
Abstract
Objective
A variety of approaches for resection of the ossifying fibromas in sinonasal cavities have been described. However, for those involving the anterior skull base, endoscopic surgery remains challenging because of limitations in identification of tumor boundaries from the anterior skull base and proper control of the tumor-feeding vessel. This study aimed to describe a technique for resection of ossifying fibromas involving the anterior skull base through an endoscopic endonasal trans-agger nasi approach, based on anatomic studies and surgeries.
Methods
Two human cadaveric heads were prepared for study of the anatomic relationship between agger nasi and anterior skull base. Two clinical cases were used to illustrate the technique and feasibility of the approach.
Results
The agger nasi was located anterior and inferior to the frontal ostium and the anterior skull base. The frontal ostium and anterior skull base could be visualized and accessed under the 0-degree endoscope by removing the agger nasi. Application of the endoscopic endonasal trans-agger nasi approach in the two patients resulted in complete resection of the tumors with no surgical complications.
Conclusions
An endoscopic endonasal trans-agger nasi approach provides a direct access to the anterior skull base. It would be feasible, effective, and safe for selected cases of ossifying fibroma involving anterior skull base.
Introduction
Ossifying fibromas are relatively rare fibro-osseous lesions that often occur in the bones of the craniofacial skeleton, such as mandible and maxilla. 1 According to the World Health Organization report, ossifying fibromas are histologically characterized by the replacement of normal bone by fibrous tissues that contain varying amounts of mineralized material and cementum.2-4 Ossifying fibromas are typically slow-growing, but potentially locally aggressive. 1 Although rare, this tumor can also occur in the sinonasal cavities, skull base, and orbit.2,3,5 It has been reported that ossifying fibromas commonly occur in the second to fourth decades of life and to be more common in women. Sinonasal tract ossifying fibromas reportedly occurs slightly later in life and more commonly in African American females.1,2,4,6
Surgery is the mainstay for the treatment of ossifying fibromas. The overall goal of surgery is complete removal of the lesions with minimal morbidity. Recently, with the introduction of endoscopic techniques, several studies have demonstrated the safety and feasibility of the endonasal endoscopic approach for resection of the tumors.7,8 However, for those occur in the sinonasal cavities and involve the anterior skull base, endoscopic surgery remains a challenge for otolaryngologists. First, it is difficult to identify the boundary of the lesions from important surrounding structures. Second, ossifying fibromas are usually highly vascularized. A rapid and proper control of the tumor-feeding vessel is crucial to minimize intraoperative hemorrhage.7,8
Agger nasi is a small ridge on the lateral side of the nasal cavity and located at the anterior edge of the middle nasal concha, directly above the atrium of the middle meatus. 9 With an in-depth understanding of the anatomic relationship between agger nasi and frontal recess and sinus, the trans-agger nasi approach and its variations have been used for the removal of lesions of frontal recess and sinus.10-14 Herein we extend previous work to describe the anatomic relationship between agger nasi and anterior skull base in an anatomic study, and first present our clinical experience in the management of two selected ossifying fibromas involving anterior skull base to demonstrate the technical nuances of the endoscopic endonasal trans-agger nasi approach.
Materials and Methods
The Ethics Committee of the Seventh Affiliated Hospital of Sun Yat-sen University does not necessarily request the application of ethical approval for this type of manuscript. All aspects of the study were conducted according to the Declaration of Helsinki.
Two formalin-fixed human cadaver heads (four sides) were used for anatomic study. Two selected patients with ossifying fibroma involving anterior skull base were evaluated and underwent endoscopic endonasal trans-agger nasi approach for resection of the tumor in the Department of Otolaryngology, the Seventh Affiliated Hospital of Sun Yat-sen University. Instruments (Richard-Wolf Endoscopy, Germany) were used for endoscopic endonasal surgeries.
