
Abstract
Objective
To introduce a new method of preauricular fistula resection and discuss its clinical efficacy.
Methods
Clinical data of 40 patients with 40 classical preauricular fistulas in our hospital were collected. The patients comprised of 19 male and 21 female patients aged 3-60 years. The fistula and part of the related cartilage were completely removed by a concealed incision on the inner side of the auricular crus, and the opening of the fistula was retained. The postoperative efficacy was analyzed.
Results
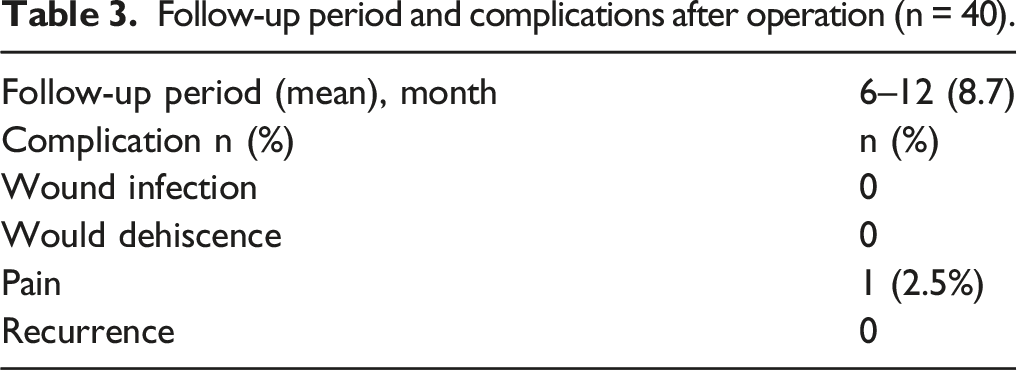
The operation time ranged from 15 to 30 minutes (mean, 25 minutes), and the blood loss ranged from 4 to 8 mL (mean, 5 mL). After complete fistula resection, the wound was closed with interrupted sutures. Dressing changes started 2 days after surgery and performed once a day, and the wound sutures were removed 7 days after surgery. All patients were followed up for 6 to 12 months (mean, 8.7 months) after surgery. Except for one patient with mild wound pain after suture removal, no patients developed infection or recurrence.
Conclusion
Use of a concealed surgical incision for treatment of a classical preauricular fistula has good results. There is no obvious scar on the ear after surgery and the procedure does not affect the facial appearance. It not only completely removes the lesion but also meets the patient’s esthetic needs.
Introduction
A congenital preauricular fistula is a relatively common congenital disease encountered in the clinical setting. Such fistulas can be clinically divided into classical and variant preauricular fistulas according to the distribution of the fistula mouth. 1 Most classical preauricular fistulas open in front of the auricular foot. If a classical preauricular fistula exhibits exudation of secretions accompanied by itching and discomfort around the fistula, and if no obvious abscess formation or rupture is present around the fistula, conservative treatment can be implemented. Timely surgical treatment is needed for patients with recurrent preauricular fistula infection. The traditional surgical approach is direct removal of the fistula and related cartilage in the tragus area, resulting in an obvious surgical scar. In this study, we adopted a new surgical approach in which a concealed incision was made inside the rising branch of the auricular foot to completely remove the fistula and related cartilage while preserving the opening of the fistula. This technique not only prevented itching, discomfort, and swelling around the ear but also met the patients’ esthetic, physiological, and psychological needs.
Patients and methods
The operative procedures and other data in this study are reported according to the STROBE guidelines. 2
Inclusion and exclusion criteria
The inclusion criteria were the presence of a classical preauricular fistula, agreement to undergo this new surgical approach and an ability to tolerate the surgery, and provision of informed consent and agreement to participate in the study. The exclusion criteria were the presence of a variant preauricular fistula, a history of preauricular fistula resection or incision and drainage of an abscess at the fistula, patient refusal to preserve the opening of the fistula, and refusal to provide consent for participation in the study.
