
Abstract
Basal cell carcinoma (BCC) is the most common non-melanocytic skin cancer. 1 The American Cancer Society estimated that in 2006, more than 2 million people were treated for non-melanoma skin cancers, most of which were BCCs. Ultraviolet (UV) exposure is the most critical risk factor for BCC. 2 Mazeron et al. reported the distribution of BCC according to nose regions; BCC occurred mainly at the external nose, such as at the ala (26%), upper lateral surface (18%), tip (15%), nasolabial fold (13%), bridge (12%), root (11%), and columella (1%). However, BCC of the nasal vestibule (0.01%) is extremely rare. 3 The nasal vestibule is a distinct triangular space located in front of the limen nasi, which is covered by squamous epithelium. The border of the vestibule is the alar, supporting the lower lateral cartilage laterally, the membranous septum and columella medially, and the floor of the nasal cavity caudally. This area is usually not exposed to UV radiation, and malignant tumors of the nasal vestibule are primarily squamous cell carcinomas. 4 Conventional surgical excision or Mohs surgery could be performed for the treatment of facial BCC. We presented an unusual case of BCC at the nasal vestibule treated with surgical excision using a skin graft.
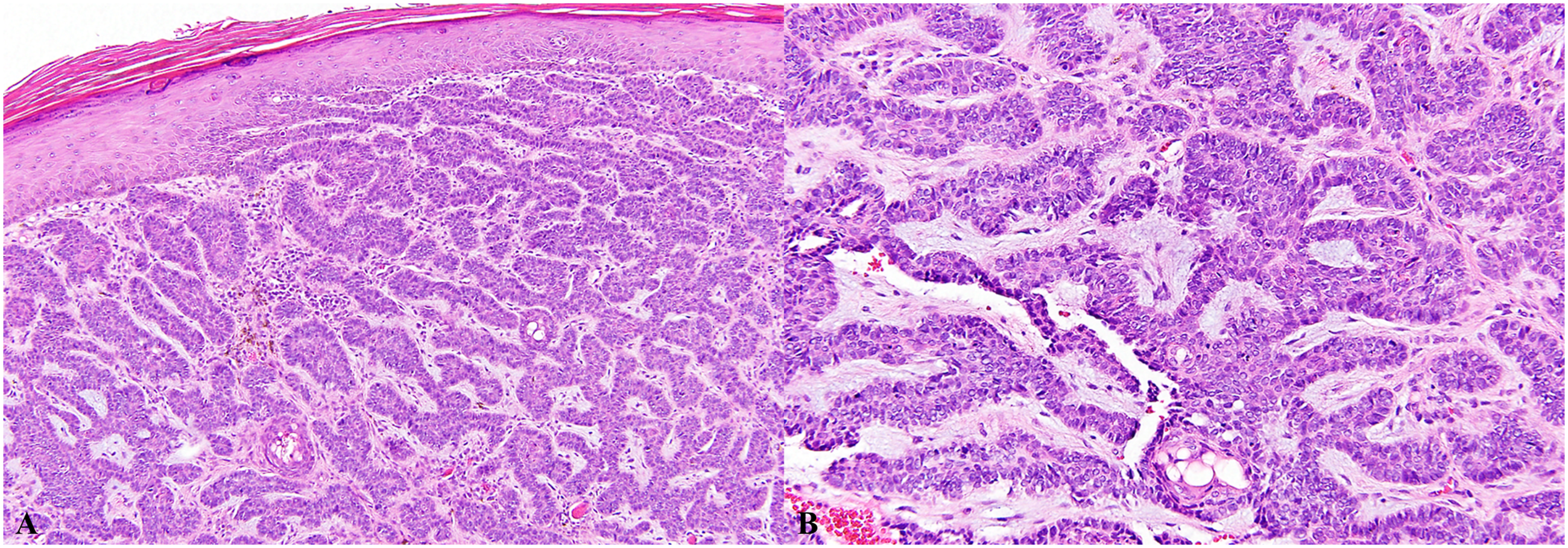
A 49-year-old man was referred to our hospital with a 5-month history of a granulomatous mass on the right nasal vestibule (Figure 1). He denied having any other nasal symptoms, such as nasal obstruction, rhinorrhea, pain, and epistaxis. On physical examination, a rubbery hard mass measuring approximately 1 cm was noted at the right nasal vestibule. An incisional biopsy was performed under local anesthesia. Microscopic examination revealed tightly packed tumor cell nests, clearly showing an epidermal origin (Figure 2A). The tumor cells had indistinctive cytoplasmic borders and peripheral palisading with a surrounding fibro-mucinous stroma (Figure 2B). These findings confirmed the presence of BCC. Oval-shaped mass on the right nasal vestibule. (A) Microscopic examination reveals tightly packed tumor cell nests clearly showing an epidermal origin (hematoxylin and eosin, original magnification 100×). B. The tumor cells have indistinctive cytoplasmic borders and peripheral palisading with a surrounding fibro-mucinous stroma (hematoxylin and eosin, original magnification 200×).
