
Abstract
Warthin’s tumors of the head and neck are more common in the parotid and salivary glands and are extremely rare in the nasopharynx. This paper reports the clinical data of a patient with a nasopharyngeal Warthin’s tumor and posterior nostril atresia who underwent nasal endoscopic nasal mass resection combined with posterior nostriphoplasty, and the patient has no tumor recurrence during the postoperative follow-up of until 14 months. This case report, combined with a literature review, conducted an in-depth analysis of nasopharyngeal Warthin’s tumors to enable more otolaryngology specialists to deepen their understanding of such diseases.
Introduction
Warthin’s tumor, also known as adenular lymphoma or lymphatic papillary cystadenoma, was first described by Hilderbrand as a congenital neck cyst in 1895, and in 1929 by Warthin as papillary cystadenoma lymphoma. 1 It is more common in the parotid gland and salivary gland, especially in the parotid gland, and it occurs very rarely in the nasopharynx. The available data on nasopharyngeal Warthin’s tumor are scattered cases, and there is no clear conclusion on the possible factors of the occurrence in the nasopharynx. This paper reports the diagnosis, treatment process, and follow-up results of one patient with a nasopharyngeal Warthin’s tumor, and analyzes the literature to provide an important literature basis for the diagnosis and treatment of similar cases in the future.
Case Description
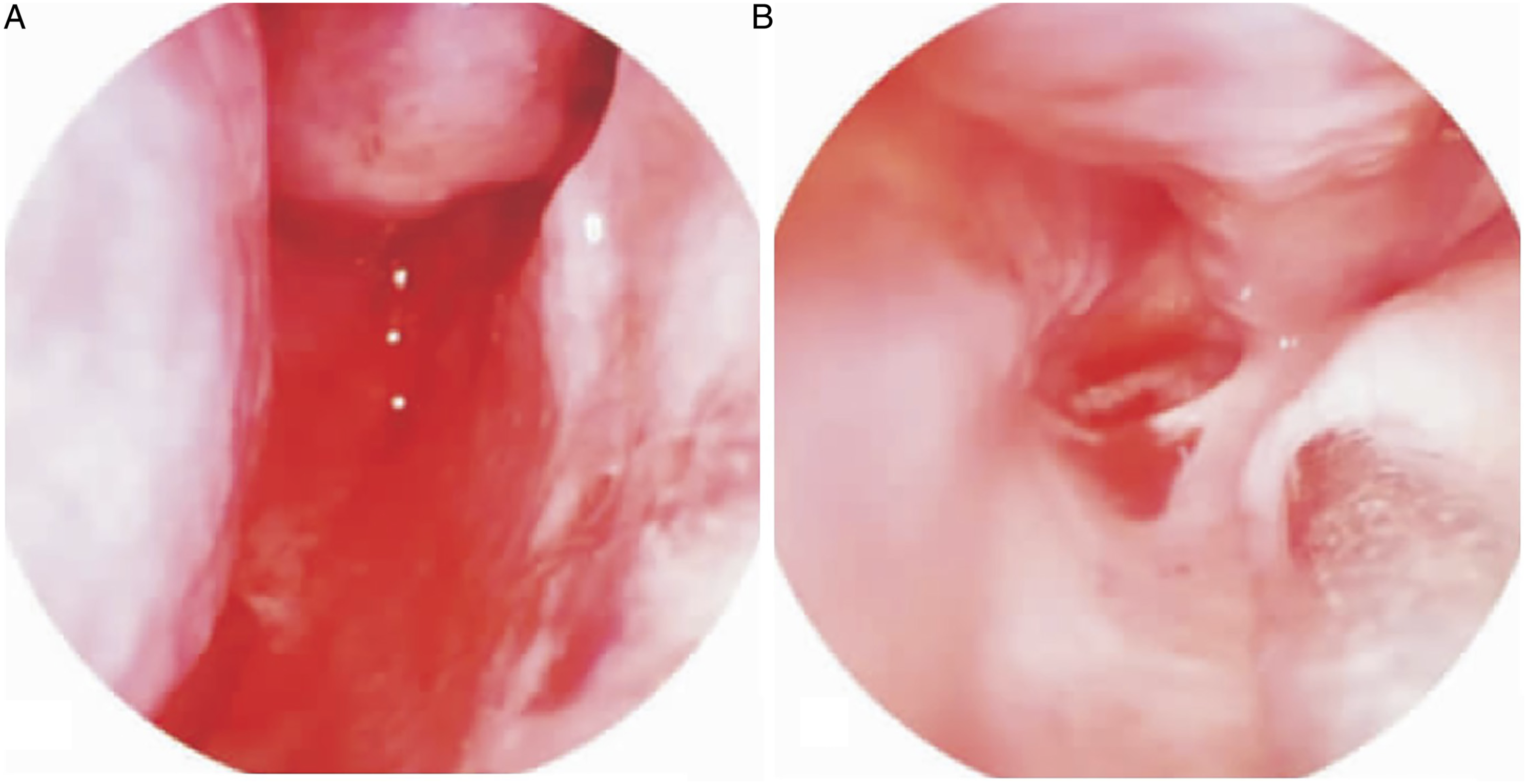
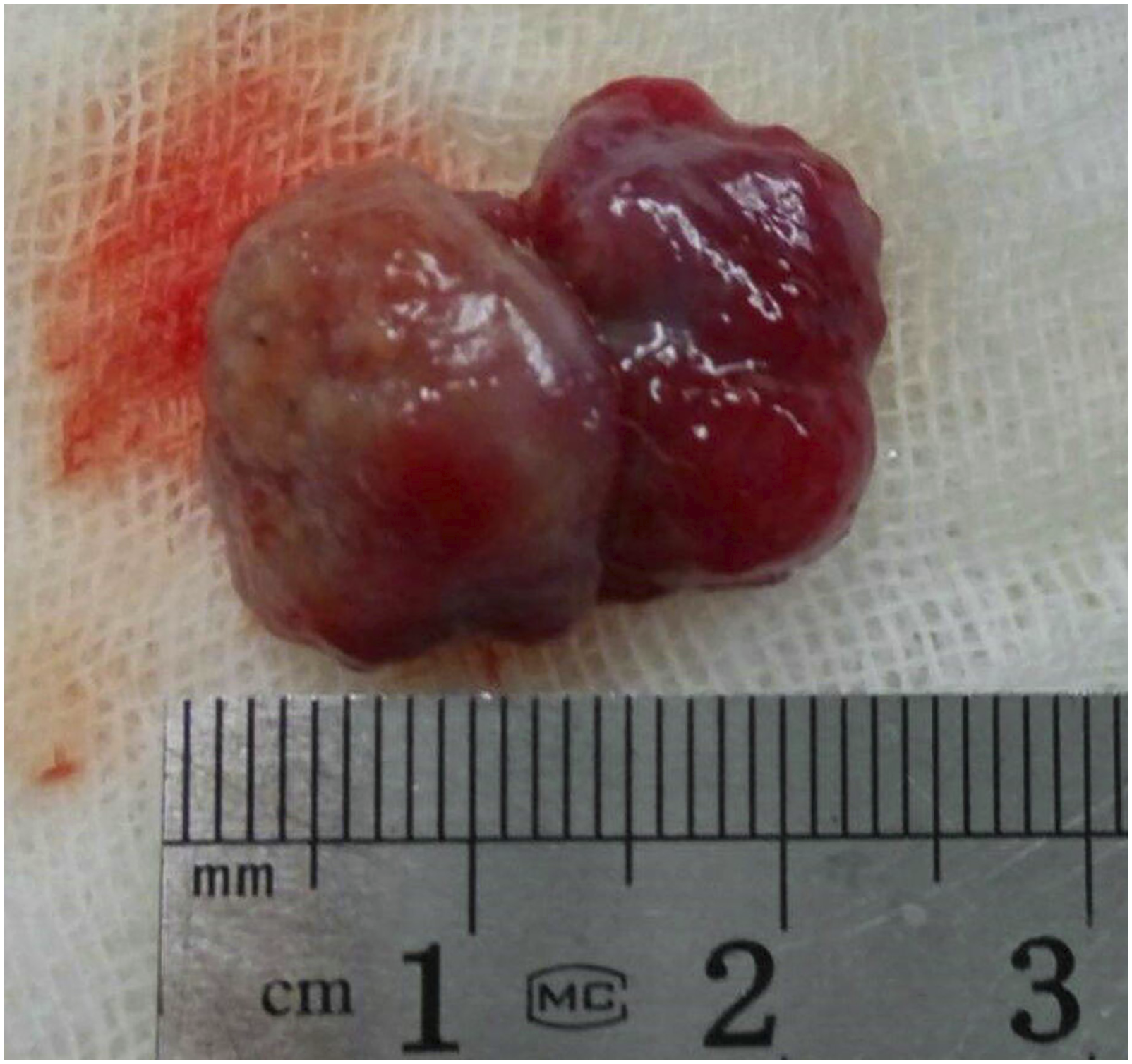
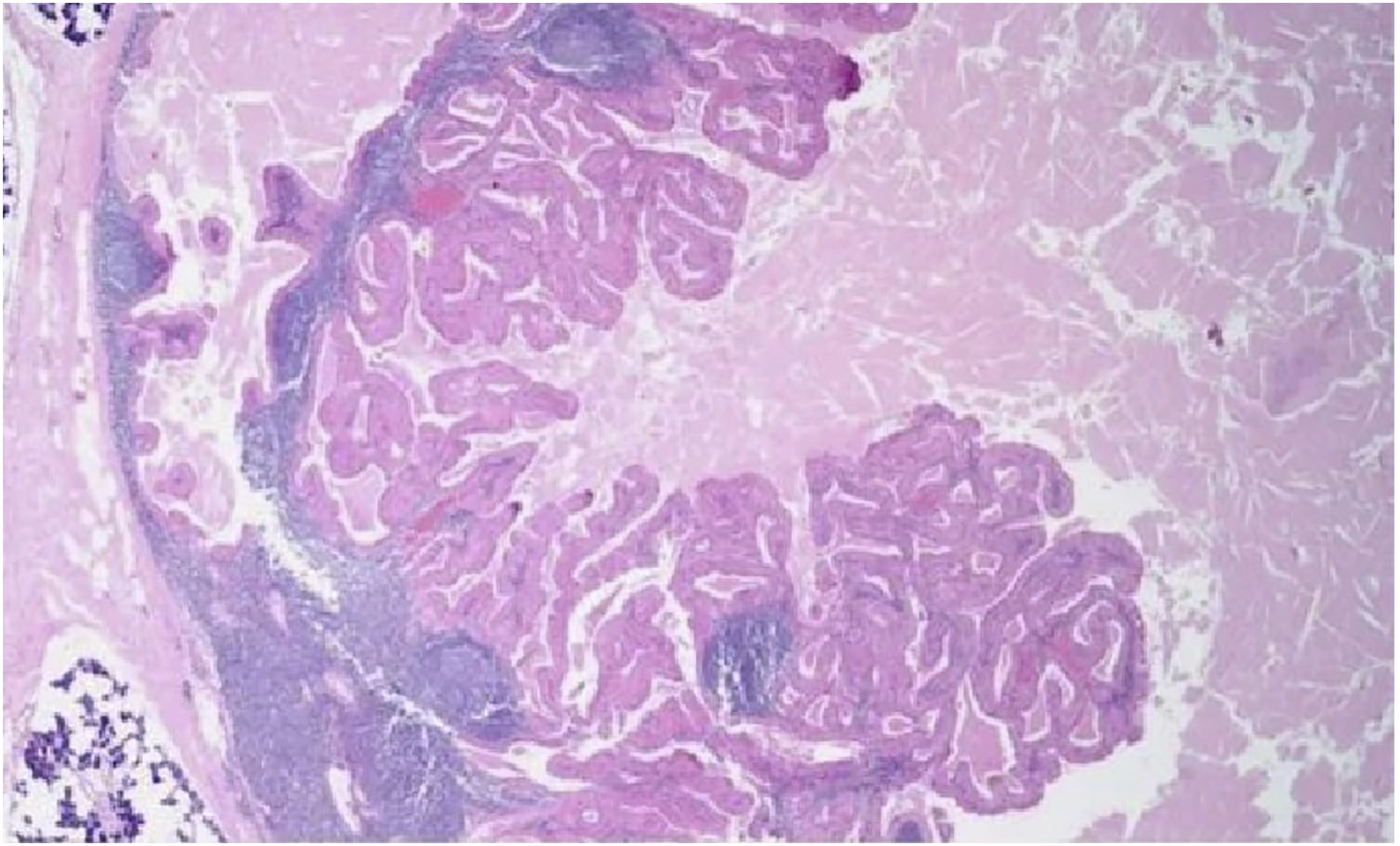
A 58-year-old female patient developed bilateral nasal congestion and purulent discharge after a cold 9 years prior. The right side was severe, and conservative treatment