Results
Anatomic relationship between agger nasi and anterior skull base
From an endoscopic view as shown in Figure 1A, agger nasi is located at the anterior edge of the anterior attachment of the middle turbinate with a mucosal membrane covering the ethmoidal crest of maxilla. To facilitate understanding of the anatomic relationship between agger nasi and anterior skull base, sagittal dissection along the line of cribriform plate was made. In the sagittal view, the lateral wall of the nasal cavity contained all the structures of this anatomic area, including middle turbinate and meatus, agger nasi cell, uncinate process, and ethmoidal bulla (Figure 1B and 1C). Agger nasi was identified anterior and superior to the middle turbinate attachment. After removing the vertical portion of the middle turbinate, the upper parts of the uncinate process and the ethmoidal bulla were identified posteriorly (Figure 1C and 1D). After the agger nasi was dissected, as well as complete removal of the middle turbinate attachment, the upper parts of the uncinate process and the ethmoidal bulla were fully exposed (Figure 1D). After removing the uncinate process and the ethmoidal bulla, the relation between agger nasi and anterior skull base, lamina papyracea and frontal ostium was revealed. The agger nasi was located anterior and inferior to the frontal ostium and the anterior skull base (Figure 1E). As indicated in Figure 1D and 1E, after removal of agger nasi, the structures of the frontal ostium and the anterior skull base could be visualized by endonasal trans-agger nasi approach under the 0-degree endoscope. Anatomic relationship between agger nasi and anterior skull base. The round circle indicates the agger nasi area on the lateral wall of nasal cavity. Schematic drawing shows the endoscopic trajectory to the anterior skull base through the endonasal trans-agger nasi approach. AN, agger nasi; MT, middle turbinate; NS, nasal septum.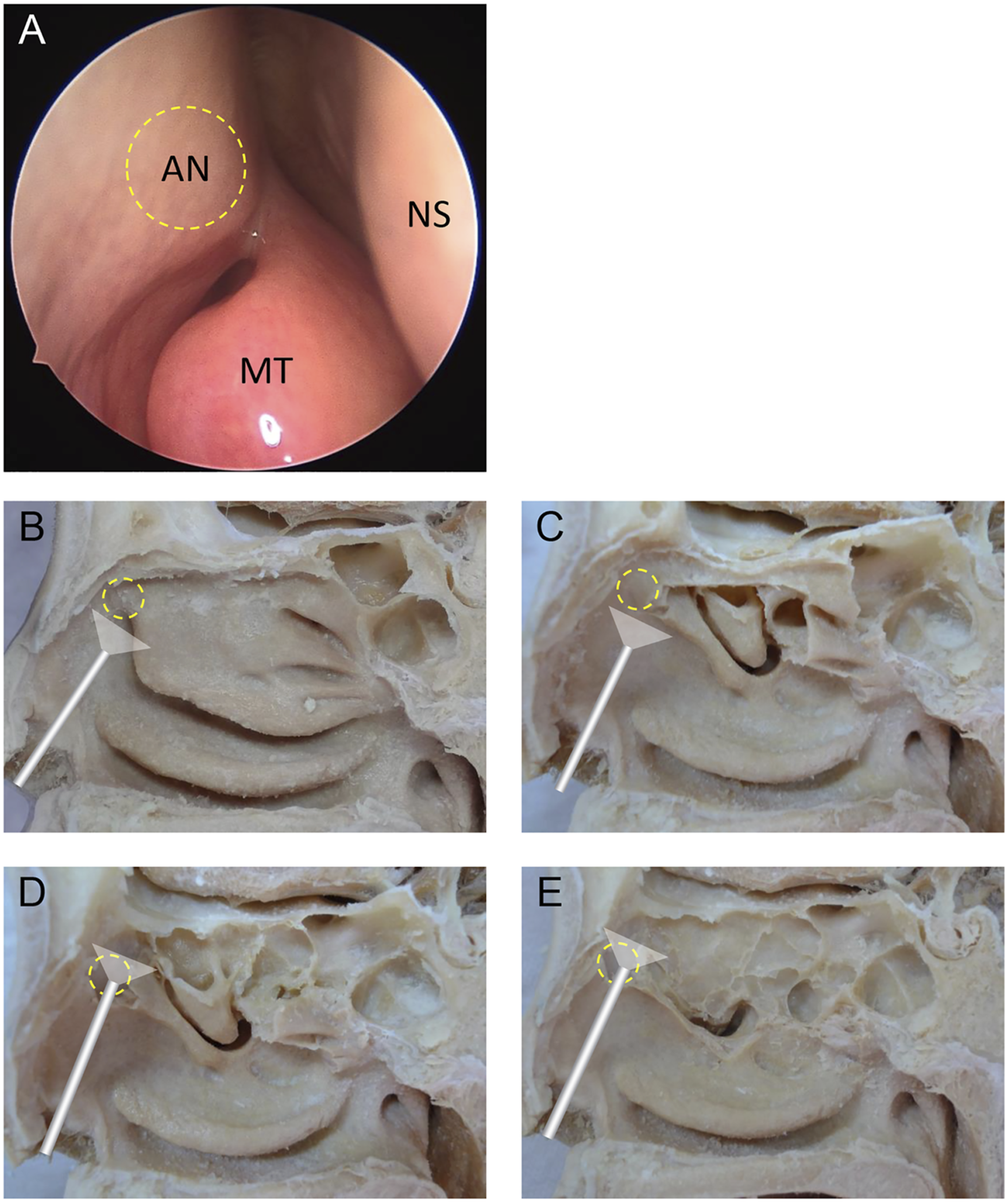