General data
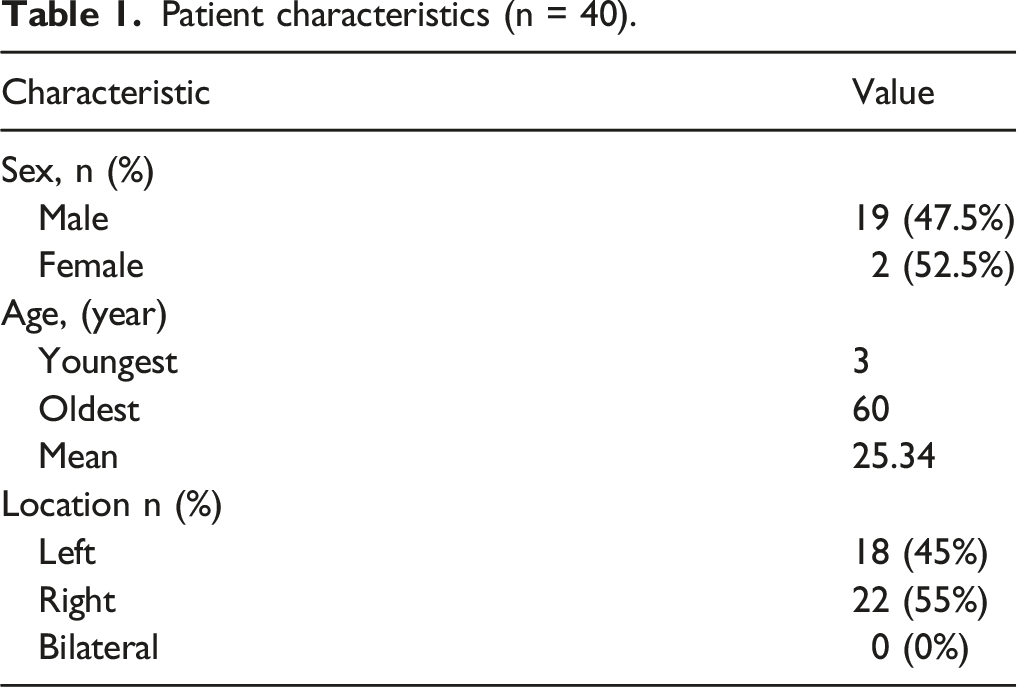
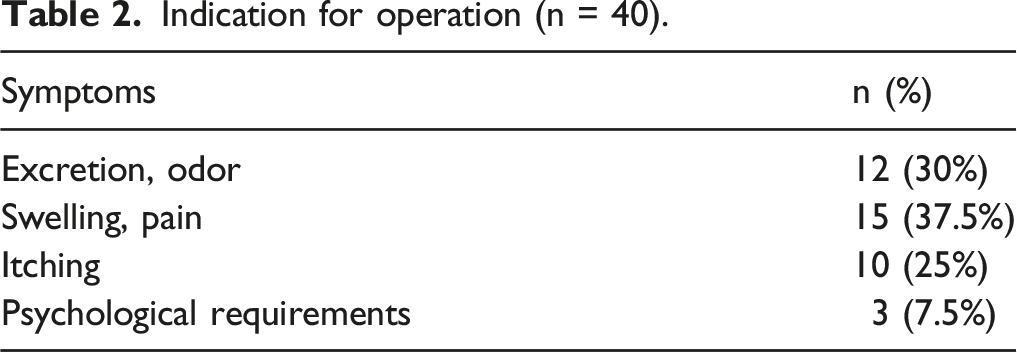
From April 2018 to April 2021, 52 patients with preauricular fistulas were admitted to our hospital. Of these, 40 eligible patients (Figure 1) were selected for inclusion in the study (Table 1). The patients’ clinical manifestations included itching around the fistula, leakage of secretions with an odor, swelling and pain around the fistula, and psychological disturbance related to the fistula (Table 2). STROBE flowchart. Patient characteristics (n = 40). Indication for operation (n = 40).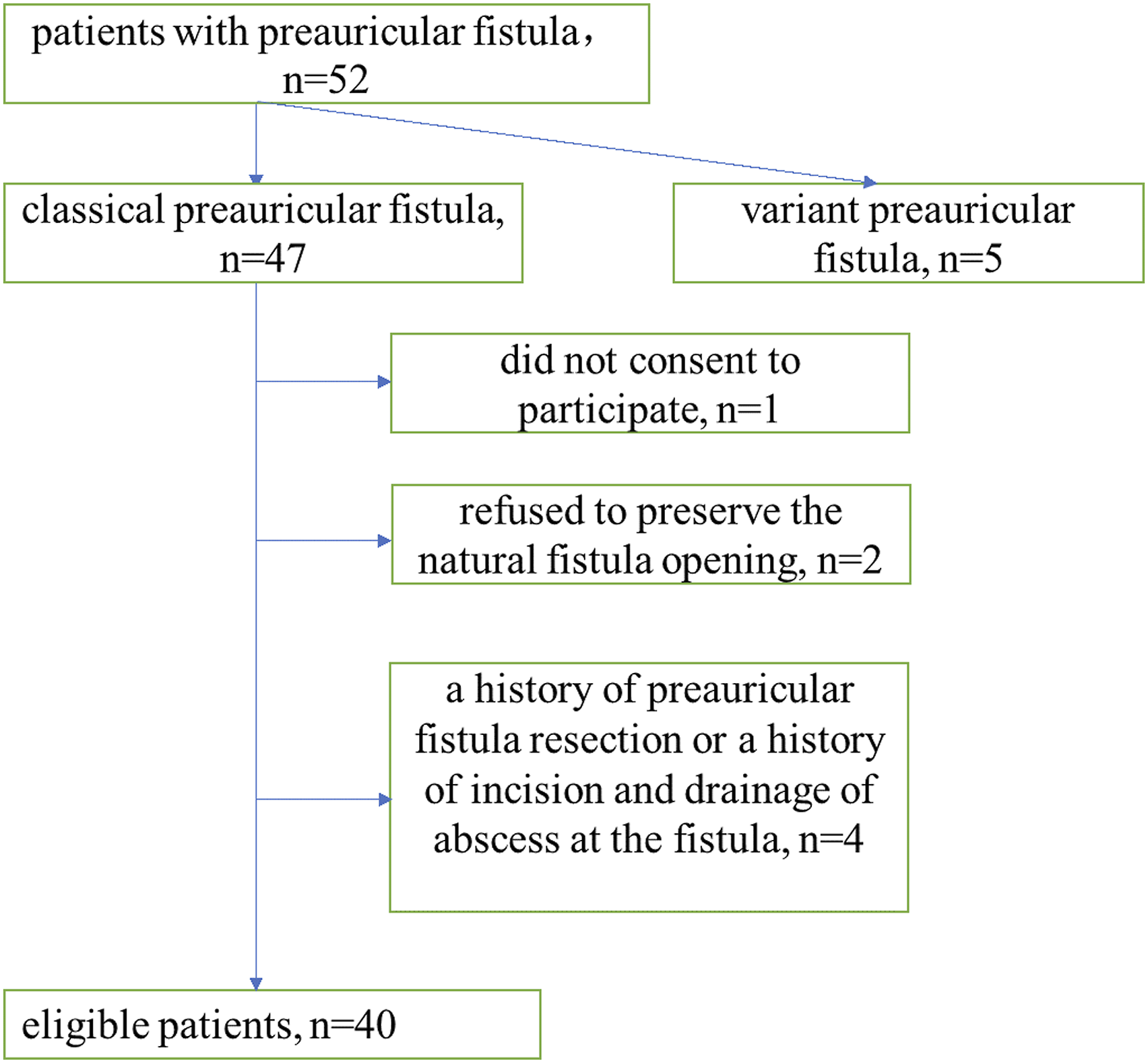
