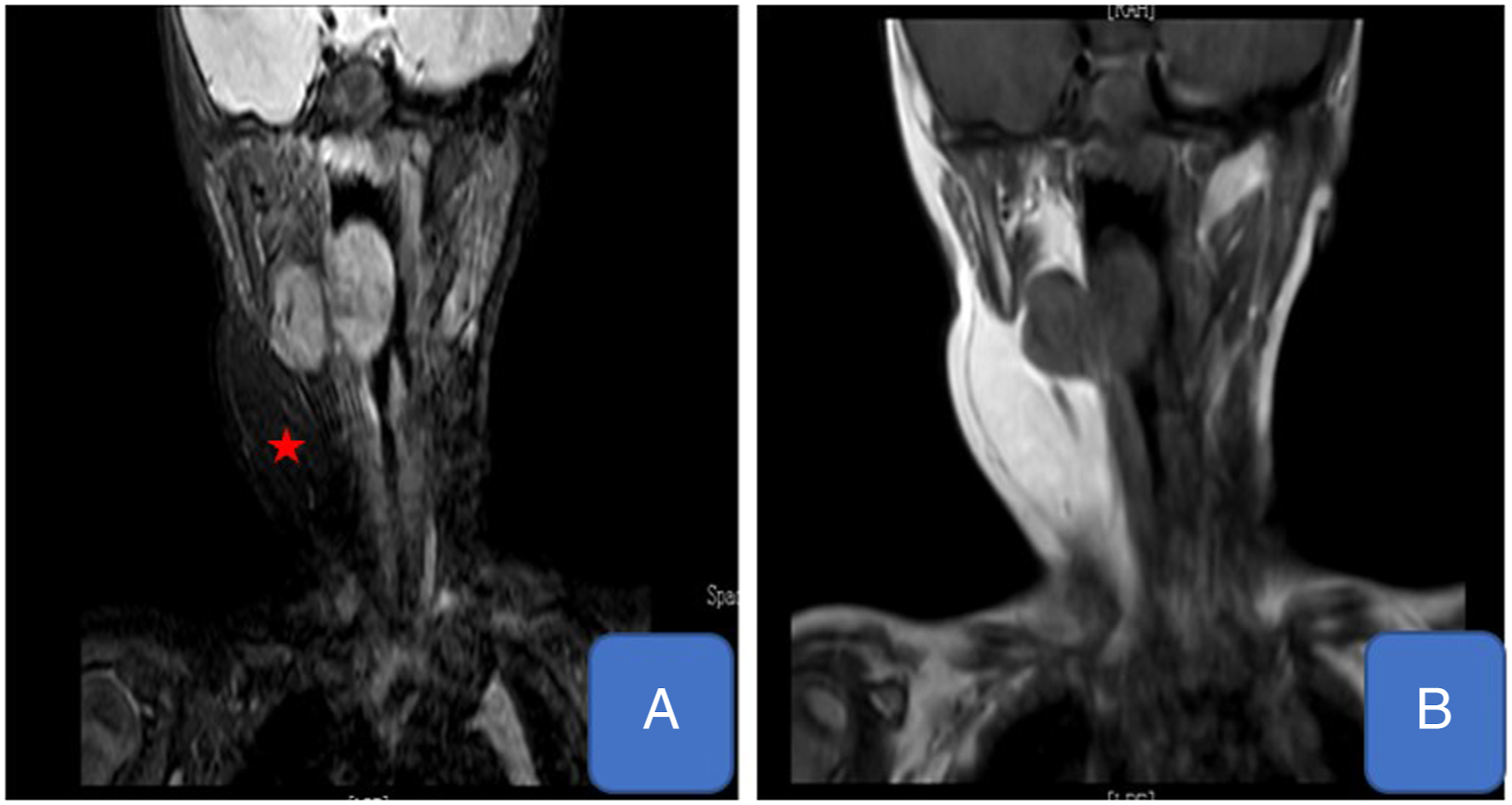
Based on the above imaging and clinical results, the mass was completely resected by adopting the transoral and transcervical approach.
The clinical protocol used for this case was established following the ethical guidelines of the Helsinki Declaration and was approved by the Human Ethics Committee of Shanghai Children’s Hospital, Shanghai Jiao Tong University. The parents or legal guardians of the two cases were provided with written informed consent for publication of the clinical data as well as images presented in this case report.
Discussion
Hemifacial hypertrophy is an uncommon congenital hemihypertrophy subtype, which was originally reported by Meckel in 1822.
1
Since then, numerous cases have been reported. The incidence of hemifacial hypertrophy among general population is approximately 1:86 000
2
and is more common in males, with a higher involvement rate of right side. Hemifacial hypertrophy can be categorized into partial and true hemihypertrophy, among which, the latter involved both soft and hard tissues. Moreover, Rowe et al
3
also classified congenital hemihypertrophy as follows: • Complex hemihypertrophy involving the whole half of the affected side or offside. • Simple hemihypertrophy involves one individual extremity. • Hemifacial hypertrophy is further divided into partial and true subtype, where the former involves heterogenous enlargement, and the latter involves all tissue enlargement.