Surgical Technique of Endoscopic Endonasal Trans-Agger Nasi Approach (Example of Case 1)
All surgical procedures were performed with the patient in the supine position under general anesthesia and orotracheal intubation. The nasal cavity was decongested with 1:10,000 adrenaline-soaked cotton pledgets. The agger nasi on the lateral wall of the left side nasal cavity was identified (Figure 2A). First, an inferiorly based full-thickness mucosal flap was created starting the insertion of the anterior middle turbinate to the roof of the nasal cavity and running anteriorly and inferiorly around the agger nasi (Figure 2B-C). The flap could be pushed inferiorly and stored at the level of the inferior turbinate until the completion of the operation. Then, the bony wall of the agger nasi and the frontal process of the maxilla were drilled and removed with a Kerrison rongeur, superiorly to the frontal ostium and laterally to the medial wall of orbit (Figure 2D-F). After identification of the frontal ostium and the anterior skull base, the tumor was dissected from the adjacent tissues after careful separation along the tumor boundary and the anterior skull base (Figure 2G-K). At the end of the procedure, the flap was repositioned to the original position (Figure 2L). The above steps could be easily completed under the 0-degree endoscope. Surgical procedures of case 1. The round circle indicates the agger nasi area. The yellow arrow indicates the opening of frontal sinus. The dash line indicates the anterior skull base. t, tumor; f, flap.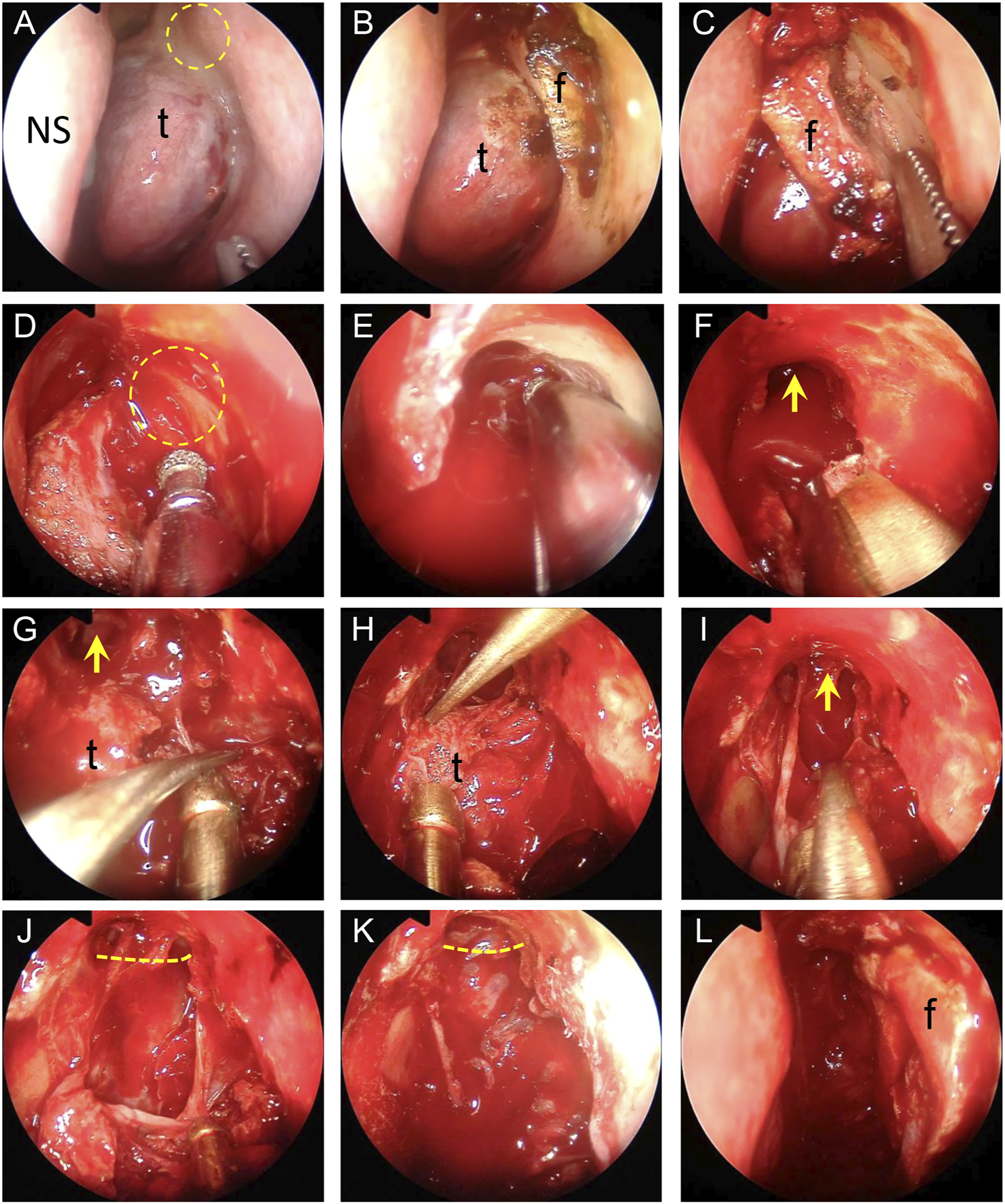
Illustrative Cases