Methods
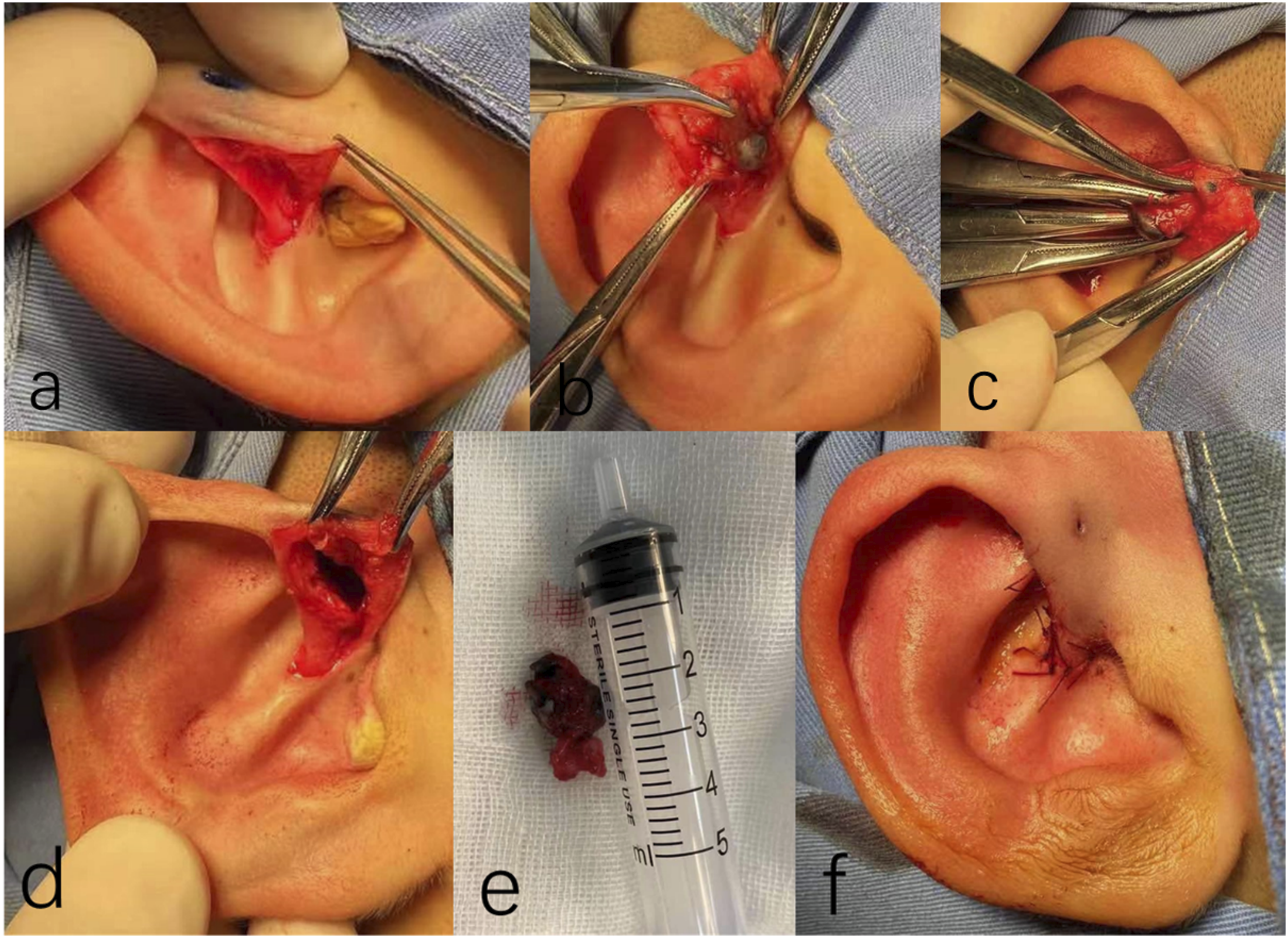
Methylene blue (0.1 mL) was injected along the fistula. An incision was made along the inner edge of the upwelling branch of the crus helix (Figure 2B), and the skin was lifted forward to the fistula (Figure 3A). The surrounding adhered tissue was stripped layer by layer along the stained fistula shape, and the fistula root was found to be located in the auricular cartilage (Figure 3B). The fistula and its attached cartilage (Figure 3E) were completely removed (Figure 3C) and sent for pathology. The tissue was