
Abstract
Congenital facial infiltrating lipomatosis (CFIL) is a rare condition that typically affects the trunk and limbs, but can also occur in the face. Managing CFIL is a significant challenge due to its diffuse involvement in important facial structures. This case report aims to describe a rare form of lipomatosis and discuss the clinical and therapeutic aspects of this entity. The patient was a 5-year-old girl who was admitted to our department due to a right paralateronasal swelling that had been present for 5 months. During the physical examination, a swelling of the right nasolabial was observed. A computed tomography scan of the facial bone revealed an extra bony soft tissue mass near the vestibule of the right nostril in contact with the frontal process of the maxillary bone and the anterior wall of the right maxillary sinus. The patient underwent excision under general anesthesia. The histological report indicated congenital focal lipomatosis. There was no recurrence of swelling a year after initial surgery. Facial infiltrating lipomatosis is a rare congenital disorder in which mature lipocytes invade adjacent tissue. Due to its diffuse infiltration and involvement of important facial structures, complete surgical excision is often impossible. Specific management of this condition requires insight into its pathogenesis as surgical removal of the mass is usually unsuccessful.
Introduction
Congenital facial infiltrating lipomatosis (CFIL) is a rare condition characterized by the presence of clusters of unencapsulated lipocytes that infiltrate surrounding soft tissues of the face, particularly the cheek and malar area, resulting in facial asymmetry. It is typically observed in early childhood and is more common in the trunk and limbs than in the face. 1 Managing CFIL clinically is a significant challenge due to its diffuse involvement of crucial facial structures. Until 2019, only 60 cases had been published in the English literature. 2
In this report, we present a case of CFIL with histopathological findings and a review of the literature. Our aim is to describe this rare form of lipomatosis and specify its clinical and therapeutic aspects.
Case Report