Two selected patients with ossifying fibroma involving anterior skull base were included in this study. They underwent endoscopic endonasal trans-agger nasi approach for tumor resection. Preoperative assessment was based on nasal endoscopy and computed tomography (CT). The patients were adequately informed about the surgical procedures, surgical risks, and potential alternatives and written informed consent was obtained from all patients. Postoperative CT was obtained within the first postoperative month to evaluate the extent of resection. Postoperative nasal endoscopy was regularly employed.
A 55-year-old man presented with nasal obstruction. CT of the paranasal sinuses showed an expansile mixed radiolucent-radio opaque mass expanding the left ethmoid sinus and involving the anterior skull base with bulging onto the medial orbital wall. A dorsal extension up to the basal lamella of middle turbinate was seen. The mass showed a rim of irregular thickened bony structures. The central areas of the lesion contained coarse calcifications as well as hypodense soft tissue densities (Figure 3A-C). The endoscopic endonasal trans-agger nasi approach was performed on the patient. After the dissection of the agger nasi, the anterior and upper edge of the tumor was identified. Then, the tumor was removed from top to bottom. En-bloc tumor excision was accomplished (Figure 3D). During the procedure, we found that the anterior ethmoid artery was located behind the tumor along the skull base and did not disturb the resection procedure. Thus, we did not control the artery. Postoperative CT images indicated the complete resection of the tumor (Figure 3E-G). The final histological examination confirmed the diagnosis of ossifying fibroma. Postoperative nasal endoscopy showed a well-healing wound with no sign of infection at 1-month post-operation (Figure 3H-I). During the clinical follow-ups conducted at 12-month after the surgery, a nasal endoscopy showed no sign of tumor recurrence and the patient remained symptom-free.