was ineffective. Her symptoms were significantly aggravated in the prior 2 years, and there was persistent nasal congestion on the right side. She came to the hospital in June 2020. Physical examination showed that she had more purulent discharge in the bilateral nasal cavity. After cleaning, the posterolateral wall of the right nasal cavity was noted to be bulging to the medial side and was adhered to the septal mucosa, and the posterior nostrils were completely closed. Computed tomography (CT) showed a right bulge of the sinus throat with an inward adhesion to the nasal septum, complete posterior nose closure, and narrow left posterior nostrils (Figure 1). Nasal endoscopy indicated a complete obstruction of the right posterior nose and left posterior nose stenosis (Figure 2). There were no laboratory abnormalities. During surgery, descending nasal mass resection combined with bilateral posterior nostrioplasty was performed, the right posterior nostrils were completely closed, and the posterior nostrils were opened from the septum with an electric knife. Then the new posterior nasal mass (Figure 3) was removed laterally, releasing the left posterior nostril adhesion, which expanded the posterior nostrils, and a bilateral nasal expansion sponge was used. The postoperative pathological results suggested that the right posterior nose tissue was a lymphatic papillary cystadenoma (Figure 4). The patient was discharged 5 days after surgery and was followed up until 14 months without recurrence. Cranial CT indicated that the right posterior nostril was blocked by a mass and that the left posterior nostril was narrow. Nasal endoscopy: A. complete obstruction of the right posterior nostrils; B. left posterior nostril stenosis. Removed lesion. Pathological examination: lymphatic papillary cystadenoma (HE×100).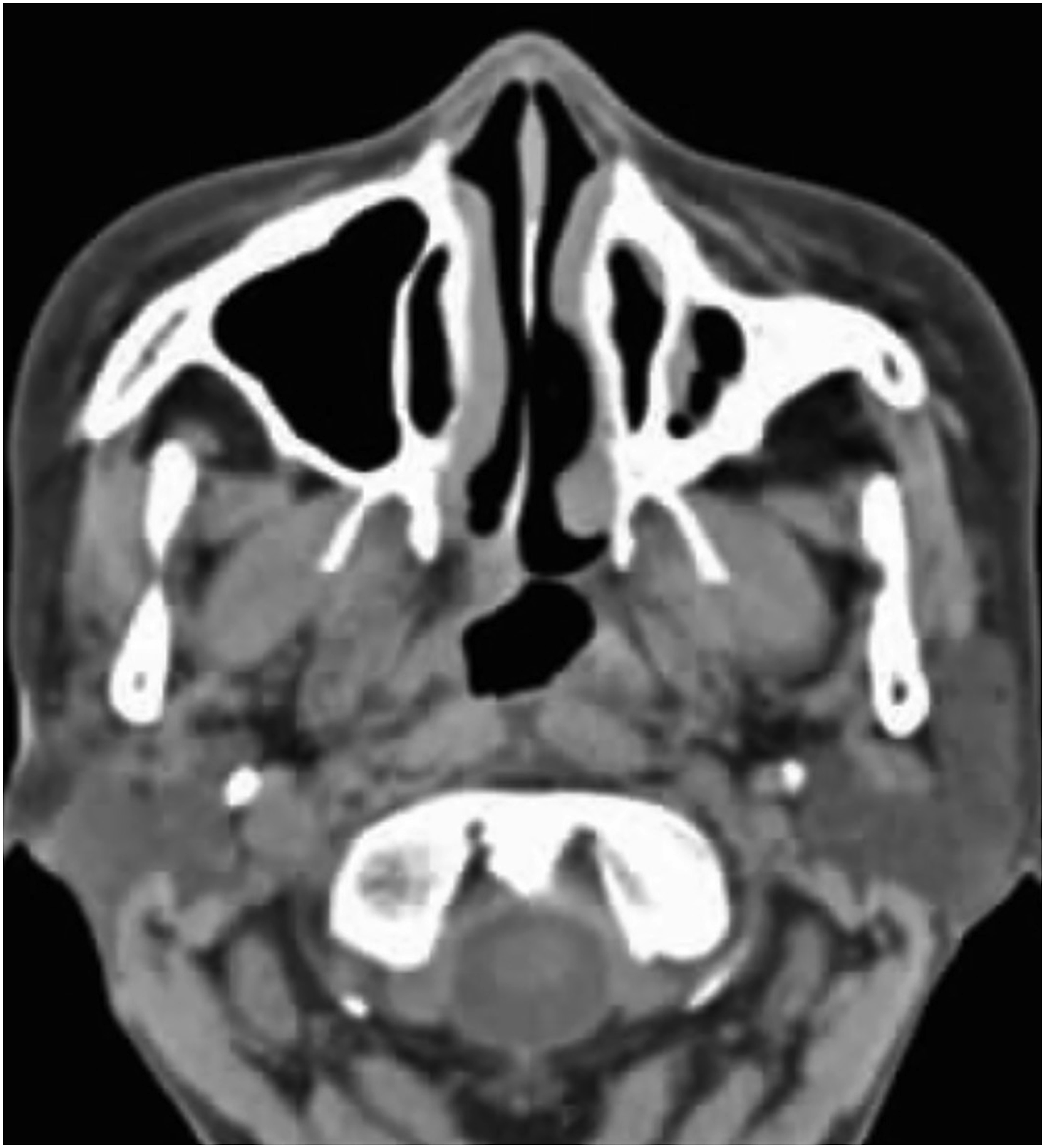