very carefully exfoliated, and the operation was gently and precisely performed to prevent chondritis. The wound was then closed with 4-0 absorbable suture in an interrupted pattern, and erythromycin ointment was applied to prevent inflammation (Figure 3F). Images of a 16-year-old female patient. (A) Preauricular fistula opening. (B) Surgical incision. (A) Location of the intraoperative incision. (B) Exposure of the fistula. (C) Removal of the fistula. (D) Immediately after removal of the fistula. (E) Fistula and partial attached helix cartilage. (F) Appearance after suturing.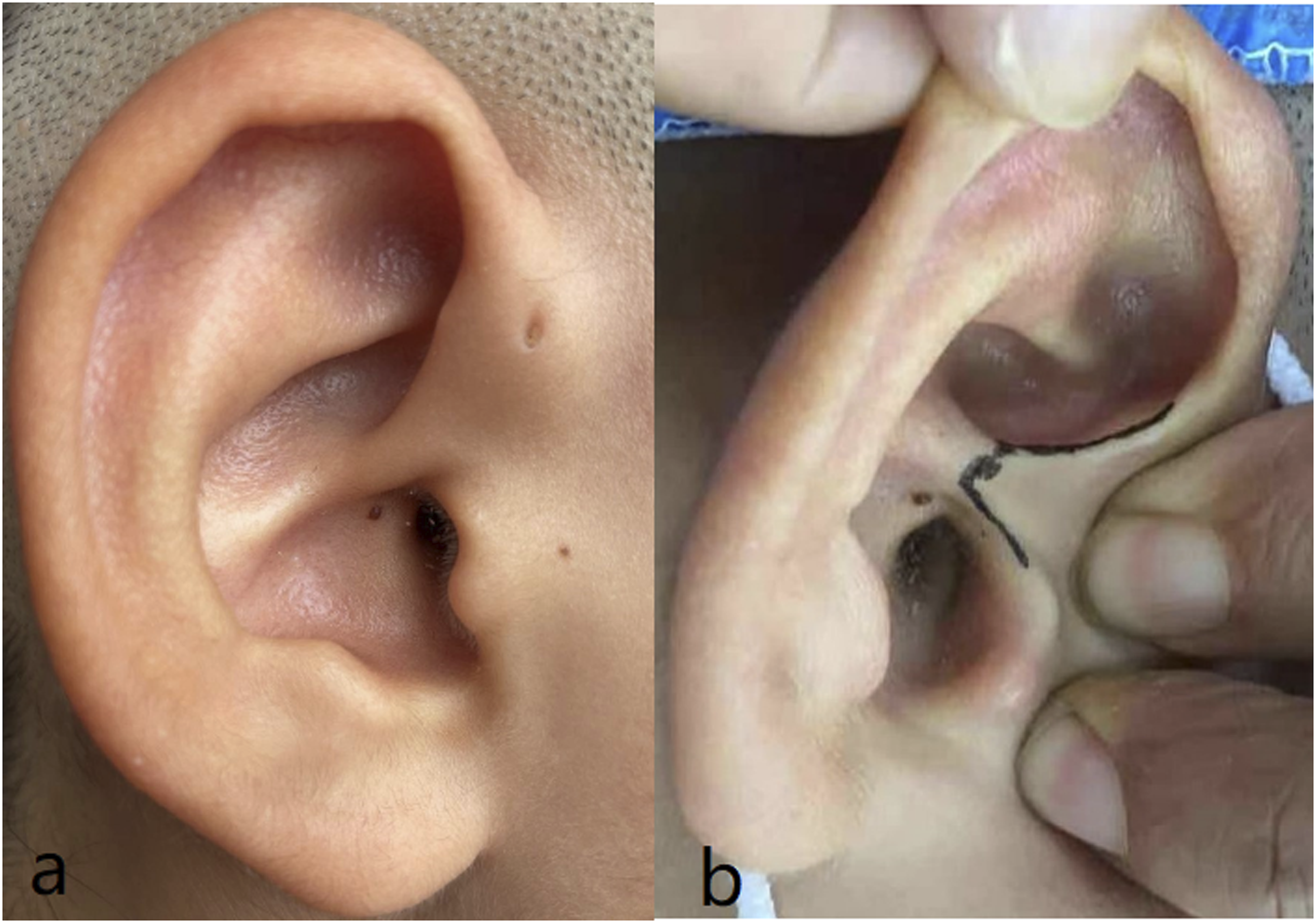