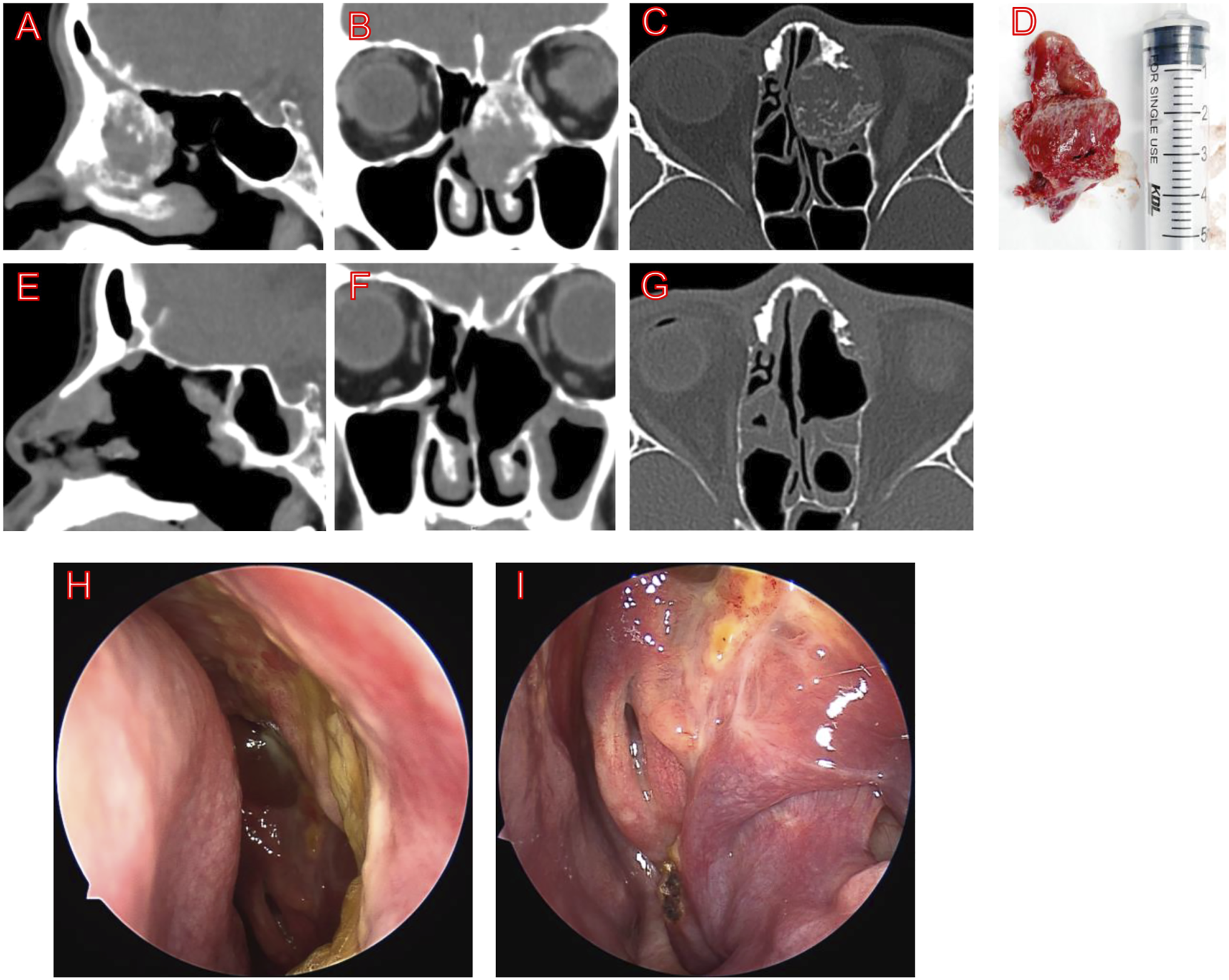
Preoperative and postoperative examination of case 1. (A–C) Preoperative CT images. (D) Surgical specimen of the tumor. (E–G) Postoperative CT images. (H–I) Postoperative nasal endoscopy at 1-month post-operation.