In line with Rowe’s classification, the patient in the present study was classified as having partial hemifacial hypertrophy due to the involvement of partial facial muscles. MRI and CT scans revealed that bony structure was not asymmetric. It is essential to carefully check for the presence of abnormalities in the maxilla, tongue and mandible to make an appropriate diagnosis, especially for initial lipomatous overgrowth alone.
Hemifacial hypertrophy is usually used to interchange hemifacial hyperplasia. Based on histological nomenclature, the disorder is defined as hemifacial hyperplasia, in which cell number, but not cell size, increases in tissues. Therefore, “hemifacial hyperplasia” can better describe the pathology of this disease. 4
Hemifacial hypertrophy represents an uncommon developmental disease characterized by abnormal facial appearance, including facial enlargement and bone developmental abnormality. According to Khanna and Andrade, 5 because both the affected and unaffected sides grew proportionally, the relative disproportion was maintained. Based on Arora and colleagues, 6 asymmetry was aggravated over time. In our patient, congenital asymmetry was observed, which became increasingly significant since the affected side grew rapidly compared with with the unaffected side.
Rowe 3 investigated the dentition deformity on the affected side from 3 aspects, namely, root shape/size, crown size, and development rate. The authors also discovered the inconsistent involvement of teeth. The second molar and cuspids in the deciduous and permanent dentition, respectively, experienced the most frequent involvement, whereas the first molars and premolars ranked the second and third, separately. However, compared with the unaffected counterpart, no more than 50% of enlargement was observed. Rowe observed enlargement and thickening of alveolar bone on the involved side, which was usually away from the largest tooth. Uniform tongue enlargement is reported, which begins in the midline sharply. The excrescences are similar to the great fungiform papillae. Tooth and relevant mandibular hard tissue deformity have laid the important foundation for correct diagnosis, especially for facial hemihypertrophy.
Its etiology remains unclear, even though some factors are proposed recently. Hemihypertrophy has been identified to be the individual entity or one part in a syndrome. Although there is no study reporting the impacts of hereditary factors, its role is depicted in lymphatic/vascular deformity, central nervous system (CNS) diseases, neurocutaneous diseases, as well as endocrine diseases triggering the changed neurotrophic action. Hemihypertrophy is depicted within additional syndromes containing Russel–Silver syndrome, Proteus syndrome, Beckwith–Wiedemann syndrome, neurofibromatosis type 1, and Klippel–Trenaunay–Weber syndrome. Hemifacial hypertrophy shares some similar clinical signs with congenital facial infiltrating lipomatosis. Thus, it is hard to distinguish the two when no suitable histological examination is available.
This study presented one isolated hemifacial hypertrophy pediatric patient with no obvious abnormality in serum biochemistry or other physical examinations. Therefore, systemic disorders including neurofibromatosis type 1 and Klippel–Trenaunay–Weber syndrome, Beckwith–Wiedemann syndrome, Wilm’s tumor, and hyperpituitarism can be rapidly ruled out. Our patient presented with limited hypertrophy. Our patient was the first case of isolated hemifacial hypertrophy associated with unilateral tonsillar hypertrophy and parapharyngeal space lipoma. Right facial gross enlargement was the most obvious feature, with no obvious abnormality in teeth, tongue, or ear. Based on the findings of MRI and CT, subcutaneous tissue enlargement, unilateral tonsillar hypertrophy, and parapharyngeal space lipoma were the major causes of hemifacial hypertrophy, with no distinct facial bony abnormality.
Treatments range from mild contouring of soft tissues to massive surgical treatment in order to correct bony defect and reshape overlapping soft tissues. Moreover, surgical procedures are surgeries on soft and hard tissues. Condylar re-contouring, ostectomy, and osteotomy can be performed in combination to achieve the expected hard tissue shape. Afterward, soft tissue debulking may be obtained. Generally, condylectomy may not be needed while it was performed by Trapp. 7 Orthodontic treatment can be applied to correct occlusal deformity. In most cases, an aggressive surgery is avoided because relevant studies are lacking and the growth may be aggravated. In addition, it is difficult to recontour the entire half of the face, it remains uncertain about the exact amount of soft tissue to be reduced, and suboptimal esthetics after surgery may occur, although some sporadic studies have reported acceptable results. Therefore, it is necessary to try additional minimally invasive treatments. Recent advances in soft tissue contouring, such as liposuction, 8 have been made recently. The optimal indications for liposuction consist of adequate skin elasticity, sufficient subcutaneous adipose tissue for suction, and a little excessive skin. Besides, it remains to be evaluated concerning whether botulinumtoxin treatment and phosphatidylcholine preparations 9 may be the other options. This patient solved the problem only by removing too much soft tissue unilateral tonsillar hypertrophy and parapharyngeal space lipoma, and finally achieved good results, The children's faces were basically symmetrical during the postoperative follow-up, and the parents were also very satisfied with the postoperative effect.
For the long-run hemifacial hypertrophy treatment, the potential relation with childhood neoplasias and the outcomes must be kept in mind. Corrective surgical treatment at a suitable age along with psychological and sociological counseling is beneficial, which assists the patients in adapting to the environment. Nonetheless, more investigations are needed for clarifying the mechanism of aberrant growth of these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.