Discussion
Epidemiological Characteristics
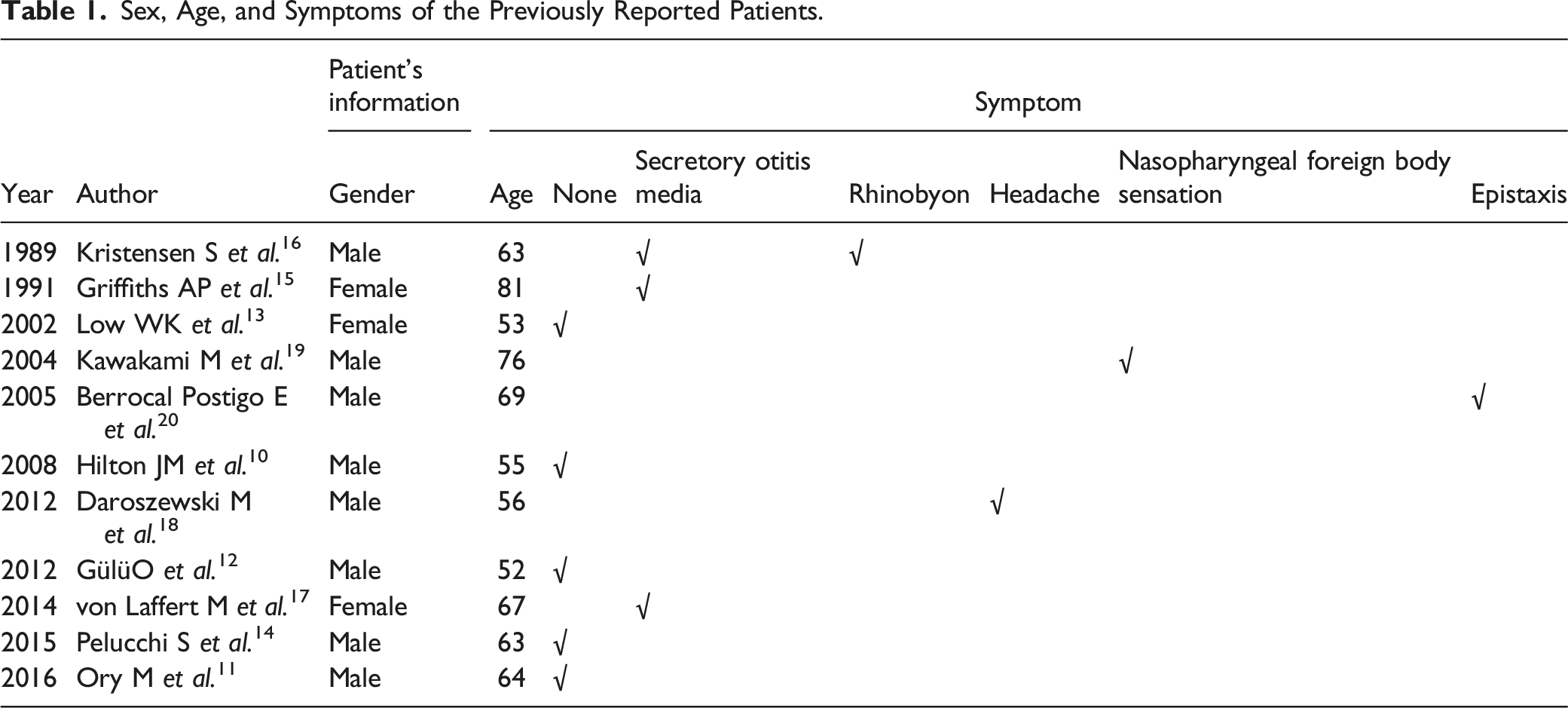
Warthin tumors are benign salivary gland benign tumors, and their incidence is increasing year by year, more than 90% occur in the parotid gland. Most data show that they are benign tumors, and it accounts for 5%−6% of the parotid tumors, and their incidence is higher in males than in females and in smokers.2-5 Kadletz et al. 6 also pointed out that Warthin incidence and metabolic syndrome may be linked, especially in patients with obesity. European scholars have proven that Warthin tumors in recent years extend beyond pleomorphic adenoma as the first parotid benign tumor. 7 Chinese scholars analyzed 3724 cases of salivary gland tumors and showed that more than 99% of the salivary gland Warthin tumors are in the parotid gland, the sex ratio is approximately 4:1, prone to occur in patients aged between 40 and 70 years, and the incidence of this tumor has tended to increase in the last 10 years. 8 The 1084 cases of Warthin tumors in east China show that the sex proportion is 11:1, the incidence of multifocal Warthin tumors is 9.5%, 28 of the tumors occurred outside the parotid gland, and none of the tumors were located nasopharynx. Thus, nasopharyngeal Warthin tumors are quite rare. 9 In the published literatures, 11 nasopharyngeal Warthin tumors10-20 have been reported since 1989, as well as 12 more cases. The onset was generally when the patients were 52–81 years old, there were 8 males and 4 females (2:1), average age is 63.08 years old, among which 3 male patients had a clear history of heavy smoking and 5 patients had parotid gland lymphoma (41.7%).