This report presents the case of a 5-year-old girl who had meningitis at a young age but did not experience any aftereffects. She was admitted to our department due to a right paralateronasal swelling that had persisted for 5 months. There were no relevant episodes during pregnancy, such as infectious disease, drug use, exposure to teratogenic agents, or difficult labor. Physical examination revealed a swelling of right nasolabial area of 2 cm on the main axis, which was firm and painless, and the overlying skin was normal. Examination of the oral cavity and oropharynx did not reveal any abnormalities, including dental abnormalities such as macrodontia or macroglossia. No facial paralysis was observed. The remaining ear, nose, and throat (ENT) examination was also normal. A computed tomography (CT) scan of the facial bone revealed an additional soft tissue mass near the vestibule of the right nostril, in contact with the frontal process of the maxillary bone and the anterior wall of the right maxillary sinus (Figure 1).
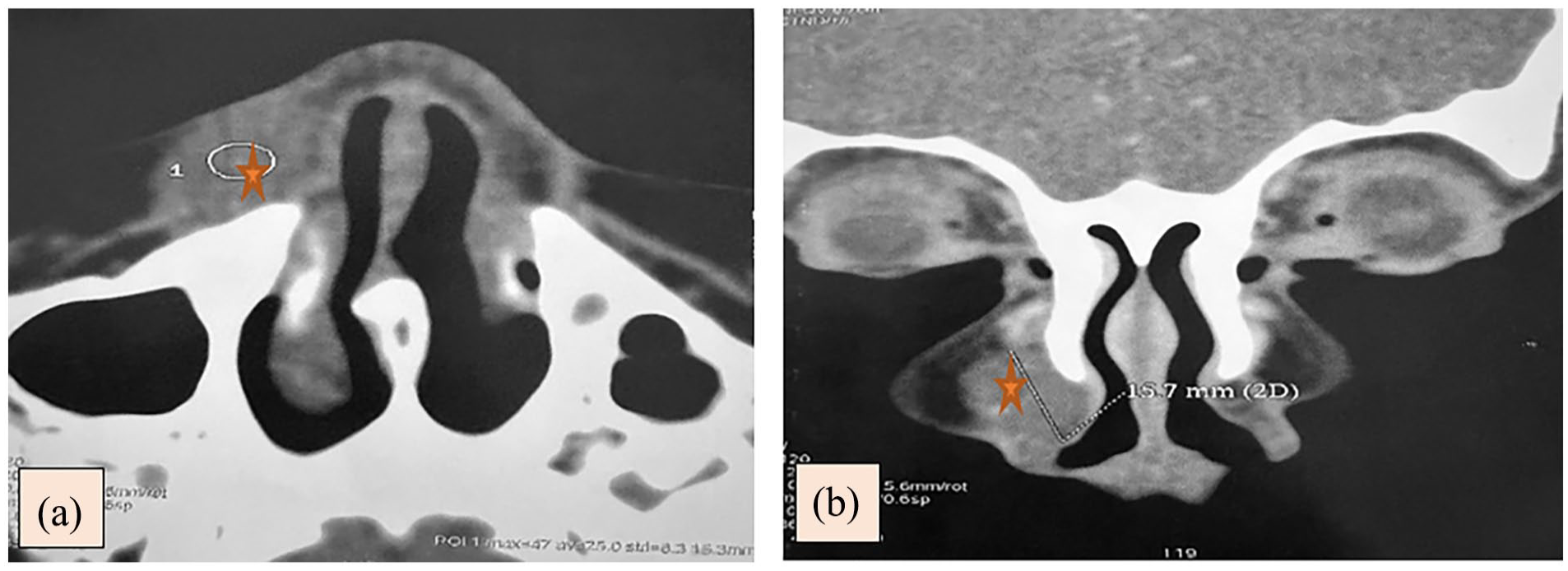
(a, b): CT scan of the facial mass in axial and coronal section showing an extraosseous soft tissue mass adjacent to the right nostril vestibule, in contact with the frontal process of the maxillary bone and the anterior wall of the right maxillary sinus, measuring 12 mm × 17 mm × 15 mm. CT, computed tomography.
The patient underwent excision under general anesthesia. Excision was carried out via the vestibular route, intraoperatively we found a focally hemorrhagic yellow to brown soft tissue adhering to the bone. Careful and slow dissection was performed to ensure complete removal of the mass and to preserve the integrity of the overlying skin and subcutaneous tissue. The dissection was deemed satisfactory. The definitive histology revealed the presence of lobules of mature adipocytes of varying sizes separated by fibrous septa, which dissociate the muscle fibers in some places. They surround hyperplastic nerve threads and thick-walled vessels, suggestive of congenital facial lipomatosis (Figure 2). There was no recurrence of the swelling 1 year after initial surgery.
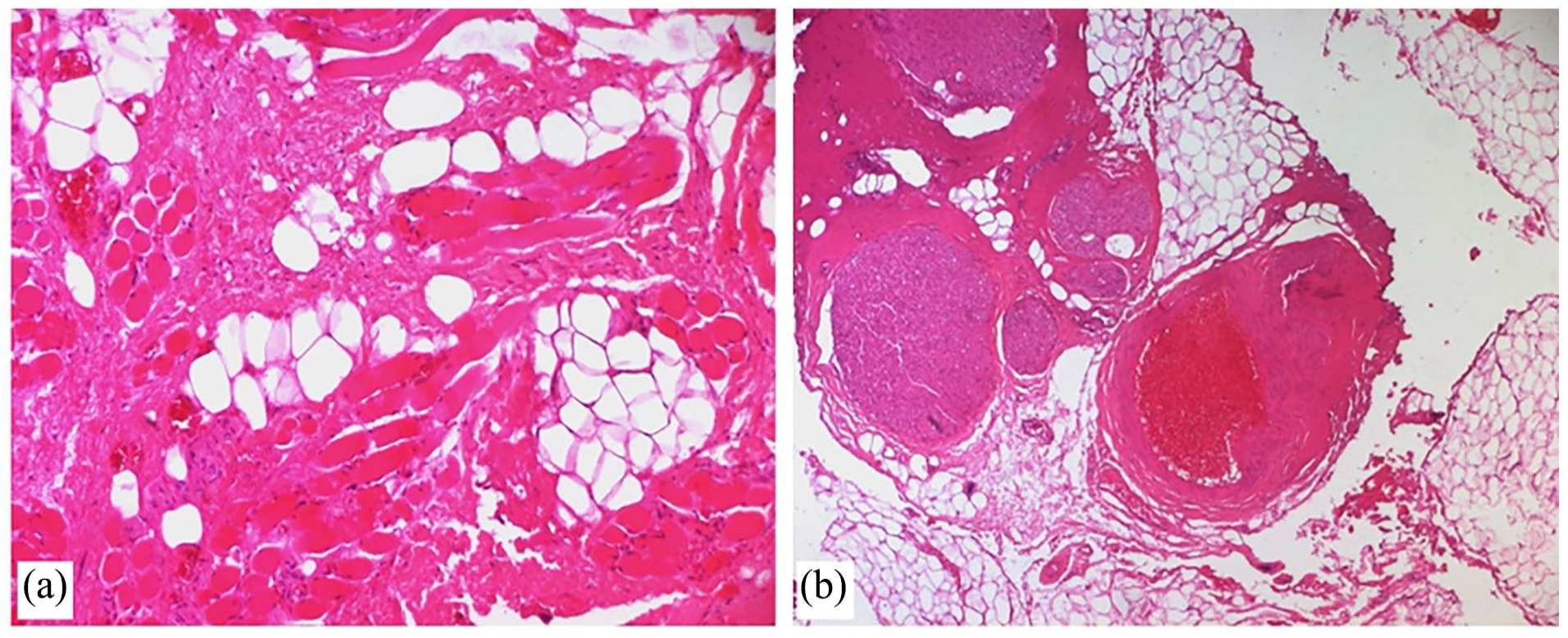
The specimen is made of lobules of mature adipocytes of variable size, separated by fibrous septa and dissociating striated muscle fibers (a, HE ×100), in places these lobules surround hyperplastic nerves and thick-walled vessels (b, HE ×50). HE, hematoxylin and eosin.
Discussion
The first case was described by Slavin et al in 1983, 3 and since then, almost 70 cases have been published in the English literature. CFIL is a rare congenital pathology, typically discovered after birth or in early childhood. 1 CFIL has no sex predilection. 4