A 25-year-old female patient with previous endoscopic sinus surgery for an ossifying fibroma and repeated left-sided headache. The postoperative course was uneventful, but CT showed a remnant ossifying fibroma involving anterior skull base. 15 months after the surgery, the patient returned to our department for recurrent headache. CT of the paranasal sinuses demonstrated a remnant mass extending from the left suprabullar ethmoid cells along the skull base up to the anterior wall of the sphenoid sinus with compression of the medial orbital wall. There was no evidence of intracranial extension. The mass showed a clear rim of thickened bony structures. The central areas contained ground glass like calcifications (Figure 4A-C). Intraoperatively, the tumor was found to be closely located behind the agger nasi, extending from the floor of the frontal sinus dorsally along the anterior skull base up to the anterior wall of the sphenoid sinus. The lamina papyracea was intact. During the procedure, we found the upper part of the tumor and the anterior skull base could not be visualized under a 0-degree endoscope without dissection of agger nasi. Therefore, an endoscopic endonasal trans-agger nasi approach was performed for complete surgical removal of the tumor. The margins of the tumor were drilled off starting from the frontal sinus floor and going out posteriorly. After dissecting the superior part of the tumor, we observed that the anterior ethmoid artery traveled through the tumor. Therefore, electrocoagulation of the artery was done to minimize intraoperative bleeding. Then, an angled curette was used to further dissect the tumor in an extracapsular fashion. Finally, the surrounding bone of the resection bed was drilled until normal-appearing bone was seen. Postoperative CT images indicated that a gross total resection of the tumor was achieved (Figure 4D-F). Final pathology reported