Wide surgical excision was performed around the tumor, including normal tissue, and the medial side of the lower lateral cartilage was partially exposed after tumor removal. Frozen biopsy was performed to check for tumor invasion at the tumor resection margin. After confirming negative tumor margins in all directions, including in the tumor bed (Figure 3A), a full-thickness skin graft from the right ear skin was used at the defect site. The tumor size was approximately 1.0 × 0.7 cm, and permanent pathological evaluation confirmed BCC; no resection margin involvement was noted. At the 5-year follow-up post-surgery, there was no evidence of recurrence and there were no cosmetic problems (Figure 3B). (A) Surgical defect after wide excision of vestibule BCC. (B) Clinical photographs taken 5 years after surgery.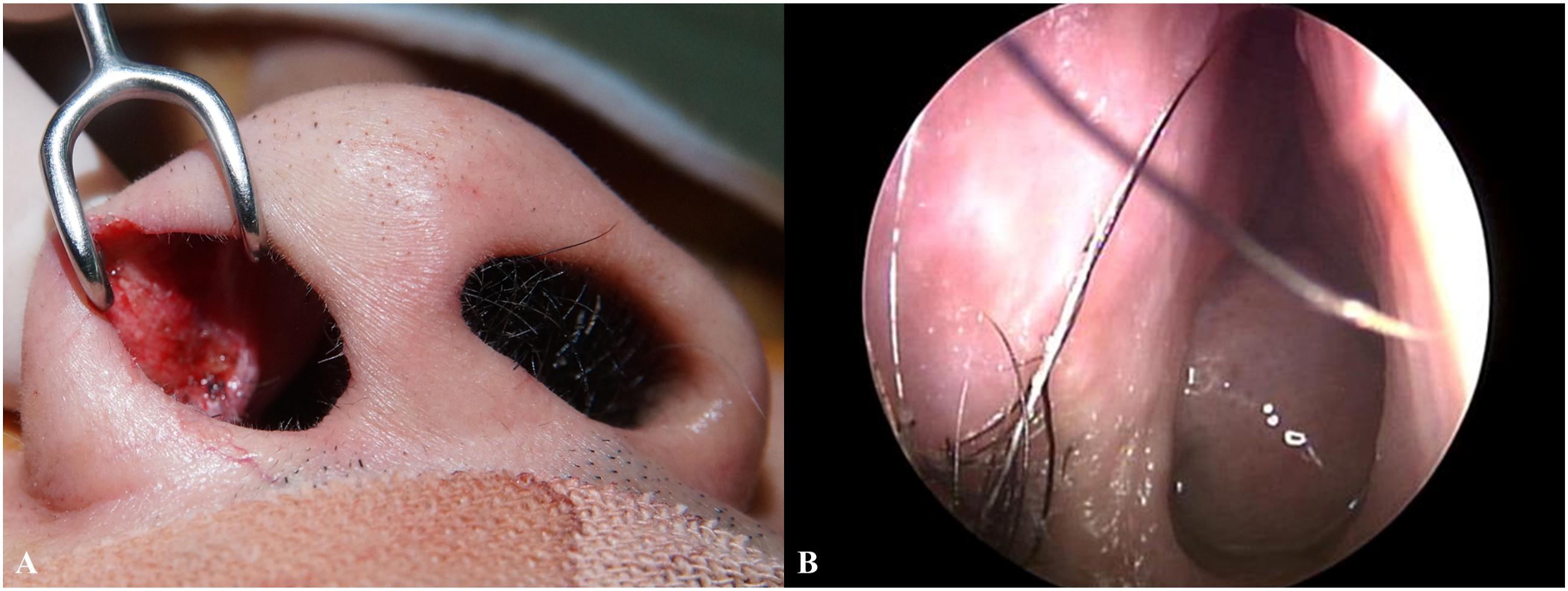
The incidence of BCC continues to increase worldwide due to increasing solar UV exposure and population aging. 2,5 Approximately 80% of all BCCs occur in the head and neck area; of these, 25–30% are found on the nose. 2,6 Common sites on the nose are the nose tip, upper lateral surface, and ala nasi. Less than 1% of BCCs on the nose develop on the nasal vestibule. 2,3 The differential diagnoses include premalignant lesions such as actinic keratosis and keratoacanthoma and malignant tumors such as melanoma and squamous cell carcinoma. 6
Excision with an adequate margin is suggested as the treatment of choice. The treatment goal for BCC is to completely resect the tumor and preserve function and cosmesis. Various surgical and medical therapies are available for BCC treatment. Surgical excision is commonly performed for lesions that are not at an advanced stage. Other less frequently used treatments include topical 5-fluorouracil (5-FU) or imiquimod, cryosurgery, intralesional injection, photodynamic therapy, and Mohs surgery. Radiation therapy is another option if surgery is contraindicated or resection margins are positive. 4,5,7