Results
The 40 patients (Figure 1) included in this study comprised 19 male and 21 female patients aged 3 to 60 years (mean, 25.34 years). The follow-up time ranged from 6 to 12 months (mean, 8.7 months) (Figure 4). Distribution of follow-up time in months.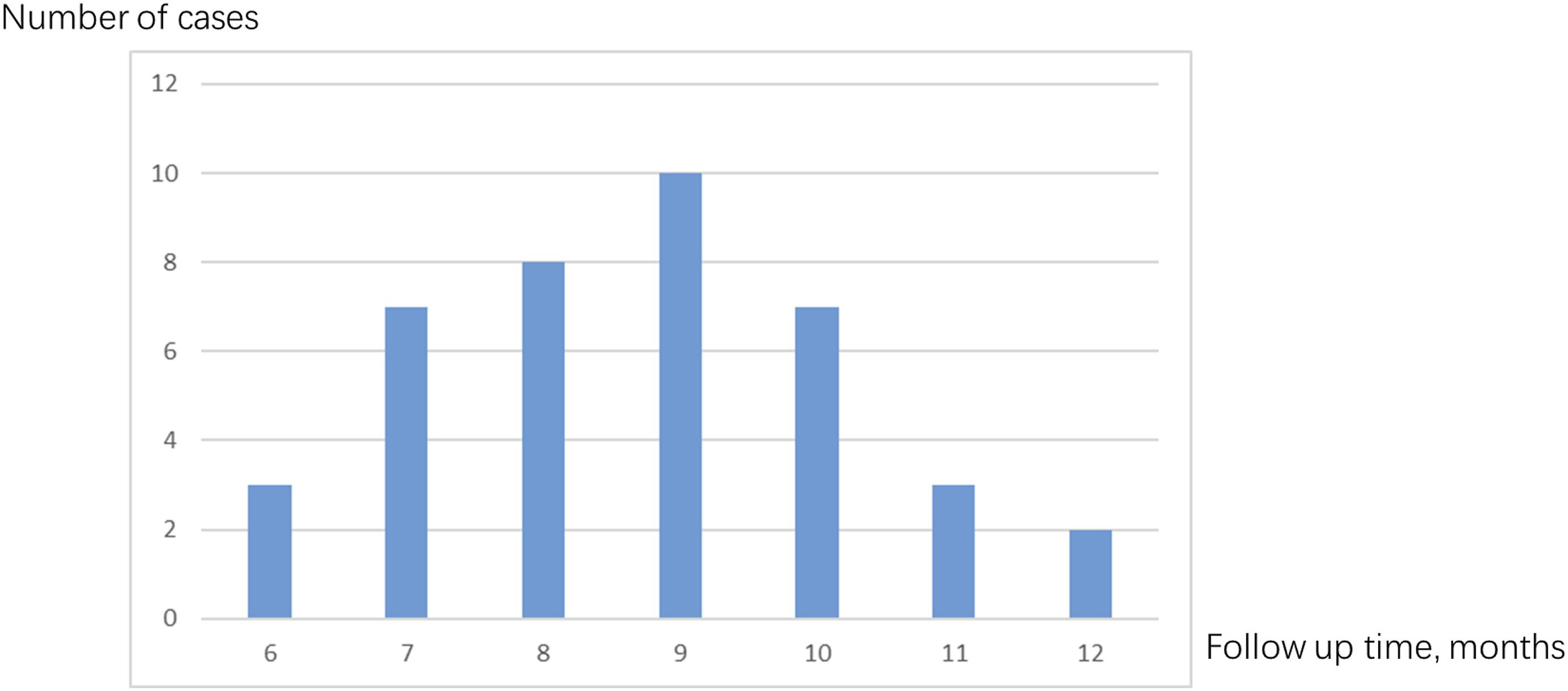
The dressing was changed 2 days after surgery (Figure 5A) and the sutures were removed 7 days after surgery (Figure 5B). There was no obvious scar formation in the postoperative incision and no change in auricle morphology (Figure 5C). No patients developed recurrence during