the diagnosis of juvenile psammomatoid ossifying fibroma. The patient's symptom of headache disappeared after the revision surgery and had no complications during the postoperative course. Nasal endoscopic evaluation showed completion of wound healing at 3-month post-operation (Figure 4G-H).
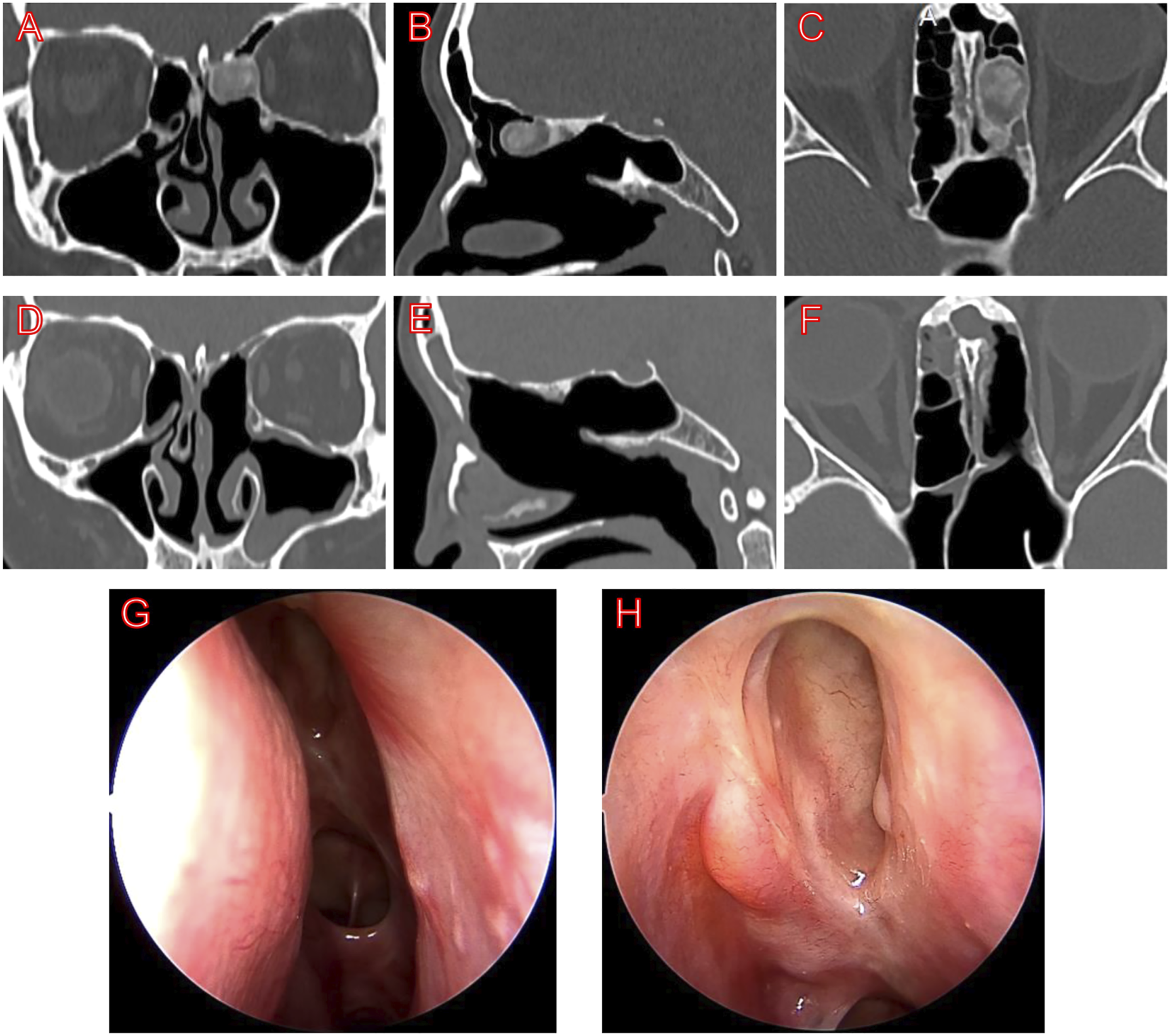
Preoperative and postoperative examination of case 2. (A–C) Preoperative CT images. (D–F) Postoperative CT images. (G-H) Postoperative nasal endoscopy at 3-month post-operation.
Discussion
Ossifying fibromas are benign fibro-osseous lesions characterized by a mixture of fibrous tissue and newly mineralized product being formed. They mainly occur in the bones of mandible and maxilla, but can rarely occur in the orbit, paranasal sinuses, and skull base.2,3 Generally, radical resection, especially gross total resection, is the most common recommendation whenever possible. Recent literatures have described the endoscopic transnasal approach and its variations for resection of the tumor, endorsing this method as a successful treatment for this benign lesion.5-7 However, it has been reported that the recurrence is common when partially or incompletely resected, with recurrence rates in the literatures ranging from 13.3 to 23%.6,7 The risk of recurrence is mainly influenced by the tumor locations, such as orbit and skull base, as well as the infiltration of residual tumor margins. Therefore, it is important to completely remove the tumor to prevent recurrence. In the present study, we present our experience with an endoscopic endonasal trans-agger nasi approach for the resection of ossifying fibroma involving anterior skull base, which has not been described previously. This approach affords direct access to the anterior skull base and the upper margin of the tumor by passing through the agger nasi, thus minimizing the risk of injury to the skull base.