Clinical Symptoms
Sex, Age, and Symptoms of the Previously Reported Patients.
The Origin of the Tumor
There is no consensus on the source of nasopharyngeal Warthin tumors, but some are thought to originate from the small sporadic salivary glands in the nasopharynx and others may originate from metaplasia.10,15,16,18,20 Recently, Valstar et al. 21 found through PET-CT that another large salivary gland is distributed in the convex area, and they called it the convex salivary gland. The nasopharyngeal dry discomfort caused by radiation therapy may be related to the irradiation of this gland. All three of the reported nasopharyngeal Warthin tumors and the other 9 were all located in the lateral wall of the nasopharynx. Currently, it remains controversial whether convex salivary glands are present. 22 Assuming that the convex salivary glands do exist and according to the characteristics of Warthin tumors in the salivary glands, and most of the nasopharyngeal Warthin tumors are located in the lateral wall of the nasopharynx, and we speculate that Warthin tumors in the nasopharyngeal lateral wall are related to the convex salivary glands. However, do the tumors occur in the convex salivary glands? Because the concept of the presence of salient salivary glands have been put forward in recent years, it still needs more case studies are needed to confirm these glands. If the possibility of the convex salivary gland can be considered before surgery, the intraoperative resection can be expanded, and the pathological confirmation that the tumor is located in the gland is more convincing. What occurs in the top wall may be related to small sporadic salivary glands.
Diagnosis
According to the analysis of the existing data, the tumor should grow relatively slowly, and it is difficult to detect this tumor when it is asymptomatic in the early stage. The diagnosis can be considered from the following aspects: (1) clinical manifestations: nasopharyngeal foreign body sensation, secretory otitis media, nasal congestion, headache, etc.; (2) endoscopy: on endoscopy, a smooth swelling may be found on the nasopharyngeal surface, there could be thickening of the nasopharyngeal mucosa caused by posterior nasal stenosis and closure signs, and some patients can have middle ear effusion signs; (3) imaging: CT or MRI may be more valuable for disease diagnosis. Unfortunately, this patient did not have an MRI examination, which resulted in imperfect data, and the lack of MRI in this case is related to our lack of understanding of this patient’s disease; and (4) pathology: the final diagnosis still depends on pathological confirmation.
Treatment and Prognosis
The current treatment of the disease is mainly caused by surgical resection. With the innovation of surgical instruments and the progress of endoscopic technology, the lesions can be well exposed and removed under nasal endoscopy. This patient case had no recurrence after 14 months of follow-up. According to the available data, the length of postoperative follow-up varied, but no recurrence was reported, suggesting that surgical resection of nasopharyngeal Warthin tumors is a better treatment.
Conclusion
Nasopharyngeal Warthin tumors are clinically rare and mostly occurring in middle-aged and elderly men, and approximately 41.7% of these patients present with concurrent parotid gland lymphoma. The tumor grows slowly and has no clinical symptoms in the early stages, so early detection is more difficult. In addition to nasal congestion, approximately 1/4 of these patients have secretory otitis media. Most of these tumors are located in the lateral wall of the nasopharynx. The treatment is mainly surgical resection, which can be completed under nasal endoscopy, and the long-term prognosis is good.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The report of this case was approved by the ethical committee of the Tianjin Huanhu Hospital.
Data Availability
Except for the patients’ privacy, some fields in data are available for scientific researchers upon reasonable request through the first or corresponding author.