follow-up (Table 3). (A) Two days after surgery. (B) Two weeks after surgery. (C) Four months after surgery. Follow-up period and complications after operation (n = 40).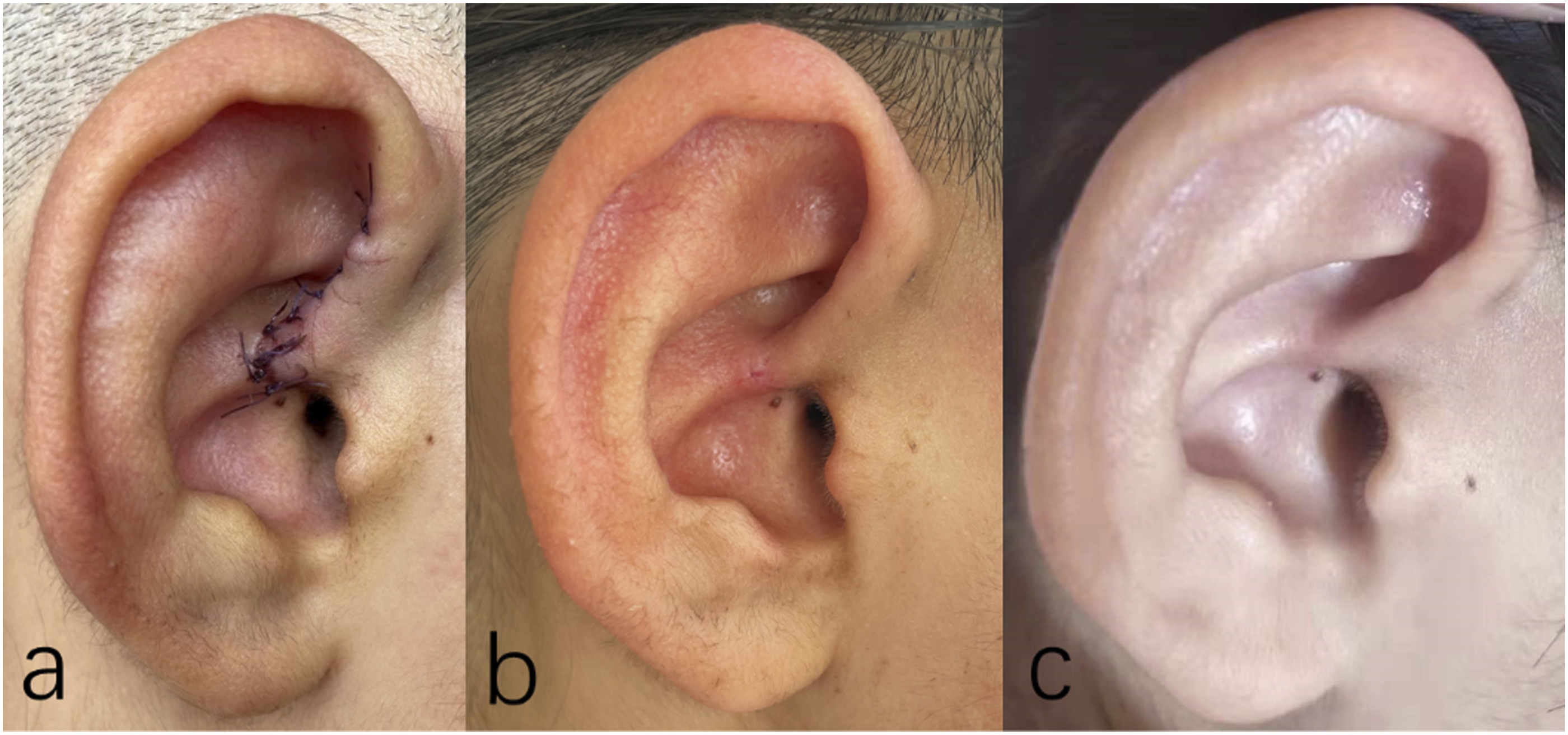
Discussion
With the progress of modern medicine, patients’ quality of life continues to improve. Additionally, because of patients’ psychological need to maintain their original appearance, the performance of plastic surgery in China has risen rapidly. Therefore, the scope of surgical treatment of preauricular fistulas has markedly expanded; surgery is not only performed on patients with obvious infection but also on patients with long-term periauricular swelling, pain, itching, and discomfort; fistula discharge overflow; odor; and other symptoms. Some patients develop recurrent fistula infection and discharge, and their symptoms are significantly improved after antibiotic treatment. Signs of worsening infection such as skin ulceration also often occur, placing serious economic and psychological burdens on the patient. Therefore, we have proposed a novel technique involving use of a concealed incision to meet patients’ increasing physiological and psychological needs.