In the case 2, the tumor was closely located behind the agger nasi, extending from the left suprabullar ethmoid cells along the skull base. During the procedure, we found the upper part of the tumor and the anterior skull base could not be visualized under a 0-degree endoscope without dissection of agger nasi. Therefore, we used the trans-agger nasi approach for the tumor resection with a forward-viewing endoscope (0-degree). Most of the anterior bone was dissected to fully expose the surgical field for tumor resection. For this case, an angled endoscope might provide a better visualization. However, spatial orientation usually becomes more challenging with an oblique-viewing scope, especially for the surgeons with less-experience. In addition, we believe that it is easier for surgeons to perform under a straight-on view in cases with lesions involving the skull base and rich of blood vessels.
There are several factors challenging the complete removal of the ossifying fibroma involving anterior skull base. First, it is difficult to identify the residual outer lamella of the tumor and its safety margins from the important surrounding structures. Specific attention should be given to avoid damaging the important anatomy structures, such as skull base and orbit, because damage of these structures would result in severe complications. Use of the image guidance system may help determine the boundary of the resection during procedures. Second, ossifying fibroma is often rich of high-flow blood sinus. In most cases, the major feeding vessel is the anterior or posterior ethmoid artery. Since preoperative embolization of these tumor-feeding arteries were impossible, and disruption of these vessel will increase the risk of operation and lead to a significant bleeding, rapid and proper control of the blood supply through the ethmoidal arteries is a key technical factor for successful resection of the tumor. Third, to minimize massive bleeding, it is recommended to remove the tumor as fast as possible to reach the border of tumor. However, in certain locations such as skull base and orbit, it is very difficult for the surgeon to peel off the bone shell. Based on our experience, in cases such as case 1 reported in the present study, the endoscopic endonasal trans-agger nasi approach could provide a direct access to the upper margin of the tumor under the 0-degree endoscope, thus facilitating the recognition of anterior skull base and identification of the safety boundary of the tumor. In cases such as case 2 we described, the trans-agger nasi approach could rapidly control the tumor-feeding vessel; therefore, help reducing intraoperative blood loss.
The trans-agger nasi approach, also termed the axillary flap approach, was originally designed by Wormald as a supero-lateral path to the frontal recess without the need of an angled endoscope. 10 This approach was developed based on the building block concept that the ethmoid air cells that crowd the frontal sinus ostium are re-constructed through a sequential cell-to-cell approach to determine the sinus drainage outflow. 15 This original approach provides adequate access to the frontal recess to easily clear the cells in the recess with an assistance of external incision or trephination of the frontal bone. Subsequently, variations of this endoscopic endonasal trans-agger nasi approach have been demonstrated in the endoscopic access to frontal recess and sinus for the removal of lesions of these areas.11-14 In the present study, we extended the previous works and found that this approach provided a direct access to the upper margin of the ossifying fibroma involving the anterior skull base with an effective vascular control, suggesting this technique is equally feasible for lesions along the anterior skull base.
There are several limitations in this study. First, although we share our experience with the endoscopic endonasal trans-agger nasi approach for resection of ossifying fibroma involving the anterior skull base, the technique described in our study needs to be compared with that executed through traditional approaches or methods in terms of outcome analysis, especially subsequent recurrence. Second, although the preliminary surgical outcomes in our study are promising, the only two cases argue for larger case series to validate the efficacy and reproducibility of this approach. Third, this approach may be only appropriate for selected lesions with tumor infiltration into orbit and skull base. If the operative space was insufficient, other approaches should be considered.
In summary, our preliminary experience demonstrated the safety and feasibility of the endoscopic endonasal trans-agger nasi approach for resection of selected cases of ossifying fibroma involving the anterior skull base. This approach offers a direct access to the anterior skull base and the upper margin of the tumor, facilitating recognition of the safety boundary of the tumor and rapid control of the tumor-feeding vessel.
Footnotes
Acknowledgments
We thank Ms. Yunping Deng from the Seventh Affiliated Hospital, Sun Yat-sen University for help follow-up of the patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This manuscript conformed to the standards of the Declaration of Helsinki. The Ethics Committee of the Seventh Affiliated Hospital of Sun Yat-sen University does not necessarily request the application of ethical approval for this type of manuscript.
Informed Consent
Written informed consent was obtained from all participants for publication.