The etiopathogenesis of CFIL remains controversial, and various theories have been suggested in the literature.
Capra et al reported a case of a girl with CFIL who had a deletion of chromosome 1q24.3q31.1. 5 Maclellan et al found a mutation in affected tissue of patients with CFIL that implicates the possible role of PIK3 in the lipomatous change. 6 Actually Oh et al 7 has demonstrated that PIK3, encoded by PIK3CA, plays a crucial role in regulating cell proliferation, adhesion, survival, and motility. This occurs due to postzygotic activating mutations in the PIK3CA gene, which constitute a part of the PIK3CA-related overgrowth syndrome. This causes mature lipocytes to invade adjacent tissues in the facial region. 7 Other authors have reported that somatic mutations in the PTEN and RET genes may also be the cause of CFIL. 8 Other cases have been suggested in the literature, including irradiation, trauma, muscular metaplasia, congenital cytomegalovirus infection, and degenerative fatty transformation. 9
Singh et al 8 suggest that this condition follows 2 patterns: a rapidly progressive form with early onset during the first year of birth and a more indolent form that progresses over decades, which is more likely the case for our patient.
The positive diagnosis of CFIL is based primarily on the clinical presentation and radiological findings.
Clinically, CFIL presents as a prominent, painless facial overgrowth and deformity on 1 side.1,2,5 The condition affects primarily mature adipose tissue that is not encapsulated, and can affect various areas of the face, including the cheeks, parotid glands, tongue, masticatory muscles, and lips. This can lead to hypertrophy of the underlying facial skeleton, including the maxilla, mandible, and zygomatic bone.2,9
CFIL may present with soft tissue and facial bone hypertrophy, as well as dental malformations such as macrodontia, poor root formation, accelerated tooth germ development, premature eruption of permanent teeth, and missing permanent teeth. 10 Our patient had no dental malformations.
Radiological examinations should aim to provide a positive and differential diagnosis of other conditions that cause hemifacial enlargement. 4
Panoramic radiography is useful for diagnosing dental malformations. 11 Panoramic radiography was not performed on the patient, as her dentition was adequate for her age. However, for radiographic diagnosis, CT scan and magnetic resonance imaging (MRI) are the most helpful tools.