A preauricular fistula, first described by Heusinger in 1865, is a common congenital disorder in childhood. Its incidence in Caucasians ranges from 0.1% to 0.9% and is higher among African and East Asian populations (4% and 10%, respectively). 3 Statistics show that the incidence of preauricular fistula varies among different countries. Its estimated incidence in the United States and Europe ranges from 0.1% to 0.9%, and in some African countries it ranges from 4% to 10% 3 ; the reported incidence is 1.91% in South Korea, 4 2.6% in Japan, 5 and 2.5% in Taiwan. 3 The difference in the incidence of preauricular fistula between sexes is controversial. Zhou Ping et al reported that the incidence of preauricular fistula was significantly higher in female than male patients, 6 whereas other studies have shown no significant difference between sexes. 7
The outer ear is embryologically formed from six hillocks of the first and second branchial arches. The preauricular sinus is the result of incomplete fusion of these interstitial colliculi. Therefore, preauricular fistulas are closely related to the cartilage of the tragus and the conicular, 8 and most of the fistula root is attached to the ear cartilage. 9 This is the anatomical basis for selection of the incision site for this concealed-incision surgery. Other rare locations reported in the literature include the upper and posterior ramus of the crus helix, auricle, and inner and posterior regions of the external auditory canal. 10 The incidence of variant preauricular fistulas is unknown, and prior to 2014, 11 only two reports described more than 10 cases. Therefore, classical preauricular fistulas account for the majority of preauricular fistulas, and our surgery is targeted at this fistula type.
Most patients with a preauricular fistula have no obvious symptoms. However, some patients develop abscesses or cellulitis around the fistula. 12 Although it is not necessary to treat asymptomatic patients, improper management of a fistula infection will lead to recurrence of the infection and severe postoperative scarring. 13 Recurrent or persistent preauricular fistula infection requires surgical resection during the quiescent phase of inflammation. 9
Traditional surgery 14 adopts a preauricular fusiform incision or double fusiform incision to remove the fistula and infected tissues, resulting in substantial surgical trauma, an obvious surgical scar, and a high recurrence rate. Recurrence rates reportedly range from 22% to 42%, 13 which may be due to the fact that multiple branches of the fistula are often missed during resection. In such cases, one of the most important factors affecting the treatment outcome is whether the surgeon has the means to identify and remove the distal branches of each fistula. This is more difficult in patients with a history of infection, which often leads to fibrosis and changes in the fistula shape. 15 In the postoperative follow-up of this study, all the patients’ ear incisions healed well without obvious scar hyperplasia, and the incisions were located inside the ascending ramus of the auricular foot without an obvious scar.
In the Chinese tradition, preauricular fistulas are sometimes informally referred to as an “ear storehouse” or “granary”: “The front storehouse stores grain, the back storehouse hides bran, and the ear edge hides clothes.” Many Chinese believe that preauricular fistulas symbolize wealth and that facial features herald personal fate. These people are often averse to surgery to alter their facial features. The herein-described operation satisfies their psychological need to retain the “ear storehouse.”
Our study has some limitations. The number of cases in this study was small, and information on recurrence and complications was often obtained through follow-up at least 1 year after surgery. Therefore, the follow-up time in our study was too short to record the recurrence rate and related complications. Additionally, this study excluded patients with severe infection, skin ulceration, or scar formation, and we did not perform the concealed incision on these patients; therefore, we could not determine whether this procedure is appropriate for such patients. In the future, longer follow-up and expanded surgical indications will be implemented to further investigate the applicability and merit of this method for the treatment of preauricular fistulas.
Conclusion
Use of a concealed surgical incision for the treatment of classical preauricular fistulas has good results. There is no obvious scar on the ear after surgery and the procedure does not affect the facial appearance. It can not only completely remove the lesion but also meets the patient’s esthetic needs.
Footnotes
Acknowledgement
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the ethics committee of our hospital. Grant Number: ChiCTR1801020117.
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.