Wollina et al. reported that surgical excision of BCC of the nose showed a 2.5-times higher recurrence rate than that of BCCs at other locations. 2 This may be because the nose is a specialized structure in the center of the face, with three-dimensional contours, and is composed of bone and cartilage. In addition, the nose and its underlying nasal cavities form an essential part of the airway. 3 Therefore, preservation of the nose or reconstruction of the nose after tumor resection is essential for cosmetic and functional reasons. Reconstruction with a graft or local flap is often required for BCC of the nose. 5 Therefore, Mohs surgery is indicated for lesions with an increased risk of recurrence and in cases where functional and anatomic relations need to be preserved. 7
However, surgical excision could be a definitive treatment, with careful examination of tumor involvement in the resection margin through frozen biopsy during surgery. 1,8 Previous studies have compared surgical excision and Mohs micrographic surgery for primary and recurrent BCC of the face. For primary BCC, the recurrence rates were 4.1% and 2.5% in patients treated with surgical excision and Mohs surgery, respectively. For recurrent BCC, the recurrence rates were 12.1% and 2.4% in patients treated with surgical excision and Mohs surgery, respectively. Mohs surgery is preferred over surgical excision for the treatment of recurrent facial BCC. However, considering that there was no significant difference in the recurrence of primary BCC between the treatment groups, surgical excision is probably sufficient in most cases of primary BCC. 9 In our case, a full-thickness skin graft harvested from the right ear skin was used. Also, a septal mucosal advancement flap could be used for the defect. 10
Significance Statement
We reported a rare case of basal cell carcinoma of the nasal vestibule treated with excision and a full-thickness skin graft. Surgical excision without radiation therapy is available because the surgical margin is sufficient for excision. Moreover, verifying tumor invasion via frozen biopsy during surgery is extremely important for ensuring sufficient surgical margins.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board of Jeju National University Hospital approved this study.