CT scan is a useful tool for demonstrating the location and relationship of osseous changes and masses to surrounding structures. However, it may not always be conclusive in determining the lipomatous nature of a mass. In our case, although the nature of lipomatous nature was not determined on CT scan, we were able to identify its relationship with surrounding osseous structures. It is important to note that fatty infiltration can be inhomogeneous, which may be related to intervening fibrous elements. 11 Modern thin section scanners enable isometric 3-dimensional reconstruction, which is valuable for surgical planning. 4 However, MRI helps in tissue characterization and determination of the extent of the lesion. 4 It is crucial to demonstrate the thin capsule and differentiate it from surrounding normal fat. 4 A lack of contrast enhancement on MRI rules out the possibility of a malignant cause. 12 Ultrasonography reveals adipose tissue but cannot fully define the lesion. 13
Histomorphological findings are the following: (1) mature adipose tissue that infiltrates adjacent muscles and soft tissue without encapsulation, (2) the presence of fibrous components, numerous nerve bundles, and vessels with thickened walls, as described in our study, (3) rapid growth causing hypertrophy of the underlying bone without malignancy, (4) a high tendency for postsurgical recurrence, and (5) the presence of fibrous elements and absence of lipoblasts or malignancy characteristics.2,3
Unilateral facial swelling can be caused by various diagnoses, including lipoma, vascular malformation, hemangioma, liposarcoma, lipoblastomatosis, and other overgrowth syndromes. It is important to note that subjective evaluations have been excluded from this analysis. However, CT and MRI can easily eliminate vascular malformation or hemangioma. 2
Another potential differential diagnosis to consider is hemifacial hyperplasia (HFH), which is a congenital deformity that causes unilateral facial enlargement and involves multiple tissues. 2 HFH is typically characterized by hyperplasia rather than hypertrophy, as the increase in cell number is more significant than the increase in cellular volume. 2
Encephalocraniocutaneous lipomatosis and Proteus syndrome may also be considered as potential differential diagnoses. 9
In this case, the differential diagnosis was based on various factors. Lipoma, which is an encapsulated tumor with thin fibrous strands, was considered but excluded due to the diffuse fatty infiltration that appeared unencapsulated. Lipoblastomatosis was also ruled out as it typically presents with lipoblasts and signet ring cells. The presence of bony hypertrophy and remodeling suggests a chronic process and malignancy was excluded based on the patient’s long clinical history. Liposarcoma was excluded due to the absence of lipoblasts and pleomorphism on histopathology. Cutaneous signs are typically present in diseases such as infiltrating angiolipoma or facial angioma. After eliminating these differential diagnoses, we diagnosed CFIL based on clinical presentation, CT findings, and histopathological findings.
Treating CFIL remains a challenge due to the lack of clarity regarding the timing and technique of treatment. Treating CFIL remains a challenge due to the lack of clarity regarding the timing and technique of treatment. Treating CFIL remains a challenge due to the lack of clarity regarding the timing and technique of treatment. There is no consensus among the authors regarding the preferred treatment modality.3,9,10
Early study by Slavin et al 3 recommended aggressive resection during childhood to improve facial appearance and control overgrowth.
Chen et al 14 argue in favor of delaying radical surgical treatment due to the high recurrent rate and the increased risk of facial nerve injury. The recurrent rate of CFIL was ranged from 27.3% to 62.5% after the first surgery in early childhood. 14
In addition, Couto et al 15 suggest that growth hormone may play a role in recurrences. It was believed that attempting to reduce the mass before the end of adolescence was likely unsuccessful. This is in agreement with the findings of Jaiswal et al, who advocated for definitive excision and reconstruction during adolescence to minimize the risk of facial nerve injury and to allow for maturation and better matching of the contralateral cheek contour. 4
Li et al recommend conservative treatment, such as liposuction, for young patients with minimal risk. 16 Kalantary et al 17 propose a multistep surgical approach that begins with initial debulking to correct soft tissue asymmetry, followed by orthognathic surgery to correct skeletal asymmetry, dental problems, and associated malocclusion. 17 The CFIL is characterized by its recurrence and patient management requires multidisciplinary collaboration and multistage surgical intervention. 1
Conclusions
The diagnosis of CFIL should be considered based on clinical examination and confirmed by characteristic radiological findings. Regular observation of the patient is necessary until bone growth stabilizes, after which appropriate cosmetic surgery should be performed. This disease is noteworthy for its complex etiology, the significant damage it causes to facial appearance and function, and the limitations of the curative approach.
Footnotes
Acknowledgements
None.
Data Availability
Data will be made available on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval is not applicable for this article.
Informed Consent
There are no human subjects in this article and informed consent is not applicable.